

Abstract
Orbital cellulitis describes an infection involving the soft tissues posterior to the orbital septum, including the fat and muscle within the bony orbit. This condition may be associated with severe sight and life-threatening complications. Despite significant advances in antimicrobial therapies and diagnostic technologies, the management of orbital cellulitis often remains challenging, and rapid diagnosis and prompt initiation of therapy are important in minimizing complications and optimizing outcomes. This review summarizes the distinctive characteristics of preseptal and orbital cellulitis, with a focus on anatomic considerations, predisposing conditions, approaches to evaluation, and management strategies.
Keywords: Orbital cellulitis, Evaluation, Management
1. Introduction
Orbital (postseptal) cellulitis is used to describe infectious involvement of the tissues posterior to the orbital septum, including the fat and muscle within the bony orbit. Preseptal cellulitis, in contrast, characterizes a cellulitis of the tissues localized anterior to the orbital septum. This distinction is important, as orbital cellulitis, while less common, may be associated with significant visual and life-threatening sequelae, including optic neuropathy, encephalomeningitis, cavernous sinus thrombosis, sepsis, and intracranial abscess formation (Lessner and Stern, 1992; Schmitt et al., 2005; Yeh et al., 2010). As such, rapid diagnosis and prompt initiation of therapy are important in order to minimize complications and optimize outcomes.
Medical management focuses primarily on aggressive antibiotic therapy while treating underlying predisposing factors such as sinusitis (Lessner and Stern, 1992; Mills and Kartush, 1985). Surgical intervention may be indicated in cases of orbital cellulitis with an associated foreign body, although in cases of orbital cellulitis with an associated abscess, the precise need and timing of surgery are less clearly defined (Harris, 1983; Howe and Jones, 2004). Some surgeons have advocated immediate surgical drainage, whereas other surgeons have reported that many of these abscesses resolve with medical therapy alone (Harris, 1983; Howe and Jones, 2004; Rahbar et al., 2001; Greenberg and Pollard, 1998, 2001; Rubin et al., 1989; Sajjadian et al., 1999).
Advancements in diagnostic technology and antibiotic therapy continue to evolve, and these improvements have reduced the associated morbidity and mortality of orbital cellulitis (Chaudhry and Shamsi, 2007; Ambati and Ambati, 2000). The management of orbital cellulitis, however, remains challenging, and prompt diagnosis and expeditious treatment are paramount in minimizing complications and optimizing outcomes. In this review, we will discuss the distinctive characteristics of preseptal and orbital cellulitis, with a focus on anatomic considerations, predisposing factors, approaches to evaluation, and management options.
2. Anatomy
There are several important anatomic considerations that are particularly relevant in the setting of orbital cellulitis. The distinction between preseptal and orbital cellulitis lies in the location and extent of the inflammatory process, and one of the major landmarks in this determination is the orbital septum. In preseptal cellulitis, the inflammatory process is localized anterior to the orbital septum, while in orbital cellulitis there is involvement of the soft tissues posterior to the orbital septum, including the orbital soft tissues. The orbital septum is part of the anterior orbital connective tissue framework and provides the mechanical function of containing orbital fat. Structurally, the orbital septum is a thin, fibrous, multilaminated structure that attaches peripherally to the periosteum of the orbital margin to form the arcus marginalis (Koornneef, 1979).
In the orbit, several surgical spaces exist and include the intraconal, extraconal, subperiosteal, and sub-Tenon’s spaces. The extraocular rectus muscles of the eye originate at the annulus of Zinn in the posterior orbit, and intermuscular septa connecting these muscles establish an anatomic cone that divides the orbital space into intraconal and extraconal compartments. In the posterior orbit, however, fascial connections between the rectus muscles are thin and may be incomplete, and as such, processes localized in the posterior orbit may extend between the intraconal and extraconal spaces.
The subperiosteal space is a potential space that is present between the periorbita and the bony orbital walls. The periorbita has firm attachments to the bone at the orbital suture lines. In other areas, however, the periorbita is relatively loosely adherent to the bony orbit. Hence, this potential subperiosteal space may provide an additional avenue for the spread of inflammatory or infectious processes.
From a vascular standpoint, several notable anatomic considerations exist. Venous drainage of the paranasal sinuses and the middle region of the face are mainly through the orbital veins, which communicate with the pterygoid plexus and cavernous sinus. In the orbit, these veins lack valves, which as a result, may allow passage of infectious processes in both anterograde and retrograde directions. Superficial infections of the face, therefore, may gain entry and pass posteriorly into the cavernous sinus and pterygoid plexus. A septic process of the cavernous sinus can result in involvement of the structures that are present within the sinus, including the oculomotor nerve, the trochlear nerve, the branches of the trigeminal nerve, the abducens nerve, the internal carotid artery, and the sympathetic nerves of the orbit. Lastly, an infectious process of the cavernous sinus may further extend to the contralateral cavernous sinus, the pituitary gland, and the surrounding meninges, leading to severe sight and life-threatening sequelae.
The paranasal sinuses are important structures in the pathophysiology of orbital cellulitis, as these structures are a common source of infection in both the pediatric and adult age groups (Harris, 1983; Chandler et al., 1970). In a retrospective case series of 315 pediatric patients admitted for management of preseptal and orbital cellulitis (18 orbital, 297 preseptal), sinusitis was associated in all 18 cases of orbital cellulitis and in 44 cases of preseptal cellulitis (Ambati and Ambati, 2000). Anatomically, the paranasal sinuses are major components of the orbit. The medial orbital wall that separates the orbit from the ethmoid sinus is very thin, particularly in childhood, and several perforations exist through which valveless blood vessels and nerves travel. This combination of thin bone, naturally occurring perforations, and loosely adherent periorbita allows for communication of infectious and inflammatory processes between the ethmoidal air cells and the medial orbit. For these reasons, the medial wall is a common location for the development of subperiosteal abscesses (Fig. 1). In addition, the orbital floor inferiorly is also comprised of relatively thin bone and is susceptible to the formation of a subperiosteal abscess from an adjacent maxillary sinusitis (Fig. 2) (Chandler et al., 1970).
