

Abstract
We present a rare case of adenocarcinoma arising from a heterotopic pancreas in the duodenum, and review the associated literature. A 62-year-old woman was admitted to our hospital, complaining of vomiting and epigastralgia. Imaging studies revealed advanced gastric cancer with a gastric outlet obstruction. Whipple's operation and resection of the regional lymph node were performed because of a direct invasion to the pancreas. Histopathologic examination of the resected specimen demonstrated the malignant transformation of a hetrotopic pancreas in the duodenum. At the 12-month follow-up, there was no recurrence of symptoms. The prognosis of adenocarcinoma arising from a heterotopic pancreas is not known. Further accumulation of cases and investigation of this entity are necessary.
Keywords: Heterotopic pancreas, Adenocarcinoma, Duodenum, Gastric outlet obstruction
Heterotopic pancreas has been defined as the presence of pancreatic tissue that is not normally situated and has no anatomic or vascular connection with the pancreas proper.1 Heterotopic pancreas is considered to result from the alteration of embryonic growth, whereby a part or all of the ventral anlagen of the primitive pancreas was left behind in the foregut.2 The manifestations and complications of heterotopic pancreas include acute or chronic pancreatitis and cystic degeneration.3,4 However, the malignant transformation of heterotopic pancreas is extremely rare. We report a rare case of this entity in the duodenum, with a review of the literature.
Case Report
A 62-year-old woman was admitted to our hospital, complaining of vomiting and epigastralgia. She had no history of note, and a physical examination revealed no specific findings. Results of laboratory tests were within the normal limits. Serum tumor markers were as follows: carcinoembryonic antigen, 8.1 ng/mL (normal range, <6.0 ng/mL); carbohydrate-associated antigen19-9, 66.9 U/mL (normal range, <37 U/mL). Gastrointestinal endoscopy disclosed gastric outlet obstruction (Fig. 1a). The biopsy specimen obtained from a stenotic site revealed regenerative gastric mucosa without malignancy. A duodenal contrast study showed stenosis of the pyloric ring with dilatation of the duodenal bulb (Fig. 1b). Abdominal computed tomography (CT) demonstrated a heterogeneously enhanced mass of 1.8 × 1.4 cm in the pyloric ring (Fig. 2a). Under a diagnosis of advanced gastric cancer in the pyloric region, open surgery was carried out, revealing that the tumor had infiltrated into the pancreas. Therefore, Whipple's operation and resection of the regional lymph node were performed.
Fig. 1 .

a. Gastrointestinal endoscopic examination disclosed a gastric outlet obstruction (arrow). 1b. A duodenal contrast study showed stenosis of the pylorus ring with dilatation of the duodenal bulb.
Fig. 2 .

a. An abdominal computed tomogram (CT) demonstrated a heterogeneously enhanced mass of 1.8×1.4 cm in the pylorus ring (arrow). 2b. Magnetic resonance cholangiopancreatography (MRCP) presented no abnormal findings.
Upon macroscopic examination, the specimens showed a solid submucosal tumor that had infiltrated through the full thickness of the duodenum, measuring 12 × 34 mm. Histologic examinations demonstrated the heterotopic pancreatic tissue composed of exocrine acini, small ducts, and islets of Langerhans, detected within the proper muscular layer at the periphery (Heinrich type I).5 The tumor cells had swollen and variously sized nuclei; furthermore, the tumor cells infiltrated diffusely with fused ducts or small foci in an area ranging from the submucosal layer to the proper muscular layer. A diagnosis of moderately differentiated tubular adenocarcinoma arising from a heterotopic pancreas in the duodenum was made (Fig. 3). Extensive perineural invasion was present, but focal lymphovascular invasion was absent. The regional lymph nodes were free from metastasis (0/51). The patient's postoperative course was uneventful, and she was discharged on postoperative day 26. At the 12-month follow-up, there was no recurrence of symptoms or on imaging.
Fig. 3 .

a. Nonneoplastic heterotopic pancreatic tissue (arrow) was present within the submucosal and proper muscular layer of the duodenum. 3b. Heterotopic pancreatic tissue is composed of complete structures consisting of ducts (arrowhead), acini (white arrow), and islets of Langerhans cells (arrow) (Heinrich classification; Type I). 3c. Direct transitions between the normal pancreatic structures (arrow) and the carcinoma (arrowhead) were observed. 3d. The histological type was moderately differentiated tubular adenocarcinoma.
