

Abstract
Advanced cancer is a risk factor for venous thromboembolism. However, lymph node metastases are usually not considered an established risk factor. In the framework of the prospective, observational Vienna Cancer and Thrombosis Study we investigated the association between local (N0), regional (N1–3), and distant (M1) cancer stages and the occurrence of venous thromboembolism. Furthermore, we were specifically interested in the relationship between stage and biomarkers that have been reported to be associated with venous thromboembolism. We followed 832 patients with solid tumors for a median of 527 days. The study end-point was symptomatic venous thromboembolism. At study inclusion, 241 patients had local, 138 regional, and 453 distant stage cancer. The cumulative probability of venous thromboembolism after 6 months in patients with local, regional and distant stage cancer was 2.1%, 6.5% and 6.0%, respectively (P=0.002). Compared to patients with local stage disease, patients with regional and distant stage disease had a significantly higher risk of venous thromboembolism in multivariable Cox-regression analysis including age, newly diagnosed cancer (versus progression of disease), surgery, radiotherapy, and chemotherapy (regional: HR=3.7, 95% CI: 1.5–9.6; distant: HR=5.4, 95% CI: 2.3–12.9). Furthermore, patients with regional or distant stage disease had significantly higher levels of D-dimer, factor VIII, and platelets, and lower hemoglobin levels than those with local stage disease. These results demonstrate an increased risk of venous thromboembolism in patients with regional disease. Elevated levels of predictive biomarkers in patients with regional disease underpin the results and are in line with the activation of the hemostatic system in the early phase of metastatic dissemination.
Introduction
Cancer patients have a higher risk of developing venous thromboembolism (VTE) than patients without cancer, and VTE has a negative impact on the survival of cancer patients.1–6 However, the risk of VTE among cancer patients differs considerably3,5 and is below 10% even in certain groups of patients with advanced cancer.7 Predictive parameters are, therefore, required to stratify patients into risk groups. In the last years, clinical research on prediction of cancer-associated VTE has focused on clinical and laboratory parameters.8–14 Based on laboratory and clinical parameters associated with VTE, a scoring model for the prediction of VTE in cancer patients was recently developed15 and has already been expanded16 and validated17 in other study populations. However, given the heterogeneity of cancer patients, improved predictability and better understanding of the underlying pathomechanisms of cancer-associated VTE are desirable. Routine parameters that are usually available at initial diagnosis of every cancer patient would be particularly useful to help the oncologist to assess the VTE risk of each individual patient better.
Patients with advanced cancer have an elevated risk of developing VTE. Distant metastases in cancer patients are among the strongest risk factors for cancer-associated VTE.3,18,19 However, lymph node metastases are not usually regarded as an established risk factor.5,20,21 Studies of patients in the Californian Cancer Registry investigated the association between VTE and local, regional, and distant disease in a group of different cancer sites19 and in several single tumor entities.22–27 The risk was highest in patients with metastatic disease, but was also slightly elevated in patients with regional disease, compared to those with localized cancer only. As these studies were based on registry data obtained between 1990 and 1999, other influences on the risk of VTE, such as treatment-related factors, could not be considered. Moreover, to our knowledge there are no studies that have comprehensively investigated the relationship between laboratory biomarkers predictive of cancer-associated VTE and tumor stage, so as to elucidate the pathophysiology of the association between coagulation and malignancy.
We hypothesized that the presence of lymph node metastases is a strong risk factor for VTE and is associated with increased levels of biomarkers predictive of cancer-associated VTE. To test this hypothesis, we prospectively followed 832 cancer patients and investigated the relationship between local (N0), regional (N1–3), and distant (M1) cancer stages and the occurrence of VTE. Furthermore, we correlated all plasma biomarkers that have been established to be predictive of cancer-associated VTE, namely D-dimer,8 prothrombin fragment 1 and 2 (F1 + F2),8 clotting factor VIII,13 platelets,15 soluble P-selectin (sP-selectin),9 leukocytes15 and hemoglobin concentration15 with local, regional, and distant cancer stages, to elucidate the pathogenesis of the prothrombotic state in patients with regional stage disease, and to establish possible links between the hemostatic system and the process of metastatic dissemination.
Design and Methods
The Vienna Cancer and Thrombosis Study (CATS) is an ongoing, prospective and observational cohort study at the Medical University of Vienna and is conducted in accordance with the Declaration of Helsinki after approval by the institutional ethics committee. The aim of CATS is to investigate factors that are associated with the occurrence of symptomatic VTE in patients with cancer. All patients with solid tumors included in the CATS between October 2003 and December 2009 were eligible for this study.