Figure 1.

CT scan showing a medial orbital subperiosteal abscess on the left side associated with ethmoid and sphenoid sinusitis.
Figure 2.

CT scan showing an inferior/medial orbital subperiosteal abscess on the right side associated with ethmoid and maxillary sinusitis.
In the superior orbit, the orbital roof is relatively thick in comparison to the medial and inferior walls. Severe infections of the overlying frontal sinus, however, can develop and may lead to meningitis, epidural and subdural abscesses, and intracerebral abscesses. Laterally, no sinus is present adjacent to the bony orbital wall. Lastly, the sphenoid sinus is adjacent posteriorly in the area of the orbital apex and optic canal. As such, infections of the sphenoid sinus may result in direct and significant visual sequelae (Chandler et al., 1970).
3. Preseptal cellulitis
Preseptal cellulitis describes an infection of the eyelid and superficial periorbital soft tissues without the involvement of the globe and orbit. It occurs more commonly than orbital cellulitis and is generally associated with a more favorable prognosis (Chaudhry and Shamsi, 2007; Ambati and Ambati, 2000). Preseptal cellulitis, nevertheless, requires accurate diagnosis and expeditious treatment, as the infection can progress posteriorly into the orbit and lead to significant visual and CNS complications (Howe and Jones, 2004; Jones and Steinkuller, 1988). Visual dysfunction may also result in children with prolonged eyelid edema secondary to occlusion amblyopia, and as such, particular attention should be paid in young patients.
3.1. Predisposing factors
Both preseptal cellulitis and orbital cellulitis occur more commonly in the pediatric population. A common cause of preseptal cellulitis is extension of infection from the paranasal sinuses (Chandler et al., 1970; Jones and Steinkuller, 1988; Oxford and McClay, 2005). Contiguous spread of infection from the soft tissues of the face and ocular adnexa are also important sources of infection and may result from trauma, foreign bodies, insect bites, skin infections (impetigo), eyelid lesions (chalazia, hordeola), and iatrogenic causes such as eyelid and oral procedures (Cox et al., 1994; Molarte and Isenberg, 1989; Smith et al., 1978). In a retrospective review of 104 patients with preseptal cellulitis over a 15-year period, the most common predisposing etiologies were acute dacryocystitis (32.6%), sinusitis/upper respiratory infection (28.8%), and recent trauma/surgery (27.8%) (Chaudhry and Shamsi, 2007; Kikkawa et al., 2002).
3.2. Clinical manifestations
Preseptal cellulitis typically presents with eyelid edema and erythema, features characteristic of cellulitis. The extent of infection, however, is superficial and does not extend posteriorly into the orbit. As such, patients with preseptal cellulitis will present with normal vision, absence of proptosis, and full ocular motility without pain on movement.
3.3. Evaluation
Both preseptal and orbital cellulitis can present with eyelid inflammation, and distinguishing between the two conditions may be challenging. In the evaluation of a patient with preseptal cellulitis, however, it is critical to assess for the presence of orbital involvement, as orbital cellulitis has the potential for serious complications. A meticulous examination based on the recognition of distinctive signs, relevant history, and an understanding of predisposing risk factors is paramount in accurate diagnosis and expeditious treatment (Howe and Jones, 2004; Jones and Steinkuller, 1988).
The evaluation should include a comprehensive ophthalmic examination, including an assessment of visual acuity, pupillary response, tonometry, anterior segment biomicroscopy, and ophthalmoscopy. As preseptal cellulitis involves the soft tissues anterior to the orbital septum, distinctive features of these patients include normal vision without proptosis/resistance to retropulsion, limitation of ocular motility, orbital pain, afferent pupillary defect, optic nerve edema, and posterior segment venous engorgement.
A meticulous examination of the ocular adnexa and globe is important, particularly in the setting of trauma, as perforating injuries to the globe may be present despite minimal preseptal signs and apparently trivial puncture wounds of the eyelids. For patients with a history suggestive of a possible foreign body injury, imaging with fine cuts through the orbit should be performed to assess for retained intraorbital and intraocular foreign bodies. Slit lamp microscopy focusing on findings suggestive of a possible open globe injury, including 360° subconjunctival hemorrhage, prolapsed uveal tissue, peaking of the pupil, and vitreous hemorrhage, should be performed. Particular attention should be directed to the area of the globe directly under a full-thickness puncture wound of the eyelid. In the event that the eye cannot be adequately assessed in the emergency room or clinic, an examination under anesthesia is mandatory.
A physical examination, including an assessment of routine vital signs, should be performed. Blood cultures should be obtained in patients with concern for systemic toxicity, and a lumbar puncture may be necessary if meningeal signs are present. If possible, samples of conjunctival discharge, eyelid lesions, and lacrimal sac material should be sent to microbiology.
3.4. Medical management
The primary management strategy in the treatment of preseptal cellulitis focuses on appropriate antibiotic therapy, which should be promptly initiated and modified based on clinical response and interpretation of Gram’s stain, culture, and sensitivity results. While no randomized, controlled studies have investigated the optimal antibiotic regimen for preseptal cellulitis, treatment regimens are typically based on empiric coverage of the common causative organisms.
