

Abstract
Background:
To identify the socio-demographic differences between a sample of women who present for first-trimester and second-trimester abortion.
Aim:
To determine whether women presenting late (in the second trimester) for abortion differ socio-demographically from those presenting early (in the first trimester).
Materials and Methods:
Data over 4 years for women presenting for second-trimester abortion were collected from the records of Family Planning Clinic at a public tertiary level teaching hospital in India. Eighty-four cases were analysed. The case presenting for first-trimester abortion after each second-trimester abortion was included for comparison. Information was gathered concerning age, parity, educational background, employment status, educational background of the husband, family expenditure and religion. Data were statistically analysed and significance determined using logistic regression analysis.
Results:
Second-trimester abortions represented 2% (84/4254) of all abortions in the study period. More women of higher age (P = 0.03) and parity (P = 0.02) and higher educational status (P = 0.04) presented for second-trimester abortion as compared to first-trimester abortion. The occupational status of the woman, husband's educational background, monthly family expenditure per person and religion did not significantly influence the time of presentation for abortion.
Conclusion:
Second-trimester abortions are associated with both increasing age and parity and higher education. This group of educated, older and multiparous women should be one of those targeted for counseling to reduce the risks associated with second trimester abortion.
Keywords: Abortion, First trimester, Second trimester, Socio-demographic characteristics
Introduction
Ever since the liberalization of the Medical Termination of Pregnancy Act 1971, the number of legal abortions in India has risen markedly. The latest national data show that they now exceed 640,000 annually.[1] In India, induced abortion is legal up to 20 weeks’ gestation; however, the decision for second-trimester abortion requires the concurrence of two registered medical practitioners.[2] While abortions before 12 weeks are safer, some women may present after this time. Those performed later in pregnancy are associated with greater morbidity and mortality, economic and emotional burden on the patients and staff.[3] Delaying abortion until the second trimester could be due to detection of anomalies or sex-selection, the latter of which is illegal in India but it frequently occurs.[4]
Globally, mid-trimester procedures constitute 10-15% of all abortions being done;[5] a study from Africa indicates that the proportion may be as high as 20%.[6] The few qualitative studies from around the world which have highlighted the causes for second-trimester abortion mention delay in recognizing the pregnancy, barriers to service access and time taken to make a decision.[6,7] However, there are no data to indicate whether the socio-demographics of the women concerned differ from those of women who present early, although one study has highlighted the differences between Blacks and Whites in terms of late abortion in the South of the USA.[8]
There are limited studies from India and South-east Asia which portray differences in socio-demographic characteristics between women who present early versus those who present in the second trimester. While an analysis of the reasons behind this phenomenon may help to improve policy making and guide public health interventions, a study of the differences in socio-demographics between these two groups can help identifying the target population for these interventions.
Materials and Methods
A retrospective data analysis was performed on all cases presenting to the Family Planning Clinic, Obstetrics and Gynaecology Department, Lok Nayak Hospital, New Delhi, for second trimester abortion from September 2003 to August 2007. The first case that presented for first-trimester abortion after each second-trimester abortion was included for comparison. In the context of the study, first-trimester abortion was defined as one performed at a gestational age of at most 12 completed weeks of gestation and second-trimester abortion as one carried out between 13 and 20 completed weeks of gestation. Mid-trimester abortions were carried out during that time by extra-amniotic ethacridine lactate instillation followed by intravenous infusion of escalating doses of oxytocin after 6 hours, while first-trimester procedures were done by suction evacuation.
The characteristics compared in the two groups were age, parity, educational background, employment status, educational background of the husband, monthly family expenditure per person and religion. Data were analysed using descriptive statistics in SPSS ver. 16.0 [SPSS Inc., Chicago, IL], and statistical significance determined by means of logistic regression analysis and Odds Ratios calculated with 95% confidence intervals. A P value < 0.05 was considered significant.
Results
The total number of abortions carried out at our hospital during the period under study amounted to 4254. Second-trimester abortions represented 2% (84/4254) of these. The socio-demographic characteristics are highlighted in Table 1.
Table 1.