Study participants underwent tumor staging or, in the case of disease progression after remission, re-staging prior to study inclusion. The study participants were followed prospectively until the end of follow-up (2 years), occurrence of VTE, death, loss from follow-up, or withdrawal of consent. At study inclusion, venous blood samples were drawn and the patients’ medical history was recorded.
Based on the Tumor Node Metastasis (TNM) Classification specified by the Union for International Cancer Control (UICC)28 we defined three tumor stages: local, regional, and distant. Patients with no lymph node metastases and no distant metastases were classified as have local stage (TxN0M0) disease. Regional stage was defined by a positive lymph node status but concurrent absence of distant metastases (TxN1-3M0). The presence of distant metastases led to the classification of distant stage cancer, irrespective of the lymph node status (TxNxM1). Lymph node metastases and distant metastases were detected and verified by imaging techniques (e.g. computerized tomography), cancer biopsy, or cancer surgery.
The patients’ characteristics are described by medians and interquartile ranges for continuous variables because of the non-normal distributions, and by frequencies and percentages for categorical variables. The Kruskal-Wallis test was applied to compare the distribution of (non-normally distributed) biomarkers. In the case of a significant overall test result, a Mann-Whitney test was applied and corrected with Bonferroni’s correction. The median of the follow-up distribution was estimated by the Kaplan-Meier method with reverse meaning of the status indicator.29 Univariate and multivariable Cox-regression analyses were used to calculate the VTE risk for patients with local, regional and distant cancer. The first multivariable Cox-regression model (model 1) comprised regional stage (versus local stage), distant stage (versus local stage), surgery, radiotherapy, chemotherapy, age, and newly diagnosed cancer (versus progression of disease). We assumed that surgery, chemotherapy and radiotherapy would entail a modified risk for VTE not only limited to the exact time-point of the procedure, but also for a certain period afterwards. Therefore, three time-dependent binary variables that indicated times of possible influence on the VTE risk by surgery, chemotherapy, or radiotherapy were included in model 1. In a second multivariable Cox-regression analysis (model 2) we adjusted for laboratory biomarkers according to the availability in clinical practice (D-dimer, leukocytes, platelets, and hemoglobin), and newly diagnosed cancer. For reasons of comparability with other studies and to maximize practicality in clinical routine, laboratory biomarkers were dichotomized according to cut-off levels used in the Khorana VTE prediction score15 and, in the case of D-dimer, according to the 75th percentile of the CATS study population.8 More detailed information is available in the Online Supplementary Material.
