

Myeloid malignancies (MMs) are a heterogeneous group of hematologic malignancies presenting different incidence, prognosis and survival.1–3 Changing classifications (FAB 1994, WHO 2001 and WHO 2008) and few available epidemiological data complicate incidence comparisons.4,5 Taking this into account, the aims of the present study were: a) to calculate the incidence rates and trends of MMs in the Province of Girona, northeastern Spain, between 1994 and 2008 according to the WHO 2001 classification; and b) to predict the number of MMs cases in Spain during 2013. Data were extracted from the population-based Girona Cancer Registry (GCR) located in the north-east of Catalonia, Spain, and covering a population of 731,864 inhabitants (2008 census). Cases were registered according to the rules of the European Network for Cancer Registries and the Manual for Coding and Reporting Haematological Malignancies (HAEMACARE project). To ensure the complete coverage of MMs in the GCR, and especially myeloproliferative neoplasms (MPN) and myelodysplastic syndromes (MDS), a retrospective search was performed. The ICD-O-2 (1990) codes were converted into their corresponding ICD-O-3 (2000) codes, including MDS, polycythemia vera (PV) and essential thrombocythemia (ET) as malignant diseases. Results of crude rate (CR) and European standardized incidence rate (ASRE) were expressed per 100,000 inhabitants/year.
A total of 1,331 cases of MMs were diagnosed in the province of Girona from 1994 to 2008: 718 men (53.9%) and 613 women (46.1%). Acute myeloid leukemia (AML) accounted for 24.0% (319 of 1,331), MDS 34.4% (458 of 1,331), MPN 36.7% (489 of 1,331) including chronic myeloid leukemia (CML), and myelodysplastic/myeloproliferative neoplasms (MDS/MPN) for 4.9% (65 of 1,331).
The MMs CR was 15.04 and ASRE was 11.08 (13.06 in men and 9.56 in women), with a statistically significant male predominance (sex ratio 1.17). Median age was 72 years in men and 73 years in women (Table 1).
Table 1.
Number of cases, median age, incidence rates and sex ratio of myeloid malignancies diagnosed in Girona province (1994–2008) according to the 2001 WHO classification.
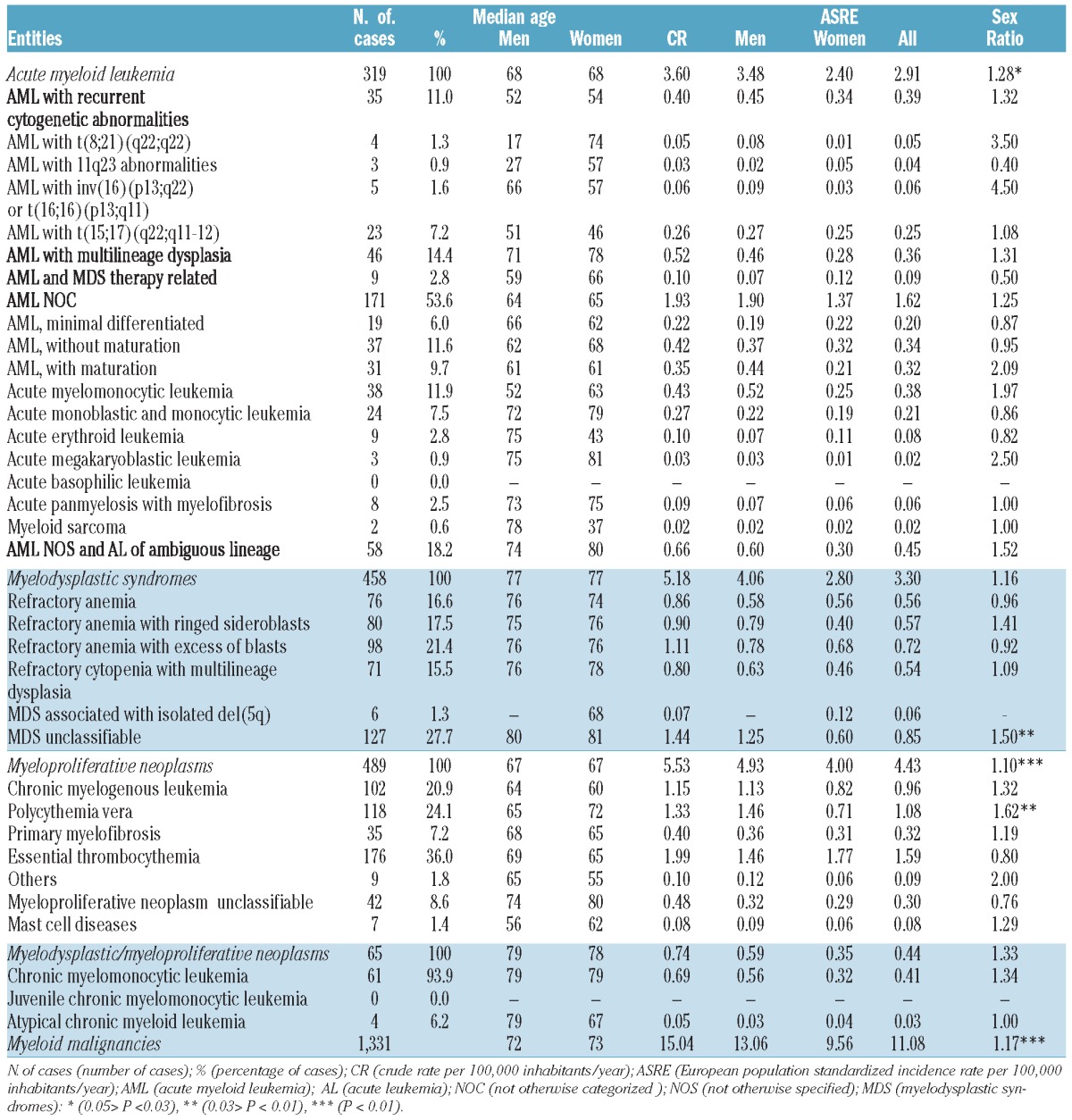
Although the highest incidence among MMs groups in the province of Girona was MPN (ASRE = 4.43), diagnosis was often made in outpatient settings and this means these cancers are more likely to be underreported to cancer registries than other cancers. However, our results were similar to those reported in south-east England, although we included mast cell diseases as recommended by the WHO 2008.5,6 The median age of patients at diagnosis was 67 years and a significant male predominance was found both overall and also in the PV entity (Table 1).