Socio-demographic characteristics by gestational age at the time of induced abortion
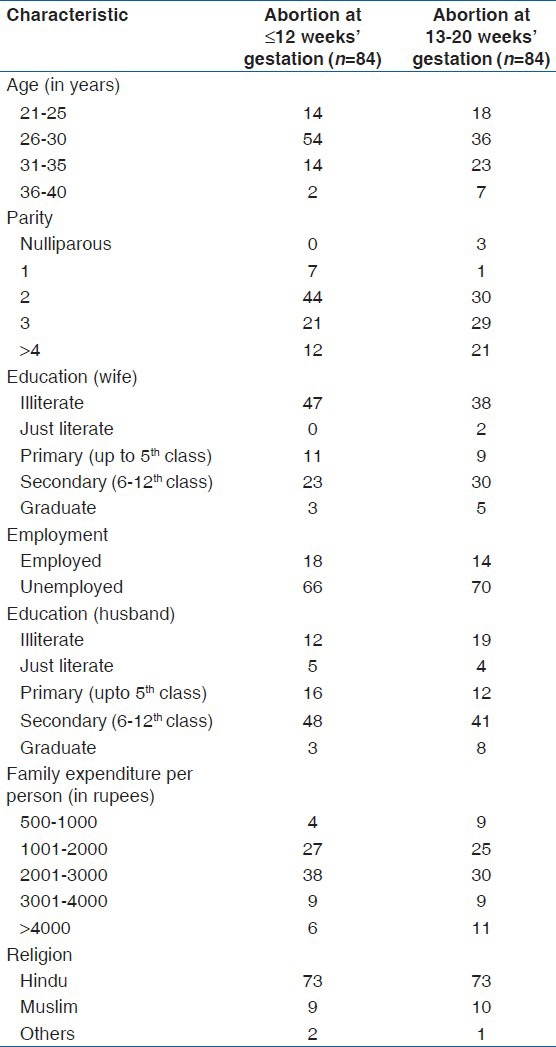
For meaningful statistical analysis, where possible, data which were not binomial were converted to binomial data by defining cut-off points. Women aged 30 years or less were clubbed and segregated from those older than 30 years, women with parity ≤2 were separated from those with parity >3, educational levels of wife and husband were divided into primary school or higher education (even if they did not study beyond secondary school), and monthly family expenditure per person into <1000 or >1000 rupees (1 rupee = 0.016 €).
Binary logistic regression was applied to explore significant predictors among the socio-demographic variables for time of seeking abortion. The outcome/dependant variable was considered as the presentation for abortion, i.e., presenting late for abortion as compared to an early presentation. Variables were dichotomized into two groups as independent measures [Table 2]. Enter method of logistic regression (LR) was applied, keeping all the possible variables as part of the equation as independent variables. Table 2 shows that significant predictors of late presentation for abortion, in our study were age, parity and educational status of the woman.
Table 2.
Predictors of late presentation for abortion
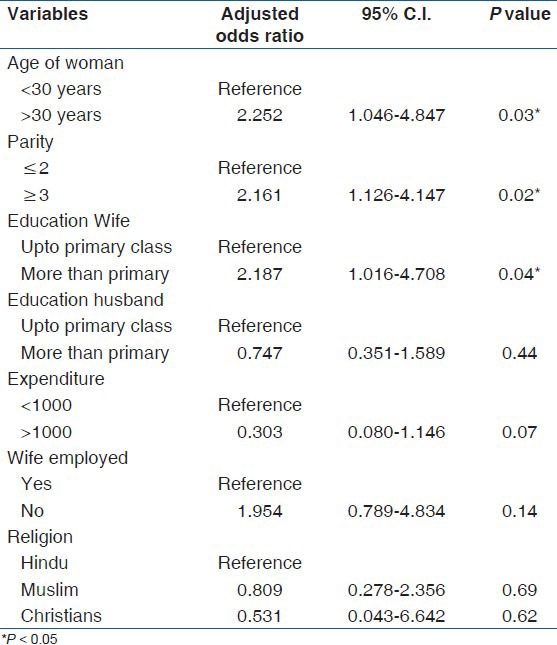
Women aged >30 years were 2.25 times (95% C.I. 1.04-4.84) more likely to seek a late abortion as compared to younger women. Multiparous women of parity three or more were 2.16 times (95% C.I. 1.12-4.14) more likely to present for late abortions as compared to those with parity 2 or less. Education of the woman was also seen as a significant predictor on applying LR, wherein it was observed that women with education grade higher than primary class were 2.18 times (95% C.I. 1.01-4.7) more likely to present for a later abortion as compared to women with education up to primary level.
