

Abstract
Background:
Unsafe injection practices are common in developing nations. Such practices, through contaminated needles and syringes, place injection recipient, healthcare workers and the community at large at risk of infection with blood borne viruses.
Aim:
An attempt was made to briefly describe an acute hepatitis outbreak that occurred in Gujarat, India, due to unsafe injection practices with a brief review of the literature.
Subjects and Methods:
An outbreak of acute hepatitis occurred in February-March 2009 in the Sabarkantha district of Gujarat in India. Blood samples were collected randomly from 25 cases, admitted in the local hospital during the ongoing outbreak. Screening was done using an immunoassay analyzer (Cobas e411; Roche Diagnostics, Indianapolis, IN, USA) for hepatitis B surface antigen (HBsAg), IgM and total antibodies to hepatitis B core antigen (HBc), hepatitis B e antigen (HBeAg) and antibody to HBe, antibodies to HCV, HIV and IgM antibodies to hepatitis A virus (HAV), as per the manufacturer's protocol.
Results:
Gross and continuous use of contaminated needle and syringes were responsible for this outbreak as all the patients gave history of receiving injections about 2-3 months prior to the development of clinical signs and symptoms, from one particular doctor. Mean age of the patients was 33.4 years (SD 12.9 years). Seventeen of these patients were males and eight were females. All patients were hepatitis B surface antigen positive, with median levels as 35,450 IU/mL (IQR 450-2,49,750 IU/mL). IgM HBc was positive in 22/25 (88%). HBe Ag was positive in 11 patients (44%). The median HBV DNA level was 2.6 × 104 IU/mL (IQR 1.18 × 102 to 6.7 × 106 IU/mL). No significant co-infection with other hepatitis viruses existed. All isolates were genotype D.
Conclusions:
The findings emphasize the role of unsafe injection practices in the community outbreak of hepatitis B infection, need to start routine surveillance system and increase awareness in health care workers regarding safe injection practices.
Keywords: Acute hepatitis B, Outbreak, Unsafe injections
Introduction
Injections are the most commonly used medical devices in health care settings. As per the World Health Organization (WHO) estimates, approximately 16 billion injections are given annually worldwide, most of them for therapeutic purposes and a very few for immunizations. Unsafe injection practices like needle and syringe reusage, along with unnecessary use of injections, are quite common, especially in the developing world. These are responsible for transmission of blood borne viruses (BBV) in healthcare workers (HCW) and the community at large, thereby posing a major public health problem. It is estimated that up to 160,000 human immunodeficiency virus (HIV), 4.7 million hepatitis C virus (HCV) and 16 million hepatitis B virus (HBV) infections are attributable each year to such unsafe injection practices.[1,2] In India, this problem is complex and multifactorial due to the lack of awareness, social commitment and lack of availability of sufficient resources in health care settings. Previously, outbreaks of BBVs, especially HBV, due to contaminated needle and syringes have been reported from India.[3,4] This problem is quite intense in the rural areas. Although many studies have pinpointed the prevalent unsafe injection practices existing in our country,[5] a recent study highlighted the alarming situation of unsafe injection practices in the Gujarat state of India.[6] The study revealed that 77% of service providers had unsafe injection practices; the proportion was higher among the Government health sector. Despite this, one of the largest epidemics of acute hepatitis occurred in February-March 2009 in the Sabarkantha district of Gujarat in India, with 456 cases and 89 deaths. The center of the outbreak was Modasa taluka. All the victims gave history of receiving injections about 2-3 months prior to the development of clinical signs and symptoms from one particular doctor. Gross and continued use of contaminated injection devices led to this explosive outbreak with such high mortality. The particular doctor was caught and found guilty of such practices.[7]
The present study reports the virological confirmation of the etiology in this outbreak along with a brief review of the literature regarding unsafe injection practices existing in our country.
Subjects and Methods
Random blood samples were collected from 25 patients admitted in the local hospital during the ongoing outbreak from February to March 2009. Samples were screened for all virological markers of hepatitis A-E. Samples were also collected from healthy HCWs of the local hospital during the same duration. Written informed consent was taken from all the patients and HCWs. Screening was done using an immunoassay analyzer (Cobas e411; Roche Diagnostics, Indianapolis, IN, USA) for hepatitis B surface antigen (HBsAg), IgM and total antibodies to hepatitis B core antigen (HBc), hepatitis B e antigen (HBeAg) and antibody to HBe, antibodies to HCV, HIV and IgM antibodies to hepatitis A virus (HAV), as per the manufacturer's protocol. Samples were also tested by enzyme-linked immunosorbent assay for IgM antibodies hepatitis E virus (HEV) and hepatitis D virus (HDV) (ImmunoLISA™ Orgenics, Yavne, Israel). All HBsAg were confirmed by neutralization assay (Cobas e411; Roche Diagnostics). Of 45 health care workers, 42 gave history of complete immunization with HBV vaccine. In them, anti-HBs titers were assayed to determine their immune status (anti-HBs assay, Cobas e411; Roche Diagnostics). On samples with sufficient residual volume (n = 16), HBV DNA quantification was done by real-time polymerase chain reaction (PCR) using COBAS TaqMan HBV test with high pure extraction (Roche Diagnostics). The linear range of the assay is 29-1.1 × 108 IU/mL and the lower limit of detection was 6 IU/mL. Direct PCR sequencing was done for surface and polymerase gene for genotyping the virus and detection of mutations in these regions as per the methodology published elsewhere.[8] HBsAg quantification was done by the chemiluminiscent immunoassay (CLIA) method (Abbott Laboratories, Chicago, IL, USA) as per the manufacturer's guidelines.
