

A 48 year old male known to have controlled essential hypertension, untreated dyslipidemia, and a heavy smoker presented with retrosternal atypical chest pain intermittent in nature. His serial Troponins were negative and resting 2D echocardiography study did not show any segmental wall motion abnormality; exercise stress test reproduced his chest pain at 6 METS with 2 mm ST depression in the inferolateral leads. Coronary CT study showed calcification in the mid and distal parts of the left anterior descending artery (LAD) (Fig. 1) with mixed plaque type causing approximately 40% stenosis with impressive vessel remodeling in that area; also it revealed a filling defect within the coronary artery lumen with contrast around that defect and an absence of calcium within the defect. In addition the defect had classically low attenuation (50 Hounsfield units) which makes it very likely an acute thrombus of LAD (Fig. 2 and zoomed view in Fig. 3) indicating most likely acute plaque with thrombus formation; the rest of the coronary tree did not show any other significant pathology (Fig. 4). The patient refused hospital admission and was treated with dual anti-platelet therapy and low molecular weight heparin (lmwh) and his symptoms resolved.
Figure 1.
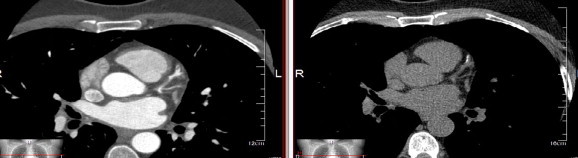
Evidence of calcification at the site of the filling defect.
Figure 2.

Multiplanar reconstructed image of LAD showing a filling defect in the lumen after origin of second diagonal branch.
Figure 3.

Zoomed view of the filling defect showing a stalk connecting it to the anterior wall of the vessel with evidence of underlying soft plaque with positive remodeling.
Figure 4.
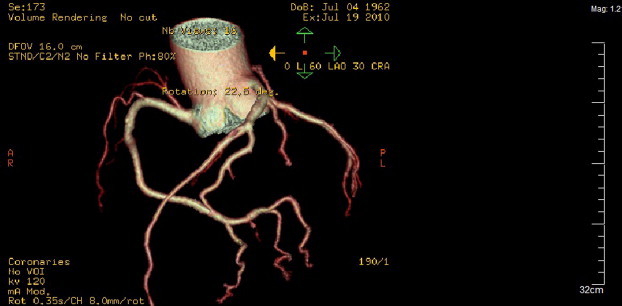
Volumetric rendering technique showing the filling defect in LAD and no other obstructive disease in the rest of coronary tree.
Coronary thrombi commonly happened after a plaque rupture in non-obstructive coronary plaque especially mixed type (Kramer et al., 2010) which is caused by rupture of thin fibrous cap on the atherosclerotic plaque core which forms the clot, but there are other causes such as dissection, hypercoagulable state, and emboli (Slim, 2010).
References
- Kramer M.C.A., Rittersma S.Z.H., de Winter R.J. Relationship of thrombus healing to underlying plaque morphology in sudden coronary death. J. Am. Coll. Cardiol. 2010;55(2):122–132. doi: 10.1016/j.jacc.2009.09.007. [DOI] [PubMed] [Google Scholar]
- Slim, Ahmad M., 2010. Coronary thrombus detected by cardiac CT angiography before cardiac catheterization. J. Thorac. Imaging. doi:10.1097/RTI.0b013e3181ced163 (Epub ahead of print, post-author corrections 11.05.2010). [DOI] [PubMed]