Discussion
The percentage of second-trimester abortions at our centre was 2% which is lower than the global reported proportion. This is possibly due to many women not presenting to the government hospital. A low sex ratio (number of females per 1000 males) of 866 in the city (as per the 2011 census)[9] confirms this hypothesis, as some second-trimester abortions carried out with the purpose of sex-selection are illegal and hence unreported. According to one study, the mortality from abortions rises exponentially by 38% for each additional week of gestation beyond 8 weeks.[10] Some of the causes for second-trimester abortions have been highlighted earlier;[6,7,11,12] they include difficulty in early recognition of pregnancy and logistic delays, the latter being partly woman-related and partly service-related.[13] However, whether factors such as age, parity, education, employment, income and religion influence the timing for presentation for abortion is not well documented.
This study highlights two important findings, namely, the association of second trimester abortion with increasing age and parity, and with higher educational status of the woman. These findings may seem paradoxical, as one would presume that more educated and experienced women, both in terms of age and gestations would rather present early as unawareness of the pregnant state would not apply. Indeed some studies have reported a greater incidence of second-trimester abortions among nulliparous and young women for the aforementioned reasons.[14,15,16] That the findings of the present study should contrast from these may have two possible reasons. Firstly, advancing age and parity may lessen the concern of women for their healthcare. Secondly, there may be unidentified factors like family illness and commitments, conception during lactation, and denial of maintained fertility that preclude presentation at the appropriate time. Well-educated women presenting late for abortion may also be explained by two reasons. One, better educated women are more likely to be employed professionally and thus may not be able to spare time to seek abortion timely. Two, this subset of the population is more likely to have a single child due to professional commitments and may thus be resorting to sex-selective abortion. These factors are worth investigating in a well-designed prospective study. Our study, being retrospective, may suffer from omitted variable bias. Certain variables like prior contraceptive use, previous abortions, and cohabitation with partner, which may also influence the results, cannot be evaluated due to non-availability of recorded data. However, our findings can provide a starting point to identify target groups which are more likely to present for second trimester abortion (older, educated and multiparous women) and should be the focus of intended counselling.
Some investigators[17,18] have identified low education level as a determinant of second trimester abortion, but this did not apply in our study.
An Indian study[19] has compared the socio-demographics of unmarried nulliparous women between 15-24 years who presented for first and second trimester abortion and found that older and more educated women presented earlier for abortion, a finding that contrasts from our study. However, our study only included three nulliparous women and a different population base which could be the reason for divergent results.
Nevertheless, our study, albeit small and restricted to one public hospital, can serve as a starting point for larger prospective studies to support or refute these findings.
Knowledge of the characteristics of women who present late for abortion can help to design health policies and counselling programs with regard to certain groups that are more prone to delays in seeking abortion. This can help to reduce the number of second-trimester abortions and hence the complications resulting from these procedures.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Family Welfare Statistics in India 2009. Ministry of Health and Family Welfare. [Last accessed on 2011 Mar 18]. Available from: http://mohfw.nic.in/Complete%20BOOK/Complete%20BOOK.pdf .
- 2.The Medical Termination of Pregnancy Act, 1971. Ministry of Health and Family Welfare. [Last accessed on 2011 Mar 18]. Available from: http://www.mohfw.nic.in/MTP%20Act%201971.htm .
- 3.Burr WA, Schulz KF. Delayed abortion in an area of easy accessibility. JAMA. 1980;244:44–8. [PubMed] [Google Scholar]
- 4.Pre-conception and prenatal diagnostic techniques (Prohibition of sex selection) Act, 1994. Ministry of Health and Family Welfare. [Last accessed on 2011 Mar 18]. Available from: http://www.mohfw.nic.in/THE%20PNDT%20ACT%20(PRINCIPAL%20ACT) 1994.htm .