Statistical analysis
Quantitative variables were expressed as median with inter quartile range (IQR), and qualitative variables were expressed as numbers with percentage. Statistical analysis was done using SPSS for Windows (Chicago, IL, USA) version 17.0.
Results
As described in Table 1, characteristically, all the patients presented with fever, jaundice and headache. The male to female ratio was 17:8. Mean age of the patients was 33.4 years (SD 12.9 years). Anti-HBc IgM was reactive in 22/25 (88%) patients. HBeAg was positive in 11/25 (44%) patients. Patients who were HBeAg non-reactive were anti-HBe reactive (56%). There was no significant co-infection with any other hepatitis viruses like HCV (0/25), HIV (0/25), HAV (2/25), HEV (2/25) and HDV (0/25). Median HBV DNA level was 2.6 × 104 IU/mL (IQR 1.18 × 102 to 6.7 × 106 IU/mL). The median HBsAg level was 35,450 IU/mL (IQR 450-2,49,750 IU/mL) [Table 2]. All the isolates were of genotype D and no mutations were detected in polymerase and surface gene regions of the isolates. Anti-HBs antibody titer in HCWs showed protective antibody titer in 42/45 (80%) [Table 3]. Samples with values ≥ 10 m IU/mL were considered as protective to HBV infection.
Table 1.
Clinical characteristics of patients
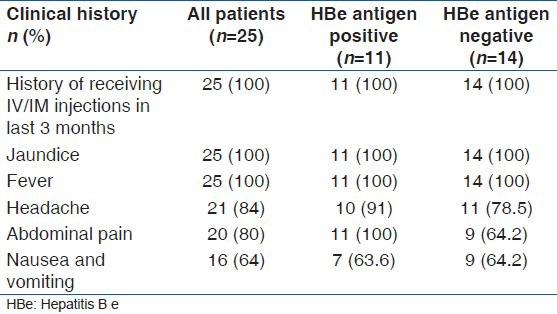
Table 2.
Molecular profile of acute hepatitis B patients (n=16)
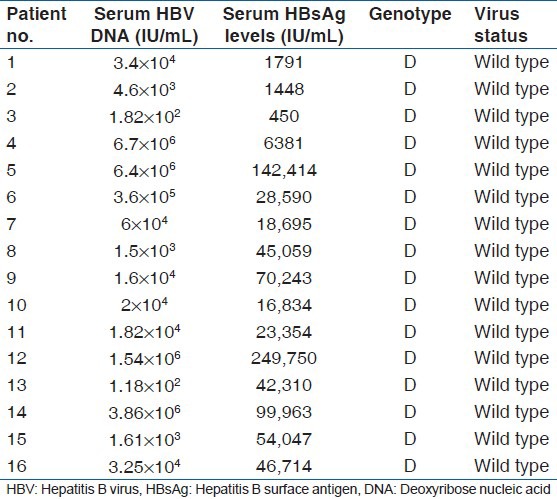
Table 3.
Sero-positivity of acute viral hepatitis markers

Discussion
The present study affirms HBV etiology in the outbreak of acute hepatitis in Modasa, Gujarat. There was no co-infection with other hepatitis viruses, especially HDV. All the isolates were of HBV genotype D. Most of the patients did not show very high viral load. As reported earlier, high mortality seen in this outbreak was not linked to high viral load in the patients but due to mutations in the pre-core and basal core promoter regions.[7] No mutations were detected in the surface and polymerase gene regions in all the isolates.