Given the predisposing factors of preseptal cellulitis, antibiotic selection is directed towards causative agents of upper respiratory infections and sinusitis, particularly Staphylococcus and Streptococcus species (Howe and Jones, 2004; Israele and Nelson, 1987; Donahue and Schwartz, 1998; Uzcategui et al., 1998). Following the introduction of the Haemophilus influenzae type b (Hib) vaccine, a decline in Hib related cases has been noted, and most cases are caused by Streptococcus pneumoniae, followed by Staphylococcus aureus and Streptococcus pyogenes (Israele and Nelson, 1987; Donahue and Schwartz, 1998; Uzcategui et al., 1998; Noel et al., 1981; Watters et al., 1976). In cases of focal trauma, coverage for S. aureus should be considered. Lastly, local trends in antimicrobial susceptibility must be carefully considered to properly guide antibiotic selection, as different institutions in discrete localities may have distinctive flora with varied resistance profiles. Consultation with the infectious disease service can be considered to aid in selection of appropriate antimicrobial therapy.
In cases of mild preseptal cellulitis in adults and children older than 1 year of age, treatment is typically rendered on an outpatient basis with empiric broad spectrum oral antibiotics, provided there is reliable access to close follow-up and no evidence of systemic toxicity. Patients who fail to respond or demonstrate clinical worsening should be promptly transitioned to intravenous antibiotics. Additionally, differential diagnoses should be explored, and the possibility of resistant organisms considered.
Patients who require hospital admission with intravenous antibiotics include children less than 1 year of age, individuals who lack immunization against H. influenzae and S. pneumoniae, immunosuppressed patients, and those with evidence of more severe infection/systemic toxicity. Treatment is continued until there is apparent clinical improvement, after which, continued recovery should be assessed on oral antibiotics. If clinical improvement is maintained, patients may be managed on an outpatient basis, with a continued course of antibiotics for a duration of 7–10 days. Patients should also be informed to maintain vigilance and return for evaluation if there is evidence of clinical worsening.
Treatment for concurrent sinusitis should be pursued if present and for chronic cases requiring further intervention, appropriate referral should be arranged.
3.5. Surgical management
Patients with preseptal cellulitis generally do not require surgical intervention except in cases of an associated foreign body or eyelid abscess. Surgical drainage and debridement of a lid abscess can be performed by a small incision through the skin over an area of fluctuance. Loculations within the cavity of the abscess must be broken, and packing of the wound should be considered to promote further drainage. While this may be performed with local infiltrative anesthesia in the emergency room or a procedure room, uncooperative patients and/or children may require sedation.
Microbiologic evaluation of associated material should be performed, with direct inoculation to blood agar, chocolate agar, anaerobic medium, and gram stain. Culture and sensitivity results should be used to guide appropriate antibiotic therapy.
4. Orbital cellulitis
Orbital cellulitis describes infections that involve the tissues posterior to the orbital septum, including the fat and muscle within the bony orbit. Orbital cellulitis affects all age groups but is more common in the pediatric population. In contrast to the more common preseptal cellulitis, orbital cellulitis may be associated with significant complications, and as such, prompt diagnosis and expeditious treatment are important (Lessner and Stern, 1992; Schmitt et al., 2005; Yeh et al., 2010).
4.1. Predisposing factors
There are several notable predisposing factors to the development of orbital cellulitis, including direct inoculation as a result of trauma or surgery, hematogenous spread in the setting of bacteremia, or extension of infection or inflammation from adjacent paranasal sinuses, ocular and adnexal structures (Fig. 3) (Harris, 1983; Chandler et al., 1970; Oxford and McClay, 2005; Kikkawa et al., 2002). The most frequent cause of orbital cellulitis is secondary extension of infection from the paranasal sinuses, particularly from the ethmoid sinus given the thin medial orbital wall (Chandler et al., 1970). An edematous sinus mucosa with resultant narrowing of the ostia and impaired sinus drainage promotes the proliferation of indigenous microflora of the sinuses and upper respiratory tract. Resultant suppuration and direct extension through the thin bones of the orbital walls, venous channels, and foramina may provide the optimal conditions for the development of orbital cellulitis. Reported rates of an associated sinusitis in the setting of orbital cellulitis are common, with reported rates ranging as high as 100% (Ambati and Ambati, 2000).
Figure 3.

MRI scan showing severe orbital cellulitis on the right side associated with endophthalmitis of the globe. Note the multiple loculations within the posterior segment of the right eye.
Other notable causes of orbital cellulitis include trauma with associated orbital fracture or foreign body, dacryocystitis (nasolacrimal duct obstruction), dental infections, endophthalmitis, and untreated preseptal cellulitis (Howe and Jones, 2004; Cox et al., 1994; Molarte and Isenberg, 1989; Smith et al., 1978; Kikkawa et al., 2002; Allen et al., 1985). Orbital cellulitis is an uncommon occurrence following ophthalmic surgery but has been reported after strabismus surgery, eyelid surgery, anterior segment surgery, and peribulbar injection (Allen et al., 1985; Weakley, 1991; Lopez et al., 1995; Hofbauer et al., 1994).