Results
Study population
All patients with solid tumors included in the CATS between October 2003 and December 2009 (n=968) were eligible for this study. A total of 136 of these patients had to be excluded: 90 patients did not match the exact inclusion criteria after re-evaluation, for 39 patients no follow-up was available, and 7 patients were excluded because of incomplete information on tumor stage. Hence, 832 patients with solid tumors were enrolled (Table 1).
Table 1.
Baseline characteristics of the total study population and patients with VTE.
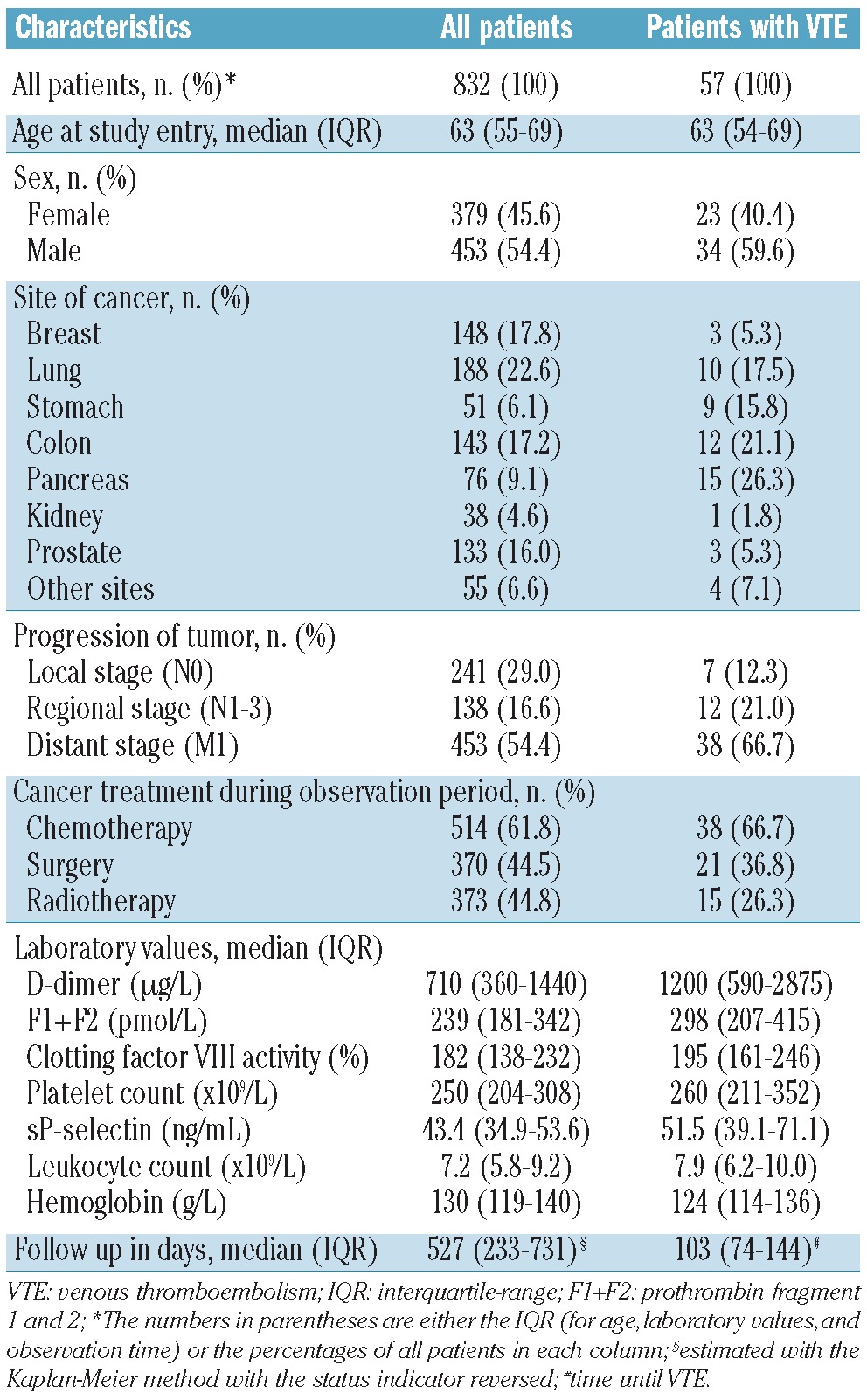
Four-hundred and ninety-four (59.4%) patients had newly diagnosed cancer and 338 (40.6%) patients had progression of disease after complete or partial remission. At study inclusion, the patients were classified as having local stage cancer (n=241; 29.0%), regional stage cancer (n=138; 16.6%), or distant stage cancer (n=453; 54.4%). Within those with regional cancer, 91 (66%) patients were classified as lymph node positive with N1 status, 38 (28%) as lymph node positive with N2 status, and 9 (7%) as lymph node positive with N3 status. Patients were observed for a median of 527 days. During the follow-up 333 (40.0%) patients died without clear evidence of fatal VTE.
Thromboembolic events
In 57 (6.9%) patients a clinically relevant VTE was detected. A deep vein thrombosis (DVT) of the lower extremity was diagnosed in 22, pulmonary embolism (PE) in 20, and combined DVT and PE in three patients. An isolated DVT of the upper extremity was detected in two patients. Each of the following events was diagnosed in one patient: combined DVT of the lower extremity and portal vein thrombosis, combined DVT of the upper extremity and PE, internal jugular vein thrombosis, and sinus vein thrombosis. PE was fatal in two patients. A portal vein thrombosis was diagnosed in four patients. All four portal vein thromboses occurred in patients with pancreatic cancer: one in a patient with local disease, one in a patient with regional cancer and two in patients with metastatic cancer. Of the 57 VTE events, several events were detected incidentally: seven cases of PE, two portal vein thromboses, one internal jugular vein thrombosis, and one DVT of the lower extremity. Nevertheless, they were rated as clinically relevant by the adjudication committee. The overall cumulative incidence of VTE was 4.9% after 6 months, 6.0% after 12 months, and 6.9 % after 2 years.