This outbreak of HBV was linked to unsafe injection practices prevalent in the region as all the victims gave history of receiving injections from one particular doctor prior to development of clinical signs and symptoms. Government authorities confirmed that the mode of transmission was from continuous use of contaminated needles and syringes as well as multiple use of single-use needle and syringes by private doctors in the Modasa town and adjoining areas by interviewing the patients, their family members and their doctors.[9] Unsafe injection practices are rampant, and investigations into this outbreak may be just an indicator of a major catastrophe waiting to occur. Reuse of single-use syringes and needles by the medical practioner also brought to light an illegal network for recycling medical waste existing in the region. There was an unusually high mortality in the present outbreak.[9] Initially, co-infection with other hepatotropic viruses was considered, but, as seen in our study, co-infection with other viruses was not found to be a co-factor. Four patients with co-infection with HAV and HEV seen in our study did not show any clinical severity of the disease. The only bright side to this sordid episode was that most of the HCWs at the district hospital had received hepatitis B vaccination and showed protective antibody titers. This highlights that at the HCW level, awareness regarding HBV immunization existed.
A similar outbreak had been reported from Mehsana in Gujarat a decade earlier. The mortality in this outbreak was also quite high (case-fatality rate of 47%). This outbreak had also been linked to unsafe injection use, and a local practioner had been implicated. In this outbreak, few cases had co-infection/super infection with HDV. Molecular studies were not reported, but it was assumed that a more virulent strain of virus might have led to the high mortality.[3] Another report highlighting the unsafe injection practices in India states that potential risk factors of hepatitis B transmission in our community is due to unnecessary therapeutic injections given by both qualified and unqualified doctors.[4] A recent survey on injection practices by health care personnel in Gujarat has shown that around 77% of medical care providers followed unsafe injection practices such as using a boiling pan for sterilization. Recapping of needles was done by 17%. Prevalence of needle stick injuries was 52.2%, which shows gross neglect of basic biosafety measures with regard to sharps.[6]
These two outbreaks, which were a decade apart, show that there has been no progress in raising awareness regarding safe injection practices at the grass-root level and that no lessons were learnt. The problem of unsafe injection practices continues to occur, and outbreaks like this might occur in the future if awareness in this matter is not created and appropriate actions are not taken.
An injection involves piercing of the skin to deliver a medication or vaccination to the body. This may be subcutaneous, intradermal, intramuscular, intravenous or intra-arterial. Injections are used for vaccination and therapeutic purposes. As per the WHO, 5% of injections are used for vaccination while 95% for therapeutic purposes.[1] Injections are associated with the risks of spreading blood borne pathogens, causing nerve and tissue injury, and may lead to the formation of abscesses. In the light of these risks, injections should be used only when safer therapeutic options such as oral, mucosal or rectal routes of delivery are not possible.[10] In practice, especially in developing nations, there is a lot of misuse and overuse of injections that are often given to earn additional revenue.
According to the WHO definition, a safe injection is one that does not harm the recipient, does not expose the provider to any avoidable risks and does not result in waste that is dangerous for the community.[11] Safe injection practices involve use of sterile single-use needles and syringes for each procedure, prevention of any form of contamination to the medication or vaccine to be injected, safe practices to ensure that sharps injuries do not occur and appropriate waste disposal to prevent reuse of needles and syringes.
Unsafe injection practices include a number of harmful practices considered unsafe for patients and/or health workers, such as use of injectable medication when safer alternatives are available, reuse of single-use disposable syringes and needles, multiple injections using a single needle and syringe, using a common container of IV fluid for more than one patient, recapping of needles, inadequately monitored needle and syringe cleaning and sterilization practices and improper disposal of sharps and syringes leading to recycling of these devices. All these practices put the patients, HCWs and the community at large at the risk of serious blood borne infections.