4.2. Microbiology
The causative agent in orbital cellulitis may be difficult to identify as a result of normal flora contaminants, prior antibiotic therapy, and mixed infections. Historically, H. influenzae type b was one of the most common organisms associated with preseptal and orbital cellulitis in children prior to the introduction and widespread adoption of the Hib vaccine in 1985 (Chaudhry and Shamsi, 2007; Ambati and Ambati, 2000; Noel et al., 1981; Watters et al., 1976). Prior to 1990, the annual incidence of H. influenzae associated infection was approximately 18,000 in the United States among children less than 5 years of age, with 900–1200 of such cases being fatal (Redmond and Pichichero, 1984). The use of these vaccines has resulted in a marked decline in the number of Hib associated infections, including orbital cellulitis (Chaudhry and Shamsi, 2007; Ambati and Ambati, 2000; Donahue and Schwartz, 1998). Some authors suggest that H. influenzae may have facilitated the pathogenicity of other organisms, as the introduction of the vaccination coincided with a decline not only in the number of preseptal and orbital cellulitis cases associated with H. influenzae but also in the overall case rate (Ambati and Ambati, 2000). However, in developing countries and in those locations where the vaccines are not widely available, H. influenzae remains a frequent causative organism.
In the United States, the most common bacterial organism identified in preseptal cellulitis in the pediatric population is S. pneumoniae, followed by S. aureus and S. pyogenes (Israele and Nelson, 1987; Donahue and Schwartz, 1998; Uzcategui et al., 1998). Abscess formations in post-traumatic cases are usually caused by S. aureus and S. pyogenes. In culture positive pediatric orbital cellulitis, S. aureus and Streptococci species are the most commonly identified organisms (McKinley et al., 2007). In a more recent study examining the organisms isolated from cultures of orbital abscesses and sinus aspirates, Staphylococcus was the most common species (22 positive cultures, 36% of which were methicillin resistant S. aureus), followed by Stretpococcus species (13 positive culture results) (McKinley et al., 2007). Non-spore forming anaerobic bacteria, including Peptococcus, Peptostreptococcus, and Bacteroides, are less common causes and are associated with infections following human or animal bites.
In the past prior to widespread Hib vaccination, blood cultures were often positive. However, recent studies have shown that blood cultures have variable rates of positive growth and are usually negative, particularly in older patients (McKinley et al., 2007; Schramm et al., 1982). Cultures from nasal swabs and ocular secretions can be performed, but organisms recovered from orbital abscesses and sinus aspirates may be most reliable.
In immunocompromised patients, fungal etiologies of orbital cellulitis must be considered. Mucormycosis and Aspergillosis species are the typical causative fungal organisms (Lawson and Blitzer, 1993; Dhiwakar et al., 2003a,b). Both may result in nasal and palatal necrosis, but Mucormycosis typically has a more rapid onset (1–7 days) versus Aspergillosis, which tends to progress at a much slower, chronic pace (months).
4.3. Clinical manifestations
While both preseptal cellulitis and orbital cellulitis can present with edema and erythema of the periorbital tissues, the latter possess the potential for severe vision and life-threatening complications (Lessner and Stern, 1992; Schmitt et al., 2005; Yeh et al., 2010). Patients may present with severe eyelid edema, decreased vision, pain with eye movement, proptosis, and ophthalmoplegia. There is typically a history of acute sinusitis or upper respiratory tract infection in the days preceding the development of eyelid edema. Symptoms may progress rapidly, and as such, prompt diagnosis and expeditious treatment are paramount.
4.4. Evaluation
A systemic evaluation should be performed when a diagnosis of orbital cellulitis is being considered. An evaluation of basic vital signs and a careful assessment of constitutional symptoms, including general malaise and loss of appetite, are important parameters that can guide treatment response and may precede physical and radiographic changes (Harris, 1983; Greenberg and Pollard, 2001; Jones and Steinkuller, 1988). Cultures may be beneficial in identifying the causative agent and allowing for targeted antibiotic therapy.
The evaluation should include a comprehensive ophthalmic examination. An assessment of visual function should be performed. While an accurate measurement of acuity may be difficult to assess in the setting of eyelid edema/discharge/chemosis, particularly in pediatric patients, such measurements can be critical in assessing treatment response. Testing for an afferent pupillary defect and color vision as well as ophthalmoscopy to assess for optic nerve edema and venous tortuosity can also be utilized for this purpose to guide clinical and surgical decision-making. The amount of proptosis and degree of extraocular motility restriction should be measured and documented. As discussed previously, a meticulous examination of the ocular adnexa and globe is important, particularly in the setting of trauma.
In the case of an immunosuppressed patient, the possibility of fungal disease, such as mucormycosis or aspergillosis, must be considered in the differential diagnosis (Dhiwakar et al., 2003a,b; McCarty et al., 2004). This is particularly pertinent in patients with poorly controlled diabetes that present with dysfunction of multiple cranial nerves (i.e., orbital apex syndrome), which should raise concern for mucormycosis. A careful evaluation for necrotic tissue should be performed, and a biopsy for histopathology should be obtained for suspicious lesions. Metabolic status, including blood sugar control, should be optimized.
4.5. Imaging
An important element in the evaluation of orbital cellulitis is radiographic imaging. Computed tomography (CT) scans provide imaging of the orbital contents and paranasal sinuses, allowing for confirmation of extension of disease into the orbit, identification of concurrent sinus disease, and detection of the presence of orbital and subperiosteal abscesses (Eustis et al., 1998; Harris, 1996; Towbin et al., 1986). Intravenous contrast can be useful in differentiating between an abscess and inflammatory phlegmatous involvement of orbital tissues. Common locations for the abscess formation are adjacent to opacified paranasal sinuses. Specifically, frequent locations for the development of subperiosteal abscesses include the medial orbital wall and the orbital floor, given the thin medial wall adjacent to the ethmoid sinus and the thin orbital floor above the maxillary sinus, respectively.