Discussion
Shultz first described heterotopic pancreas in 1727.6 Subsequently, Klob described 2 cases of histologically confirmed heterotopic pancreas in 1859.7 In recent studies, it has been reported to be in 0.6% to 13% of autopsies.2,8 Although heterotopic pancreas can be found throughout the entire gastrointestinal tract, the most frequent sites are the organs near the pancreas such as the stomach (25%–60%), duodenum (30%), and jejunum (15%), because this entity has been thought to be due to a failure of the fusion in the 2 primitive pancreas.7 Clinical symptoms caused by this entity are rather infrequent unless it is accompanied with size-up, bleeding, or concomitant pathologic changes. Furthermore, malignant transformation in the heterotopic pancreas is exceedingly rare. To our knowledge, only 9 cases of adenocarcinoma arising from heterotopic pancreas in the duodenum have been documented worldwide.9–17
We summarized these clinicopathologic features, along with our case, in Table 1. The patients ranged in age from 28–72 years. It is impossible to make a preoperative determination that a carcinoma has arisen from a heterotopic pancreas. There has been no such case in previous reports. To confirm the malignant transformation of a heterotopic pancreas, the following three criteria must be met: (1) the tumor must be found within or close to the heterotopic pancreatic tissue; (2) direct transition between pancreatic structures and the carcinoma must be observed. Malignant transformation of the heterotopic pancreas must be differentiated from the metastatic lesion or direct invasion from a neighboring digestive cancer; and (3) the nonneoplastic pancreatic tissue must comprise at least fully developed acini and ductal structures.18 Our case was compatible with these criteria from the postoperative histologic examination. Histologic types of previously reported cases were as follows: well-differentiated tubular adenocarcnima, 1 case; moderately differentiated tubular adenocarcnima, 1 case; poorly differentiated tubular adenocarcinoma, 1 case.
Table 1 .
Summary of the reported cases
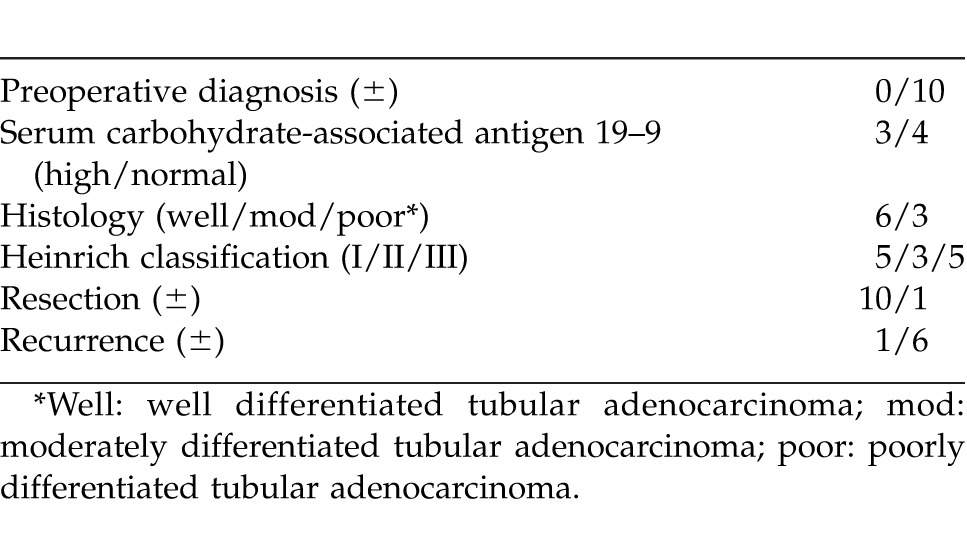
Heterotopic pancreas has been classified into three types according to the histologic components (Heinrich classification).5 Type I is composed of complete structures consisting of ducts, acini, and islets of Langerhans cells. Type II is composed of ducts and acini. Type III is composed of ducts only. In a cumulative review of the literature, type I comprised 2 cases, type II 2 cases, and type III 3 cases.
With regard to the management and prognosis, radical resections including distal gastrectomy and Whipple's operation were performed in all 5 reported patients. The prognosis of patients with adenocarcinoma arising from a heterotopic pancreas is not known. However, in the literature, only 1 case developed recurrence during follow-up periods from 16 months to 6 years. These facts suggest that radical resections for adenocarcinoma arising from a heterotopic pancreas may lead to a better prognosis than that for ordinary pancreatic cancer.
In conclusion, we have described a case of adenocarcinoma arising from a heterotopic pancreas in the duodenum. This entity is an extremely rare disease, and diagnosing it preoperatively is difficult. Further accumulation of cases and investigation of this entity are necessary.