The reasons and prevalence of unsafe injection practices vary from country to country, and depend on a multitude of factors such as knowledge, awareness, sociocultural, economic and legal factors. Developed nations, where resource constraints are not a problem, are not immune from the hazards of unsafe injection practices. The risk of nosocomial infection with BBVs as a consequence of unsafe injection practices was recognized in high-income countries in the middle of the last century, and was brought into sharper focus by the advent of HIV/acquired immunodeficiency syndrome in the 1980s.[11] Reusable glass syringes and reusable needles were replaced by disposable plastic syringes and single-use needles during the 1950s and 1960s, and, for decades, the use of a new, disposable, sterile needle and syringe for each and every injection has been standard practice.[12] Infection control policies, guidelines and practices to enhance the safety of patients and health workers have been widely researched, implemented and evaluated. Consequently, the risk of nosocomial BBV infection due to unsafe injection practices in high-income countries has been brought under control.[13]
In developing countries, resource constraints and lack of routine surveillance system regarding safe injection practices have lead to several outbreaks of BBVs in these regions. As seen in our study, definitely, lack of knowledge, especially in private clinicians working in rural areas, is responsible for the spread of this kind of fatal infection in the community. The practice of recycling syringes is quite frequently done. A study in 2003-4 by the India CLEN Programme Evaluation Network (IPEN) revealed that in nearly one-fourth (23.5%) of all injections in India, the syringes and/or needles were reused.[14] Hence, there is an urgent need for organizational commitment to the occupational safety of healthcare workers, along with the provision of training in injection safety and universal precautions, adequate supplies of personal protective equipment and hepatitis B vaccination in order to prevent any more such drastic outbreaks. The sociodemographical factors are not associated with safe injection practices, but it is the sociocultural factors that play a greater role. There is a need to train service providers to choose the proper type of treatment (oral or injectable) and proper method of handling of injection equipment. Although the WHO has published an injection safety policy in 2003, there is an urgent need to develop local policies based on the suggested guidelines.[15]
Acknowledgments
The authors would like to thank Mr. Sandeep Tyagi and Mr. Gaurav Singh for excellent technical support.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe injections in the developing world and transmission of blood borne pathogens: A review. Bull World Health Organ. 1999;77:789–800. [PMC free article] [PubMed] [Google Scholar]
- 2.Miller MA, Pisani E. The cost of unsafe injections. Bull World Health Organ. 1999;77:808–11. [PMC free article] [PubMed] [Google Scholar]
- 3.Singh J, Bhatia R, Gandhi JC, Kaswekar AP, Khare S, Patel SB, et al. Outbreak of viral hepatitis B in a rural community in India linked to inadequately sterilized needles and syringes. Bull World Health Organ. 1998;76:93–8. [PMC free article] [PubMed] [Google Scholar]
- 4.Singh J, Gupta S, Khare S, Bhatia R, Jain DC, Sokhey J. A severe and explosive outbreak of hepatitis B in a rural population in Sirsa district, Haryana, India: Unnecessary therapeutic injections were a major risk factor. Epidemiol Infect. 2000;125:693–9. doi: 10.1017/s0950268800004684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Singh J, Bhatia R, Patnaik SK, Khare S, Bora D, Jain DC, et al. Community studies on hepatitis B in Rajahmundry town of Andhra Pradesh, India, 1997-8: Unnecessary therapeutic are a major risk factor. Epidemiol Infect. 2000;125:367–75. doi: 10.1017/s0950268899003854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pandit NB, Choudhary SK. Unsafe injection practices in Gujarat, India. Singapore Med J. 2008;49:936–9. [PubMed] [Google Scholar]
- 7.Arankalle VA, Gandhi S, Lole KS, Chadha MS, Gupte GM, Lokhande MU. An outbreak of hepatitis B with high mortality in India: Association with precore, basal core promoter mutants and improperly sterilized syringes. J Viral Hepat. 2011;18:20–8. doi: 10.1111/j.1365-2893.2010.01391.x. [DOI] [PubMed] [Google Scholar]
- 8.Vincenti D, Solmone M, Garbuglia AR, Iacomi F, Capobianchi MR. A sensitive direct sequencing assay based on nested PCR for the detection of HBV polymerase and surface glycoprotein mutations. J Virol Methods. 2009;159:53–7. doi: 10.1016/j.jviromet.2009.02.027. [DOI] [PubMed] [Google Scholar]
- 9.Patel DA, Gupta PA, Kinariwala DM, Shah HS, Trivedi GR, Vegad MM. An investigation of an outbreak of Viral Hepatitis B in Modasa Town, Gujarat, India. J Glob Infect Dis. 2012;4:55–9. doi: 10.4103/0974-777X.93762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fact Sheet No. 232. Geneva: WHO October; 1999. [Last accessed on 2012 Feb 10]. World Health Organization. Safety of Injections. Available from: http://www.who.int/mediacentre/factsheets/fs231/en/index.html . [Google Scholar]
- 11.Hutin YJ, Chen RT. Injection safety: A global challenge. Bull World Health Organ. 1999;77:787–8. [PMC free article] [PubMed] [Google Scholar]
- 12.Drucker E, Alcabes PG, Marx PA. The injection century; massive unsterile injections and the emergence of human pathogens. Lancet. 2001;358:1989–92. doi: 10.1016/S0140-6736(01)06967-7. [DOI] [PubMed] [Google Scholar]
- 13.The Safe Injection Global Network (SIGN) report 2010. [Last accessed on 2012 Feb 10]. Available from: http://www.who.int/injection_safety/toolbox/sign2010_meeting.pdf .
- 14.India CLEN Programme Evaluation Network. Assessment of injection practices in India (2002-2003) [Last accessed on 2012 Oct 9]. Available from: http://www.inclentrust.org/uploadedbyfck/file/complete%20Project/Executive%20summaru/15_Main%20Report%20 Book%20 (29-6-06)%20only.pdf .
- 15.World Health Organization. Managing an Injection Safety Policy. 2003. [Last accessed on 2012 Feb 10]. Available from: http://www.who.int/injection_safety/toolbox/en/ManagingInjectionSafety.pdf .