There is some controversy as to whether or not all patients with suspected orbital cellulitis require a CT scan, particularly for pediatric patients, where radiation exposure and potential cancer risk may be a source of reluctance for physicians (Shah and Platt, 2008; Mills and Tsai, 2006). Many clinicians believe that if the clinical signs suggest orbital involvement, immediate radiographic imaging should be performed to confirm involvement of the orbit, assess for the presence of an abscess or foreign body, determine the degree of orbital involvement, and evaluate for potential sources of infection. This is particularly true in cases where the examination is limited (young children, significant periorbital edema), there is concern for CNS involvement, gross proptosis and ophthalmoplegia are present, there is no improvement or concern for progression despite appropriate treatment, and surgical intervention is being considered.
Magnetic resonance imaging (MRI) of the orbits is another option that limits radiation exposure while providing superior resolution of orbital soft tissues compared to CT and ultrasound. MRI may provide further advantages in the evaluation of a nonmetallic foreign body and suspected intracranial involvement (Mills and Tsai, 2006; Green et al., 1990). The main disadvantage of MRI, however, is the increased scanning time compared to standard CT, which may necessitate sedation and pediatric anesthesia consultation. Additionally, MRI services may not be readily available at all hours, all of which may hinder the ability to quickly obtain images and render prompt, appropriate therapy.
4.6. Medical management
Given the potential for significant complications, intravenous antibiotics should be started promptly for all cases of orbital cellulitis (Harris, 1983; Jones and Steinkuller, 1988). Treatment regimens are based on empiric coverage of most common causative organisms, typically gram-positive organisms such as Staphylococcus and Streptococcus. Antibiotic selection may later be modified once culture and sensitivity results become available. Local trends in antimicrobial susceptibility are a critically important consideration, as different communities may have distinctive flora with varied resistance profiles. For example, at our institution, greater than 75% of community acquired Staphylococcus infections are methicillin resistant, and as such, empiric therapy with vancomycin is the preferred first line agent.
Additionally, in order to provide broader coverage of gram negative and anaerobic organisms, cefotaxime and metronidazole or clindamycin are typically concurrently administered. Other possible antibiotic choices include piperacillin–tazobactam, ticarcillin–clavulanate, and ceftriaxone. For penicillin-allergic patients, vancomycin in combination with a fluoroquinolone can be considered. Treatment should be modified based on culture/sensitivity results and local resistance profiles, and consultation with the infectious disease service may be valuable.
For those patients with concurrent sinusitis, aggressive nasal hygiene is an important element of treatment. A course of nasal decongestant and saline nasal irrigation can promote drainage of the sinuses and may have a favorable impact on subperiosteal abscesses (Benninger et al., 1997; Brown and Graham, 2004). Intranasal corticosteroids can also be considered and may be useful in facilitating sinus drainage and reducing mucosal edema (Mygind, 1996). Patients with chronic, recurrent sinusitis may benefit from evaluation by the otolaryngology service.
The use of intravenous corticosteroids in the setting of orbital cellulitis is somewhat controversial, with reluctance stemming from suppressing the immune system and possibly worsening the disease process. However, tempering of the inflammatory response may be beneficial when used in conjunction with appropriate antibiotics, particularly once clinical improvement is noted. Treatment with intravenous corticosteroids has been shown to decrease mucosal edema and levels of inflammatory cytokines in the sinus mucosa of patients with acute and chronic sinusitis (Rubin and Zito, 1994; Cable et al., 2000; Wallwork et al., 2002; Fu et al., 2007). Additionally, in the setting of a subperiosteal abscess, while the inciting element is infectious, tempering of the inflammatory component may facilitate draining and resolution of sinusitis. While the role of corticosteroids in the acute management of orbital cellulitis has not been investigated in a prospective randomized fashion, its use does not appear to adversely affect outcomes (Yen and Yen, 2005).
4.7. Surgical management
Once appropriate medical therapy has been initiated, careful monitoring of visual function and constitutional signs are important to assess treatment response (Jones and Steinkuller, 1988; Harris, 1996). Increased fluid load from intravenous antibiotics may exacerbate physical findings, including eyelid edema and proptosis, and as such, should be taken into consideration.
Surgical intervention should be considered in patients who fail to respond or deteriorate on medical therapy, display worsening visual function/pupillary changes, or develop an orbital abscess, particularly in those cases that involve the orbital apex or intracranial extension.
Subperiosteal abscesses are identified on radiographic imaging and may be the result of progression and extension of infection or inflammation into the subperiosteal space. The need for immediate surgical intervention in the setting of a subperiosteal abscess can vary, as medial therapy alone may be sufficient, particularly in younger patients (Howe and Jones, 2004; Rahbar et al., 2001; Greenberg and Pollard, 1998; Rubin et al., 1989; Sajjadian et al., 1999; Garcia and Harris, 2000; Harris, 1994). Those patients with medial or inferior subperiosteal abscesses are more likely to respond to medical therapy, while those individuals with a superior subperiosteal abscess are more likely to require surgical drainage (Greenberg and Pollard, 1998). With respect to age, a retrospective study of subperiosteal abscesses secondary to sinusitis showed that single aerobes were more likely to be found in patients less than 9 years of age, whereas polymicrobial infections consisting of mixed aerobic and anaerobic flora were more likely in older patients (Greenberg and Pollard, 1998; Harris, 1994; Brook and Frazier, 1996). Additionally, non-medial abscesses had a tendency to occur in older children (Greenberg and Pollard, 1998). These differences may explain why patients younger than 9 years of age are more likely to respond to medical therapy alone, whereas older patients are more likely to require surgery (Ryan et al., 2009). Nevertheless, if there is doubt regarding clinical response and antibiotic efficacy, surgical drainage of the abscess to obtain sampling for culture and sensitivity analysis should be considered.