Risk of venous thromboembolism: tumor stage
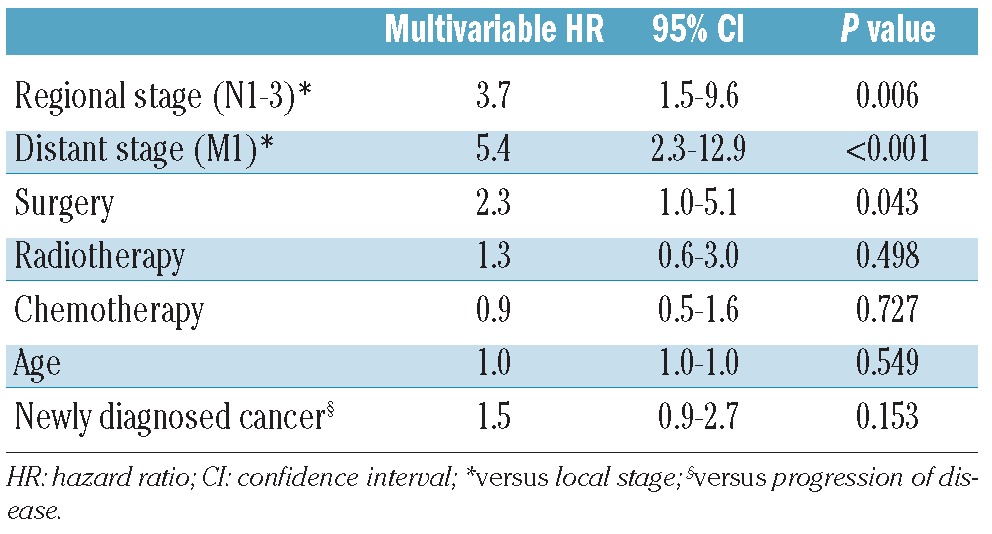
Seven (2.9%) patients with local disease, 12 (8.7%) with regional cancer, and 38 (8.4%) with distant cancer developed symptomatic VTE during the follow-up. In Kaplan-Meier analysis, the cumulative probability of VTE after 6 months was 2.1% in patients with local disease, 6.5% in patients with regional disease, and 6.0% in patients with distant cancer (Figure 1). Patients with regional and distant disease had a significantly higher risk of developing VTE compared to those with local cancer (log-rank test: P=0.002). No significant risk difference was found between patients with regional and distant stages of disease (log-rank test: P=0.707). In univariable Cox-regression analysis the risk of VTE was 3.5-fold (95% CI: 1.4–8.9, P=0.008) increased for regional stage compared to local stage, and 4.0-fold (95% CI: 1.8–9.0, P<0.001) increased for distant stage compared to local stage disease. In multivariable Cox-regression analysis (model 1) including surgery, radiotherapy, chemotherapy, age at study inclusion, and newly diagnosed cancer (versus progression of disease) the adjusted hazard ratio was 3.7 (95% CI: 1.5–9.6, P=0.006) in patients with regional stage disease compared to patients with local stage disease, and 5.4 (95% CI: 2.3–12.9, P<0.001) in those with distant cancer compared to patients with local stage disease (Table 2).
Figure 1.

Cumulative probability of VTE in patients with local, regional, and distant stage disease (log-rank test: P=0.002).
Table 2.
Multivariable Cox proportional hazards model (model 1) for association of regional metastases, distant metastases, surgery, radiotherapy, chemotherapy, age, and newly diagnosed cancer with VTE.
We also performed a separate evaluation of the frequency of VTE in the three different regional lymph node stages N1, N2, and N3. Of 91 patients with N1 status, eight (8.8%) developed VTE during the follow-up period while of the 38 patients with N2 status, four (10.5%) did so. None of the nine patients with N3 status had a VTE during the follow-up period.
Association of tumor stage with biomarkers
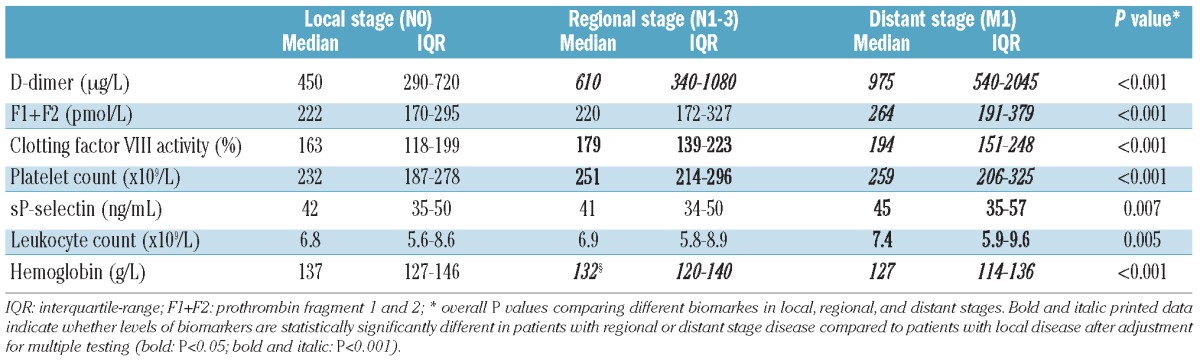
Patients with local, regional, or distant cancer had significantly different levels of all the biomarkers analyzed (D-dimer, F1+F2, factor VIII, platelets, sP-selectin, leukocytes, and hemoglobin; all P<0.0068). D-dimer levels, factor VIII activity, and platelet counts continuously increased from local to regional to distant stage, whereas hemoglobin levels continuously decreased. No continuous increase from local to regional to distant stage was found for leukocyte counts, F1+2, or sP-selectin levels.