Since ICD-O-3 (International Classification of Diseases for Oncology) was introduced, MDS can now be reported in cancer registries. Due to changes in MMs classification, and the advanced age of patients at diagnosis, these diseases have not been as well documented as other pathologies. The most frequent type within this group was MDS unclassifiable, and the least was 5q- syndrome (Table 1). The incidence of MDS (ASRE = 3.30) was close to that reported in south-east England and Germany.6,7 The higher incidence of MDS in the province of Girona than in the French study could be due to the fact that the Côte d’Or Department is a hematologic monographic registry. They used positive criteria such as karyotype abnormalities or evolution to a more aggressive type to register cases of refractory anemia in order to avoid the inclusion of false cases.8 The lower incidence of MDS in the US may be due to the underreporting of cases.9,10
The overall ASRE for AML was 2.91, with a statistically male predominance (sex ratio 1.28). The median age of AML patients was 68 years, being lower in AML with recurrent cytogenetic abnormalities and therapy-related AML. Approximately 54% (171 of 319) of cases were AML not otherwise categorized, and within this group, the majority of cases were acute myelomonocytic leukemia and AML without maturation. The AML and MDS therapy-related group was the less frequent within the four main AML groups (Table 1). The incidence rate of AML in the province of Girona was similar to that reported in France, south-east England and Sardinia.6,8,11 Nevertheless, the proportion of AML with cytogenetic abnormalities in our cohort was lower than in France and the UK.8,12 This is probably because karyotype tests were made outside the province of Girona and information was not always available for older cases. The most frequent cytogenetic abnormality was the t(15;17), as in France and the UK.8,12
Finally, the myeloid group with the lowest incidence was MDS/MPN, with an ASRE of 0.44 (Table 1). The median age at diagnosis was 78 years. Chronic myelomonocytic leukemia (CMML) was the most frequent entity, comprising more than 90% of all MDS/MPN cases. Our results were comparable to others reported in south-east England or Germany.6,7 Differences were found between our incidence rates and those reported in France, probably because in the province of Girona some cases of CMML were recoded as MDS.8 The lower incidence in the US could be a consequence of underreported cases.9,10
Significant increases in incidence trends were found in the MDS, MPN and MDS/MPN groups (Figure 1), although these could be considered unreliable. The presence of some gene mutations and the improvements in diagnostic techniques could be the reasons for these changes in incidence trends. The discovery of the JAK2 V617F mutation in 2005 could have resulted in an increase in some MPN, such PV, ET, and primary myelofibrosis, which have been identified objectively as pathological since the introduction of molecular biology.13,14 No increase in incidence of AML was found between 1994–2008, similar to results reported from France, the UK and the US.8,12,15
Figure 1.