Patients with an orbital abscess typically are identified on radiographic imaging. Associated findings include proptosis, ophthalmoplegia, globe displacement, and severe eyelid edema. The presence and location of an orbital abscess do not necessarily correlate with disease severity or prognosis (Yen and Yen, 2005). Unlike subperiosteal abscesses, however, orbital abscesses usually require surgical drainage, particularly in cases where there is a lack of improvement/progression of disease despite antibiotics, a retained foreign body, and concurrent cavernous sinus or intracranial involvement (Harris, 1983; Howe and Jones, 2004; Chaudhry and Shamsi, 2007; Garcia and Harris, 2000).
There are several other situations that may necessitate prompt surgical intervention. Cases of retained orbital foreign body with associated orbital cellulitis, including iatrogenic foreign bodies such as scleral buckles and glaucoma drainage devices, require prompt removal of the foreign body to facilitate resolution of the infection (Fig. 4a and b) (Green et al., 1990). This is particularly true for wood and other vegetative material. Other situations include fulminant infection of an ocular adnexal structure, such as endophthalmitis or dacryocystitis, where surgical debulking of the infectious source is required in addition to antibiotic therapy. Surgical drainage should also be considered in older patients with completely opacified sinuses to facilitate resolution of infection. Lastly, in cases of mucormycosis or aspergillosis, treatment often involves extensive surgical debridement in addition to aggressive antifungal therapy (Dhiwakar et al., 2003a,b; McCarty et al., 2004).
Figure 4.
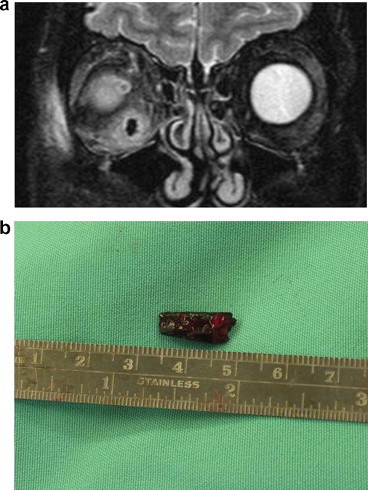
(a) MRI scan showing orbital cellulitis on the right side associated with an intraorbital foreign body. (b) Surgical exploration revealed a wood fragment from a tree branch as the foreign body.
5. Conclusions
Orbital cellulitis is not an uncommon condition with the potential for significant visual and life-threatening complications. Prompt diagnosis and expeditious treatment are important in minimizing complications, and an understanding of anatomic considerations, predisposing factors, microbiology, and evolving management strategies is paramount in achieving these goals.
Conflict of interest
The authors have no financial interest in any of the techniques or materials described.
References
- Allen M.V., Cohen K.L. Orbital cellulitis secondary to dacryocystitis following blepharoplasty. Ann. Ophthalmol. 1985;17(8):498–499. (August) [PubMed] [Google Scholar]
- Ambati B.K., Ambati J. Periorbital and orbital cellulitis before and after the advent of Haemophilus influenzae type B vaccination. Ophthalmology. 2000;107(8):1450–1453. doi: 10.1016/s0161-6420(00)00178-0. (August) [DOI] [PubMed] [Google Scholar]
- Benninger M.S., Anon J. The medical management of rhinosinusitis. Otolaryngol. Head Neck Surg. 1997;117:S41–S49. doi: 10.1016/S0194-59989770006-8. [DOI] [PubMed] [Google Scholar]
- Brook I., Frazier E.H. Microbiology of subperiosteal orbital abscess and associated maxillary sinusitis. Laryngoscope. 1996;106(8):1010–1013. doi: 10.1097/00005537-199608000-00019. (August) [DOI] [PubMed] [Google Scholar]
- Brown C.L., Graham S.M. Nasal irrigations: good or bad? Curr. Opin. Otolaryngol. Head Neck Surg. 2004;12:9–13. doi: 10.1097/00020840-200402000-00004. [DOI] [PubMed] [Google Scholar]
- Cable B.B., Wassmuth Z. The effect of corticosteroids in the treatment of experimental sinusitis. Am. J. Rhinol. 2000;14:217–222. doi: 10.2500/105065800779954400. [DOI] [PubMed] [Google Scholar]
- Chandler J.R., Langenbrunner D.J. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970;80:1414–1428. doi: 10.1288/00005537-197009000-00007. [DOI] [PubMed] [Google Scholar]
- Chaudhry I.A., Shamsi F.A. Outcome of treated orbital cellulitis in a tertiary eye care center in the middle East. Ophthalmology. 2007;114(2):345–354. doi: 10.1016/j.ophtha.2006.07.059. (February) [DOI] [PubMed] [Google Scholar]
- Cox N.H., Knowles M.A. Pre-septal cellulitis and facial erysipelas due to Moraxella species. Clin. Exp. Dermatol. 1994;19:321–323. doi: 10.1111/j.1365-2230.1994.tb01204.x. [DOI] [PubMed] [Google Scholar]
- Dhiwakar M., Thakar A. Improving outcomes in rhinocerebral mucormycosis – early diagnostic pointers and prognostic factors. J. Laryngol. Otol. 2003;117:861–865. doi: 10.1258/002221503322542854. [DOI] [PubMed] [Google Scholar]