Compared to patients with local disease, patients with regional stage disease had significantly higher D-dimer levels (P<0.001), platelet counts (P=0.002), and factor VIII activity (P=0.021), and lower levels of hemoglobin (P<0.001). Levels of F1+2, and leukocyte counts were not significantly elevated in patients with regional stage disease. Compared to patients with local disease, patients with distant disease had significantly increased levels of all biomarkers except hemoglobin concentration, which was significantly decreased (Table 3).
Table 3.
Distribution of biomarkers in patients with local, regional, and distant stage disease.
Risk of venous thromboembolism: tumor stage and routinely available biomarkers
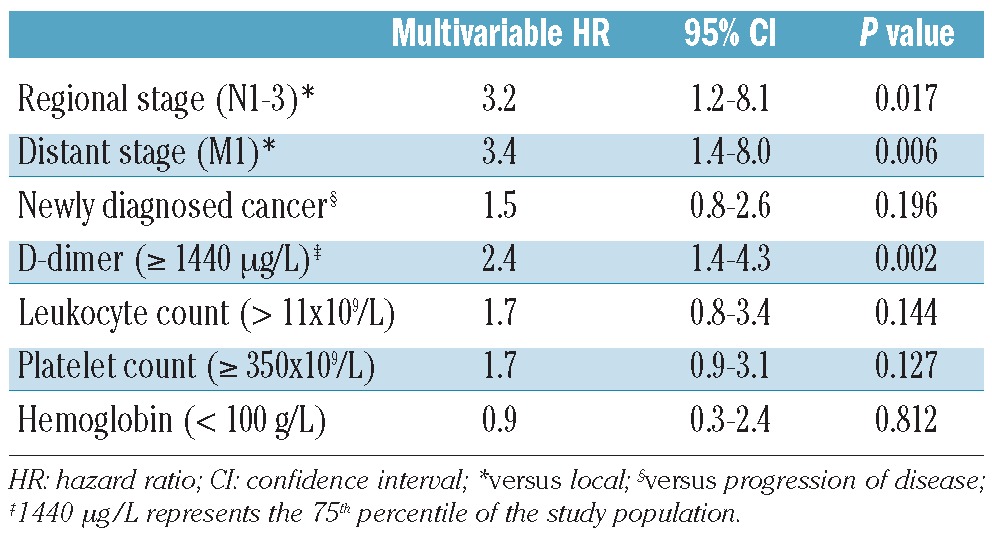
In order to consider selected laboratory biomarkers in the multivariable analysis, a second Cox-regression analysis (model 2) was performed. Model 2 comprised D-dimer, leukocytes, platelets, hemoglobin, tumor stage and newly diagnosed cancer. In this model, the hazard ratio of VTE was 3.2 (95% CI: 1.2–8.1, P=0.017) in patients with regional disease compared to patients with local disease, and 3.4 (95% CI: 1.4–8.0, P=0.006) in patients with distant disease compared to patients with local disease. D-dimer was the only biomarker in model 2 that was significantly associated with the occurrence of VTE (HR: 2.4, 95% CI: 1.4–4.3, P=0.002) (Table 4).
Table 4.
Multivariable Cox proportional hazards model (model 2) for association of regional metastases, distant metastases, newly diagnosed cancer, D-dimer, leukocytes, platelets, and hemoglobin.
Discussion
In this prospective study we demonstrate that regional lymph node metastases are a strong risk factor for cancer-associated VTE. Furthermore, a significant relationship between biomarkers predictive of cancer-related VTE and regional tumor stage is shown.