Trends in standardized incidence rate of myeloid malignancy WHO categories in Girona province (1994–2008). This figure shows the modeled standardized incidence rate. Values under the figure represented the real standardized incidence rate by year and myeloid groups.
According to our predictions, 7,551 new cases of MMs will be diagnosed in Spain for the year 2013, of which 1,772 cases will be AML, 2,647 MDS, 2,744 MPN and 388 MDS/MPN. These results are of interest for clinicians and those involved in public health in order to evaluate the cost of new treatments for these pathologies. Some limitations of this study must be considered. Classification of MMs has changed in recent decades and there could be an underreporting of cases. Also, an increased outpatient diagnosis over time makes it difficult to ensure complete coverage of MMs in cancer registries, especially MDS and MPN.
This study describes in detail the incidence of MMs in a large population-based cohort. MPN were the group with the highest incidence of MMs in the province of Girona and incidence trends increased significantly in MDS, MPN and MDS/MPN. Our results show that recent advances in diagnosis of MMs and an increase in outpatient diagnosis have resulted in changes in incidence rate trends.
Footnotes
Funding: This study was supported with the pre-doctoral grant “Formació Personal Investigador” (FI) from the Autonomous Government of Catalonia.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Rodriguez-Abreu D, Bordoni A, Zucca E. Epidemiology of hematological malignancies. Ann Oncol. 2007;18 Suppl 1:i3–i8 [DOI] [PubMed] [Google Scholar]
- 2.Sant M, Allemani C, Tereanu C, de Angelis R, Capocaccia R, Visser O, et al. Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood. 2010;116(19):3724–34 [DOI] [PubMed] [Google Scholar]
- 3.Visser O, Trama A, Maynadie M, Stiller C, Marcos-Gragera R, de Angelis R, et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur J Cancer. 2012;48(17):3257–66 [DOI] [PubMed] [Google Scholar]
- 4.Vardiman JW, Harris NL, Brunning RD. The World Health Organization (WHO) classification of the myeloid neoplasms. Blood. 2002;100(7):2292–302 [DOI] [PubMed] [Google Scholar]
- 5.Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114(5):937–51 [DOI] [PubMed] [Google Scholar]
- 6.Phekoo KJ, Richards MA, Moller H, Schey SA. The incidence and outcome of myeloid malignancies in 2,112 adult patients in southeast England. Haematologica. 2006;91(10):1400–4 [PubMed] [Google Scholar]
- 7.Neukirchen J, Schoonen WM, Strupp C, Gattermann N, Aul C, Haas R, et al. Incidence and prevalence of myelodysplastic syndromes: data from the Dusseldorf MDS-registry. Leuk Res. 2011;35(12):1591–6 [DOI] [PubMed] [Google Scholar]
- 8.Maynadie M, Girodon F, Manivet-Janoray I, Mounier M, Mugneret F, Bailly F, et al. Twenty-five years of epidemiological recording on myeloid malignancies: data from the specialized registry of hematologic malignancies of Cote d’Or (Burgundy, France). Haematologica. 2011;96(1):55–61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer. 2007;109(8):1536–42 [DOI] [PubMed] [Google Scholar]
- 10.Rollison DE, Howlader N, Smith MT, Strom SS, Merritt WD, Ries LA, et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001–2004, using data from the NAACCR and SEER programs. Blood. 2008;112(1):45–52 [DOI] [PubMed] [Google Scholar]
- 11.Broccia G, Deplano W, Dessalvi P, Giannico B, Luxi G, Chessa E, et al. Hematological malignancies in the island of Sardinia, 1974–1993: age and sex distributions and temporal changes in incidence. Hematol Oncol. 2004;22(3):91–109 [DOI] [PubMed] [Google Scholar]
- 12.Sanderson RN, Johnson PR, Moorman AV, Roman E, Willett E, Taylor PR, et al. Population-based demographic study of karyotypes in 1709 patients with adult acute myeloid leukemia. Leukemia. 2006;20(3):444–50 [DOI] [PubMed] [Google Scholar]
- 13.Girodon F, Bonicelli G, Schaeffer C, Mounier M, Carillo S, Lafon I, et al. Significant increase in the apparent incidence of essential thrombocythemia related to new WHO diagnostic criteria: a population-based study. Haematologica. 2009;94(6):865–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schafer AI. Molecular basis of the diagnosis and treatment of polycythemia vera and essential thrombocythemia. Blood. 2006; 107(11):4214–22 [DOI] [PubMed] [Google Scholar]
- 15.Xie Y, Davies SM, Xiang Y, Robison LL, Ross JA. Trends in leukemia incidence and survival in the United States (1973–1998). Cancer. 2003;97(9):2229–35 [DOI] [PubMed] [Google Scholar]