References
- 1.Dolan RV, ReMine WH, Dockerty MB. The fate of heterotopic pancreatic tissue. A study of 212 cases. Arch Surg. 1974;109:762–765. doi: 10.1001/archsurg.1974.01360060032010. [DOI] [PubMed] [Google Scholar]
- 2.Tolentino LF, Lee H, Maung T, Stabile BE, Li K, French SW. Islet cell tumor arising from a heterotopic pancreas in the duodenal wall with ulceration. Exp Mol Pathol. 2004;76:51–56. doi: 10.1016/j.yexmp.2003.08.005. [DOI] [PubMed] [Google Scholar]
- 3.Jarry J, Jr, Rault A. Sa Cuhna A, Collet D, Masson B. Acute recurrent pancreatitis by heterotopic fundic mucosa at the ampulla of vater. Pancreas. 2009;38:351–353. doi: 10.1097/MPA.0b013e3181888feb. [DOI] [PubMed] [Google Scholar]
- 4.Rebours V, Lévy P, Vullierme MP, Couvelard A, O'Toole D, Aubert A, et al. Clinical and morphological features of duodenal cystic dystrophy in heterotopic pancreas. Am J Gastroenterol. 2007;102:871–879. doi: 10.1111/j.1572-0241.2007.01091.x. [DOI] [PubMed] [Google Scholar]
- 5.von Heinrich H. Ein Beitrag zur Histologie des sogen akzessorischen Pankreas. Virchows Archiv Pathol Arat Bd. 1909;198:392–401. [Google Scholar]
- 6.Elfbing G, Hastbacka J. Pancreatic heterotopias and its clinical importance. Acta Chir Scand. 1965;130:593–602. [PubMed] [Google Scholar]
- 7.Barbosa DE, Castro JJ, Dockerty MB, Waugh JM. Pancreatic heterotopias: review of the literature and report of 41 authenticated surgical cases, of which 25 were clinically significant. Surg Gynecol Obstet. 1946;82:527–542. [PubMed] [Google Scholar]
- 8.Jiang LX, Xu L, Wang XW, Zhou FR, Gao W, Yu GH, et al. Gastric outlet obstruction caused by heterotopic pancreas: a case report and a quick review. World J Gastroenterol. 2008;14:6757–6759. doi: 10.3748/wjg.14.6757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bookman MR. Carcinoma in the duodenum: originating from aberrant pancreatic cells. Ann Surg. 1932;95:464–467. doi: 10.1097/00000658-193203000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Potet F. Cystic dystrophy on aberrant pancreas of the duodenal wall. Arch Fr Mal App Dig. 1970;59:223–238. [PubMed] [Google Scholar]
- 11.Legel L. Heterotopic pancreas. Report of 8 new cases [in French] J Chir (Paris) 1979;116:553–560. [PubMed] [Google Scholar]
- 12.Al Jitawi SA, Hiarat AM, Al-Majali SH. Diffuse myoepithelial hamartoma of the duodenum associated with adenocarcinoma. Clin Oncol. 1984;10:289–293. [PubMed] [Google Scholar]
- 13.Franke U, Hartmann F, Heitland W, Dolle W. Malignant transformation of ectopic pancreas. An unusual cause of acquired duodenal stenosis with cholestasis in a 26-year-old patient. Internist (Berl) 1989;30:525–527. [PubMed] [Google Scholar]
- 14.Nam JY, Lee SI, Chung JP, Choi SH, Lee DY, Choi JP, et al. A case of duodenal adenocarcinoma arising from the heterotopic pancreas. Korean J Gastroenterol. 2003;42:164–167. [PubMed] [Google Scholar]
- 15.et al. Cystic dystrophy of the duodenal wall developing in heterotopic pancreas: report of 9 cases. Pancreas. 2007;34:152–156. doi: 10.1097/01.mpa.0000246669.61246.08. Tison C Reqenet N, Meurette G, Mirallie E, Cassaqnau E, Frampas E. [DOI] [PubMed] [Google Scholar]
- 16.Inoue Y, Hayashi M, Arisaka Y, Higuchi K, Egashira Y, Tanigawa N. Adenocarcinoma arising in a heterotopic pancreas (Heinrich type III): a case report. J Med Case Reports. 2010;4:39. doi: 10.1186/1752-1947-4-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bini R, Voghera P, Tapparo A, Nunziata R, Demarchi A, Capocefalo M, et al. Malignant transformation of ectopic pancreatic cells in the duodenal wall. World J Gastroenterol. 2010;16:1293–1295. doi: 10.3748/wjg.v16.i10.1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Guillou L, Nordback P, Gerber C, Schneider R. Ductal adenocarcinoma arising in a heterotopic pancreas situated in a hiatal hernia. Arch Pathol Lab Med. 1994;118:568–571. [PubMed] [Google Scholar]