- Dhiwakar M., Thakar A., Bahadur S. Invasive sino-orbital aspergillosis: surgical decisions and dilemmas. J. Laryngol. Otol. 2003;117:280–285. doi: 10.1258/00222150360600887. [DOI] [PubMed] [Google Scholar]
- Donahue S.P., Schwartz G. Preseptal and orbital cellulitis in childhood. A changing microbiologic spectrum. Ophthalmology. 1998;105:1902–1905. doi: 10.1016/S0161-6420(98)91038-7. [DOI] [PubMed] [Google Scholar]
- Eustis H.S., Mafee M.F. MR imaging and CT of orbital infections and complications in acute rhinosinusitis. Radiol. Clin. North Am. 1998;36(6):1165–1183. doi: 10.1016/s0033-8389(05)70238-4. (xi, November) [DOI] [PubMed] [Google Scholar]
- Fu S.Y., Su G.W. Cytokine expression in pediatric subperiosteal orbital abscesses. Can. J. Ophthalmol. 2007;42(6):865–869. doi: 10.3129/i07-151. (December) [DOI] [PubMed] [Google Scholar]
- Garcia G.H., Harris G.J. Criteria for nonsurgical management of subperiosteal abscess of the orbit: analysis of outcomes 1988–1998. Ophthalmology. 2000;107:1454–1456. doi: 10.1016/s0161-6420(00)00242-6. [DOI] [PubMed] [Google Scholar]
- Green B.F., Kraft S.P. Intraorbital wood. Detection by magnetic resonance imaging. Ophthalmology. 1990;97:608–611. doi: 10.1016/s0161-6420(90)32549-6. [DOI] [PubMed] [Google Scholar]
- Greenberg M.F., Pollard Z.F. Medical treatment of pediatric subperiosteal orbital abscess secondary to sinusitis. J. AAPOS. 1998;2:351–355. doi: 10.1016/s1091-8531(98)90033-7. [DOI] [PubMed] [Google Scholar]
- Greenberg M.F., Pollard Z.F. Nonsurgical management of subperiosteal abscess of the orbit. Ophthalmology. 2001;108:1167–1168. doi: 10.1016/s0161-6420(00)00627-8. [DOI] [PubMed] [Google Scholar]
- Harris G.J. Subperiosteal abscess of the orbit. Arch. Ophthalmol. 1983;101:751–757. doi: 10.1001/archopht.1983.01040010751010. [DOI] [PubMed] [Google Scholar]
- Harris G.J. Subperiosteal abscess of the orbit. Age as a factor in the bacteriology and response to treatment. Ophthalmology. 1994;101(3):585–595. doi: 10.1016/s0161-6420(94)31297-8. (March) [DOI] [PubMed] [Google Scholar]
- Harris G.J. Subperiosteal abscess of the orbit: computed tomography and the clinical course. Ophthal. Plast. Reconstr. Surg. 1996;12:1–8. doi: 10.1097/00002341-199603000-00001. [DOI] [PubMed] [Google Scholar]
- Hofbauer J.D., Gordon L.K. Acute orbital cellulitis after peribulbar injection. Am. J. Ophthalmol. 1994;118:391. doi: 10.1016/s0002-9394(14)72965-4. [DOI] [PubMed] [Google Scholar]
- Howe L., Jones N.S. Guidelines for the management of periorbital cellulitis/abscess. Clin. Otolaryngol. 2004;29:725–728. doi: 10.1111/j.1365-2273.2004.00889.x. [DOI] [PubMed] [Google Scholar]
- Israele V., Nelson J.D. Periorbital and orbital cellulitis. Pediatr. Infect. Dis. J. 1987;6:404–410. doi: 10.1097/00006454-198704000-00012. [DOI] [PubMed] [Google Scholar]
- Jones D.B., Steinkuller P.G. Strategies for the initial management of acute preseptal and orbital cellulitis. Trans. Am. Ophthalmol. Soc. 1988;86:94–108. [PMC free article] [PubMed] [Google Scholar]
- Kikkawa D.O., Heinz G.W. Orbital cellulitis and abscess secondary to dacryocystitis. Arch. Ophthalmol. 2002;120(8):1096–1099. (August) [PubMed] [Google Scholar]
- Koornneef L. Orbital septa: anatomy and function. Ophthalmology. 1979;86:876–880. doi: 10.1016/s0161-6420(79)35444-6. [DOI] [PubMed] [Google Scholar]
- Lawson W., Blitzer A. Fungal infections of the nose and paranasal sinuses. Part I. Otolaryngol. Clin. North Am. 1993;26:1007–1035. [PubMed] [Google Scholar]
- Lessner A., Stern G.A. Preseptal and orbital cellulitis. Infect. Dis. Clin. North Am. 1992;6:933–952. [PubMed] [Google Scholar]
- Lopez P.F., Marx J. Endophthalmitis and orbital cellulitis after radial keratotomy. Ophthalmology. 1995;102(12):1902–1907. doi: 10.1016/s0161-6420(95)30777-4. (McLeod SD; Flowers CW, December) [DOI] [PubMed] [Google Scholar]
- McCarty M.L., Wilson M.W. Manifestations of fungal cellulitis of the orbit in children with neutropenia and fever. Ophthal. Plast. Reconstr. Surg. 2004;20:217–223. doi: 10.1097/01.iop.0000124677.03668.d7. [DOI] [PubMed] [Google Scholar]
- McKinley S.H., Yen M.T. Microbiology of pediatric orbital cellulitis. Am. J. Ophthalmol. 2007;144(4):497–501. doi: 10.1016/j.ajo.2007.04.049. (Epub 2007 August 15, October) [DOI] [PubMed] [Google Scholar]
- Mills R.P., Kartush J.M. Orbital wall thickness and the spread of infection from the paranasal sinuses. Clin. Otolaryngol. 1985;10(4):209–216. doi: 10.1111/j.1365-2273.1985.tb00243.x. (August) [DOI] [PubMed] [Google Scholar]