In our study, we were especially interested in the association between lymph node metastases and the occurrence of VTE. We, therefore, applied the TNM classification to elucidate the relationship between local (N0), regional (N1–3), and distant stage (M1) disease, and the occurrence of VTE. Previous studies paid only little attention to the clinical relevance of regional lymph node metastases as a risk factor for VTE in cancer patients. To our knowledge the only studies on this subject are those by the Californian Cancer Registry, which investigated the association between local, regional, and distant stage disease and the occurrence of VTE.19,22–27 Studies by the Californian Cancer Registry that focused on tumor sites similar to those included in CATS (lung, colon, stomach, pancreatic, breast, and prostate) reported an approximately 2-fold higher risk of VTE in patients with regional disease than in those with local cancer (odds ratios ranging from 1.1 in patients with pancreatic cancer to 2.7 in patients with colon cancer).19,22–24 Interestingly, in our study the risk of VTE in patients with regional stage cancer was clearly higher. We found that patients with regional stage cancer had a 3–4-fold higher risk of developing VTE than those with local stage cancer. In Kaplan-Meier analysis the cumulative risk of VTE after 6 months was even slightly higher in patients with regional lymph node metastases than in patients with distant metastases.
An explanation for the considerably higher risk of VTE in regional stage cancer patients in CATS might be that the Californian Cancer Registry studies are based on registry data, whereas CATS is a prospective study specifically designed to identify predictive parameters for cancer-associated VTE. We verified patients’ exact TNM status at study inclusion and documented type and duration of patients’ anti-cancer therapies during follow-up. To eliminate the confounding influence of anti-cancer therapies on the occurrence of VTE, we adjusted for surgery, chemotherapy, and radiotherapy in time-dependent Cox-regression analyses, and found that the hazard ratio of regional lymph node metastases for VTE remained similarly high.
It has been shown that the VTE risk in cancer patients is highest in the first 6 months after diagnosis.3 The inclusion of patients with progression of disease after remission in our study might, therefore, be a possible confounder, biasing the VTE risk in patients with regional and distant stage disease. Hence, we adjusted for newly diagnosed cancer (versus progression of disease) in the multivariable analyses. However, patients with newly diagnosed cancer did not have a significantly higher risk of VTE than patients with progression of disease after complete or partial remission.
The high incidence of VTE in patients with regional disease in our study was not caused by bulky lymph nodes obstructing the venous flow. However, in one patient with regional pancreatic cancer a local obstruction of venous flow by the primary tumor or regional lymph node metastases could not be definitely excluded, since VTE occurred in the portal vein.
In order to consider selected laboratory biomarkers in the multivariable analysis, we constructed a second Cox-regression model. The model included predictive biomarkers for cancer-associated VTE that are easy to determine and are routinely available in almost all hospital laboratories. Also in this extended model lymph node metastases were independently and strongly associated with the occurrence of VTE. The hazard ratio of VTE for lymph node metastases in model 2 was similar high to that for distant metastases in model 2, once again emphasizing the relevance of lymph node metastases as a strong risk factor for cancer-associated VTE.
To explain and understand the considerably elevated VTE risk in patients with regional stage disease it is helpful to take a closer look at the process of metastatic dissemination. The invasion of tumor cells into the blood stream or lymph fluid is essential for the development of distant metastases. Hence, contacts and interactions between tumor cells and the hemostatic system precede the manifestation of distant metastases. Thus, a hypercoagulable state in cancer patients may already exist in patients with regional spread. To support this approach to explaining the prothrombotic state in patients with regional stage disease, and to establish possible links between the hemostatic system and the process of metastatic dissemination, we correlated biomarkers that are predictive of cancer-associated VTE with local, regional, and distant disease.
In our investigations, D-dimer levels were already elevated in patients with regional cancer. This clearly confirms the assumption of a hypercoagulable state in patients with regional disease. These results are in line with the data of other studies that found a correlation between tumor stage and D-dimer levels in patients with breast cancer30 and colorectal cancer.31 Interestingly, F1+2 levels were elevated only in patients with distant cancer, but not in those with regional disease. The fact that in patients with regional disease D-dimer levels were increased, while F1+2 levels were not, indicates that tumors might induce a hypercoagulable state in patients with regional disease by interaction with the fibrinolytic system. This hypothesis is supported by the fact that malignant cells can activate coagulation in cancer patients by dysregulating fibrinolytic pathways.32 Clotting factor VIII activity and platelet counts were elevated in patients with regional and distant disease. We hypothesize that these factors might play an important role in the early phase of metastatic dissemination. In contrast, sP-selectin concentration and leukocyte counts were elevated only in patients with distant stage disease, suggesting that sP-selectin and inflammatory processes might play a more important role in the late phase of metastatic dissemination. In accordance with our findings, Connolly et al. demonstrated an association between pre-chemotherapy leukocytosis and distant metastases in a prospective observational study in patients with different types of malignancies.33 Low hemoglobin concentration is a predictive parameter for cancer-associated VTE and it is even part of the Khorana VTE prediction score.15 For this reason we also investigated the association between hemoglobin concentration and tumor stage. Hemoglobin levels were decreased in patients with regional and distant stage cancer.