- 5.Lalitkumar S, Bygdeman M, Gemzell-Danielsson K. Mid-trimester induced abortion: A review. Hum Reprod Update. 2007;13:37–52. doi: 10.1093/humupd/dml049. [DOI] [PubMed] [Google Scholar]
- 6.Harries J, Orner P, Gabriel M, Mitchell E. Delays in seeking an abortion until the second trimester: A qualitative study in South Africa. Reprod Health. 2007;4:7. doi: 10.1186/1742-4755-4-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gallo MF, Nghia NC. Real life is different: A qualitative study of why women delay abortion until the second trimester in Vietnam. Soc Sci Med. 2007;64:1812–22. doi: 10.1016/j.socscimed.2007.02.005. [DOI] [PubMed] [Google Scholar]
- 8.Lynxwiler J, Wilson M. A case study of race differences among late abortion patients. Women Health. 1994;21:43–56. doi: 10.1300/J013v21n04_03. [DOI] [PubMed] [Google Scholar]
- 9.Census of India: Provisional Population Totals India: Paper I: Census 2011. [Last accessed on 2011 May 23]. Available from: http://www.censusindia.gov.in/2011-prov-results/data_files/india/Final%20PPT%202011_chapter 5.pdf .
- 10.Bartlett LA, Berg CJ, Shulman HB, Zane SB, Green CA, Whitehead S, et al. Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol. 2004;103:729–37. doi: 10.1097/01.AOG.0000116260.81570.60. [DOI] [PubMed] [Google Scholar]
- 11.Drey EA, Foster DG, Jackson RA, Lee SJ, Cardenas LH, Darney PD. Risk factors associated with presenting for abortion in the second trimester. Obstet Gynecol. 2006;107:128–35. doi: 10.1097/01.AOG.0000189095.32382.d0. [DOI] [PubMed] [Google Scholar]
- 12.Ingham R, Lee E, Clements SJ, Stone N. Reasons for second trimester abortions in England and Wales. Reprod Health Matters. 2008;16:18–29. doi: 10.1016/S0968-8080(08)31375-5. [DOI] [PubMed] [Google Scholar]
- 13.Lee E, Ingham R. Why do women present late for induced abortion? Best Pract Res Clin Obstet Gynaecol. 2010;24:479–89. doi: 10.1016/j.bpobgyn.2010.02.005. [DOI] [PubMed] [Google Scholar]
- 14.Mallory GB, Jr, Rubenstein LZ, Drosness DL, Kleiner GJ, Sidel VW. Factors responsible for delay in obtaining interruption of pregnancy. Obstet Gynecol. 1972;40:556–62. [PubMed] [Google Scholar]
- 15.Kiley JW, Yee LM, Niemi CM, Feinglass JM, Simon MA. Delays in request for pregnancy termination: Comparison of patients in the first and second trimesters. Contraception. 2010;81:446–51. doi: 10.1016/j.contraception.2009.12.021. [DOI] [PubMed] [Google Scholar]
- 16.Loeber O, Wijsen C. Factors influencing the percentage of second trimester abortions in the Netherlands. Reprod Health Matters. 2008;16:30–6. doi: 10.1016/S0968-8080(08)31377-9. [DOI] [PubMed] [Google Scholar]
- 17.Font-Ribera L, Pérez G, Espelt A, Salvador J, Borrell C. Determinants of induced abortion delay. Gac Sanit. 2009;23:415–9. doi: 10.1016/j.gaceta.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 18.Guilbert E, Marcoux S, Rioux JE. Factors associated with the obtaining of a second-trimester induced abortion. Can J Public Health. 1994;85:402–6. [PubMed] [Google Scholar]
- 19.Kalyanwala S, Zavier AJ, Jejeebhoy S, Kumar R. Abortion experiences of unmarried young women in India: Evidence from a facility-based study in Bihar and Jharkhand. Int Perspect Sex Reprod Health. 2010;36:62–71. doi: 10.1363/ipsrh.36.062.10. [DOI] [PubMed] [Google Scholar]