- Mills D.M., Tsai S. Pediatric ophthalmic computed tomographic scanning and associated cancer risk. Am. J. Ophthalmol. 2006;142(6):1046–1053. doi: 10.1016/j.ajo.2006.08.024. (Epub 2006 October 11, December) [DOI] [PubMed] [Google Scholar]
- Molarte A.B., Isenberg S.J. Periorbital cellulitis in infancy. J. Pediatr. Ophthalmol. Strab. 1989;26:232–234. doi: 10.3928/0191-3913-19890901-06. [DOI] [PubMed] [Google Scholar]
- Mygind N. Effects of corticosteroid therapy in non-allergic rhinosinusitis. Acta Otolaryngol. 1996;116:164–166. doi: 10.3109/00016489609137814. [DOI] [PubMed] [Google Scholar]
- Noel L.P., Clarke W.N. Periorbital and orbital cellulitis in childhood. Can. J. Ophthalmol. 1981;16:178–180. [PubMed] [Google Scholar]
- Oxford L.E., McClay J. Complications of acute sinusitis in children. Otolaryngol. Head Neck Surg. 2005;133:32–37. doi: 10.1016/j.otohns.2005.03.020. [DOI] [PubMed] [Google Scholar]
- Rahbar R., Robson C.D. Management of orbital subperiosteal abscess in children. Arch. Otolaryngol. Head Neck Surg. 2001;127:281–286. doi: 10.1001/archotol.127.3.281. [DOI] [PubMed] [Google Scholar]
- Redmond S.R., Pichichero M.E. Haemophilus influenzae type b disease. An epidemiologic study with special reference to day-care centers. JAMA. 1984;252:2581–2584. doi: 10.1001/jama.252.18.2581. [DOI] [PubMed] [Google Scholar]
- Rubin S.E., Zito J. Orbital subperiosteal abscess responding to medical therapy. J. Pediatr. Ophthalmol. Strab. 1994;31:325–326. doi: 10.3928/0191-3913-19940901-12. [DOI] [PubMed] [Google Scholar]
- Rubin S.E., Rubin L.G. Medical management of orbital subperiosteal abscess in children. J. Pediatr. Ophthalmol. Strab. 1989;26:21–27. doi: 10.3928/0191-3913-19890101-06. [DOI] [PubMed] [Google Scholar]
- Ryan J.T., Preciado D.A. Management of pediatric orbital cellulitis in patients with radiographic findings of subperiosteal abscess. Otolaryngol. Head Neck Surg. 2009;140(6):907–911. doi: 10.1016/j.otohns.2009.02.014. (Epub 2009 April 16, June) [DOI] [PubMed] [Google Scholar]
- Sajjadian A., Chundru U. Prospective application of a protocol for selective nonsurgical management of suspected orbital subperiosteal abscesses in children. Ann. Otol. Rhinol. Laryngol. 1999;108:459–462. doi: 10.1177/000348949910800507. [DOI] [PubMed] [Google Scholar]
- Schmitt N.J., Beatty R.L. Superior ophthalmic vein thrombosis in a patient with dacryocystitis-induced orbital cellulitis. Ophthal. Plast. Reconstr. Surg. 2005;21:387–389. doi: 10.1097/01.iop.0000176269.84949.96. [DOI] [PubMed] [Google Scholar]
- Schramm V.L., Jr., Curtin H.D. Evaluation of orbital cellulitis and results of treatment. Laryngoscope. 1982;92(7 Pt 1):732–738. doi: 10.1288/00005537-198207000-00004. (July) [DOI] [PubMed] [Google Scholar]
- Shah N.B., Platt S.L. ALARA: is there a cause for alarm? Reducing radiation risks from computed tomography scanning in children. Curr. Opin. Pediatr. 2008;20(3):243–247. doi: 10.1097/MOP.0b013e3282ffafd2. (June) [DOI] [PubMed] [Google Scholar]
- Smith T.F., O’Day D. Clinical implications of preseptal (periorbital) cellulitis in childhood. Pediatrics. 1978;62(6):1006–1009. (December) [PubMed] [Google Scholar]
- Towbin R., Han B.K. Postseptal cellulitis: CT in the diagnosis and management. Radiology. 1986;158:735–737. doi: 10.1148/radiology.158.3.3945747. [DOI] [PubMed] [Google Scholar]
- Uzcategui N., Warman R. Clinical practice guidelines for the management of orbital cellulitis. J. Pediatr. Ophthalmol. Strab. 1998;35(2):73–79. doi: 10.3928/0191-3913-19980301-04. (March–April) [DOI] [PubMed] [Google Scholar]
- Wallwork B., Coman W. Clarithromycin and prednisolone inhibit cytokine production in chronic rhinosinusitis. Laryngoscope. 2002;112:1827–1830. doi: 10.1097/00005537-200210000-00022. [DOI] [PubMed] [Google Scholar]
- Watters E.C., Wallar P.H. Acute orbital cellulitis. Arch. Ophthalmol. 1976;94:785–788. doi: 10.1001/archopht.1976.03910030387007. [DOI] [PubMed] [Google Scholar]
- Weakley D.R. Orbital cellulitis complicating strabismus surgery: a case report and review of the literature. Ann. Ophthalmol. 1991;23(12):454–457. (December) [PubMed] [Google Scholar]
- Yeh C.H., Chen W.C. Intracranial brain abscess preceded by orbital cellulitis and sinusitis. J. Craniofac. Surg. 2010;21(3):934–936. doi: 10.1097/SCS.0b013e3181d84124. (May) [DOI] [PubMed] [Google Scholar]
- Yen M.T., Yen K.G. Effect of corticosteroids in the acute management of pediatric orbital cellulitis with subperiosteal abscess. Ophthal. Plast. Reconstr. Surg. 2005;21(5):363–366. doi: 10.1097/01.iop.0000179973.44003.f7. (discussion 366–367, September) [DOI] [PubMed] [Google Scholar]