Our study has several limitations. The tumor stage was collected only at study inclusion. We did not re-evaluate the stage at the time of occurrence of VTE. However, most of the VTE events (72%) in our study occurred in the first 6 months. Moreover, the heterogeneity of our study participants implies that our results can be applied only to patients similar to our cohort. Due to the relatively small number of VTE events in each tumor entity, we were not able to analyze the association between tumor stage and the occurrence of VTE in single tumor sites.
Based on the findings of this study, we recommend an equally high alertness for symptoms compatible with VTE in patients with regional disease as in those with metastatic cancer. Indeed, just as patients with distant metastases, patients with regional stage disease should also be regarded as being at high risk of VTE, especially in the presence of other risk factors for cancer-associated VTE.
We conclude that cancer patients with regional lymph node metastases have an increased risk of developing VTE. Elevated levels of predictive biomarkers in patients with regional stage disease underpin our results and are in line with the activation of the hemostatic system in the early phase of metastatic dissemination.
Acknowledgments
The authors would like to thank all the people who supported us in recruiting patients for the Vienna Cancer and Thrombosis Study (CATS). We are also grateful to Richard Rataj, Heidi Dude and Judith Raglhofer [Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University of Vienna (MUV)] for management of blood samples. We would also like to thank the members of the adjudication committee: Renate Koppensteiner, and Andrea Willfort-Ehringer (Department of Angiology, MUV); Sylvia Metz-Schimmerl (Department of Diagnostic Radiology, MUV); and Robert Dudczak (Department of Nuclear Medicine, MUV). Finally, we thank Tanja Altreiter (Clinical Division of Haematology and Haemostaseology, Department of Medicine I, MUV) for proof-reading this manuscript. The Vienna Cancer and Thrombosis Study was supported by grants from the Jubiläumsfonds of the Austrian National Bank (project numbers 10935 and 12739) and by an unrestricted grant from Pfizer Austria.
Footnotes
The online version of this article has a Supplementary Appenix.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Levitan N, Dowlati A, Remick SC, Tahsildar HI, Sivinski LD, Beyth R, et al. Rates of initial and recurrent thromboembolic disease among patients with malignancy versus those without malignancy. Risk analysis using Medicare claims data. Medicine (Baltimore). 1999;78(5):285–91 [DOI] [PubMed] [Google Scholar]
- 2.Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ., 3rd Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. 2000;160(6): 809–15 [DOI] [PubMed] [Google Scholar]
- 3.Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA. 2005;293(6):715–22 [DOI] [PubMed] [Google Scholar]
- 4.Sorensen HT, Mellemkjaer L, Olsen JH, Baron JA. Prognosis of cancers associated with venous thromboembolism. N Engl J Med. 2000;343(25):1846–50 [DOI] [PubMed] [Google Scholar]
- 5.Falanga A, Zacharski L. Deep vein thrombosis in cancer: the scale of the problem and approaches to management. Ann Oncol. 2005;16(5):696–701 [DOI] [PubMed] [Google Scholar]
- 6.Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902–11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Agnelli G, Gussoni G, Bianchini C, Verso M, Mandala M, Cavanna L, et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncol. 2009;10(10):943–9 [DOI] [PubMed] [Google Scholar]
- 8.Ay C, Vormittag R, Dunkler D, Simanek R, Chiriac AL, Drach J, et al. D-dimer and prothrombin fragment 1 + 2 predict venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2009;27 (25):4124–9 [DOI] [PubMed] [Google Scholar]
- 9.Ay C, Simanek R, Vormittag R, Dunkler D, Alguel G, Koder S, et al. High plasma levels of soluble P-selectin are predictive of venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). Blood. 2008;112(7):2703–8 [DOI] [PubMed] [Google Scholar]
- 10.Ay C, Pabinger I. Tests predictive of thrombosis in cancer. Thromb Res. 2010;125(2): 12–5 [DOI] [PubMed] [Google Scholar]
- 11.Khorana AA, Francis CW, Culakova E, Lyman GH. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer. 2005;104(12):2822–9 [DOI] [PubMed] [Google Scholar]
- 12.Simanek R, Vormittag R, Ay C, Alguel G, Dunkler D, Schwarzinger I, et al. High platelet count associated with venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). J Thromb Haemost. 2010;8(1):114–20 [DOI] [PubMed] [Google Scholar]
- 13.Vormittag R, Simanek R, Ay C, Dunkler D, Quehenberger P, Marosi C, et al. High factor VIII levels independently predict venous thromboembolism in cancer patients: the cancer and thrombosis study. Arterioscler Thromb Vasc Biol. 2009;29(12):2176–81 [DOI] [PubMed] [Google Scholar]
- 14.Ay C, Dunkler D, Simanek R, Thaler J, Koder S, Marosi C, et al. Prediction of venous thromboembolism in patients with cancer by measuring thrombin generation: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2011;29 (15):2099–103 [DOI] [PubMed] [Google Scholar]
- 15.Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008;111(10):4902–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ay C, Dunkler D, Marosi C, Chiriac AL, Vormittag R, Simanek R, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010;116(24):5377–82 [DOI] [PubMed] [Google Scholar]
- 17.Mandala M, Clerici M, Corradino I, Vitalini C, Colombini S, Torri V, et al. Incidence, risk factors and clinical implications of venous thromboembolism in cancer patients treated within the context of phase I studies: the ‘SENDO experience’. Ann Oncol. 2012;23(6): 1416–21 [DOI] [PubMed] [Google Scholar]
- 18.Sallah S, Wan JY, Nguyen NP. Venous thrombosis in patients with solid tumors: determination of frequency and characteristics. Thromb Haemost. 2002;87(4):575–9 [PubMed] [Google Scholar]
- 19.Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–64 [DOI] [PubMed] [Google Scholar]
- 20.Khorana AA, Connolly GC. Assessing risk of venous thromboembolism in the patient with cancer. J Clin Oncol. 2009;27(29): 4839–47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Connolly GC, Khorana AA. Emerging risk stratification approaches to cancer-associated thrombosis: risk factors, biomarkers and a risk score. Thromb Res. 2010;125(2):1–7 [DOI] [PubMed] [Google Scholar]
- 22.Chew HK, Davies AM, Wun T, Harvey D, Zhou H, White RH. The incidence of venous thromboembolism among patients with primary lung cancer. J Thromb Haemost. 2008; 6(4):601–8 [DOI] [PubMed] [Google Scholar]
- 23.Alcalay A, Wun T, Khatri V, Chew HK, Harvey D, Zhou H, et al. Venous thromboembolism in patients with colorectal cancer: incidence and effect on survival. J Clin Oncol. 2006;24(7):1112–8 [DOI] [PubMed] [Google Scholar]
- 24.Chew HK, Wun T, Harvey DJ, Zhou H, White RH. Incidence of venous thromboembolism and the impact on survival in breast cancer patients. J Clin Oncol. 2007; 25(1):70–6 [DOI] [PubMed] [Google Scholar]
- 25.Rodriguez AO, Wun T, Chew H, Zhou H, Harvey D, White RH. Venous thromboembolism in ovarian cancer. Gynecol Oncol. 2007;105(3):784–90 [DOI] [PubMed] [Google Scholar]
- 26.Rodriguez AO, Gonik AM, Zhou H, Leiserowitz GS, White RH. Venous thromboembolism in uterine cancer. Int J Gynecol Cancer. 2011;21(5):870–6 [DOI] [PubMed] [Google Scholar]
- 27.Sandhu R, Pan CX, Wun T, Harvey D, Zhou H, White RH, et al. The incidence of venous thromboembolism and its effect on survival among patients with primary bladder cancer. Cancer. 2010;116(11):2596–603 [DOI] [PubMed] [Google Scholar]
- 28.Sobin LH, Wittekind C. International Union against Cancer TNM: Classification of Malignant Tumours. 6th ed. New York: Wiley-Liss, 2002 [Google Scholar]
- 29.Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17(4):343–6 [DOI] [PubMed] [Google Scholar]
- 30.Blackwell K, Haroon Z, Broadwater G, Berry D, Harris L, Iglehart JD, et al. Plasma D-dimer levels in operable breast cancer patients correlate with clinical stage and axillary lymph node status. J Clin Oncol. 2000;18(3):600–8 [DOI] [PubMed] [Google Scholar]
- 31.Oya M, Akiyama Y, Okuyama T, Ishikawa H. High preoperative plasma D-dimer level is associated with advanced tumor stage and short survival after curative resection in patients with colorectal cancer. Jpn J Clin Oncol. 2001;31(8):388–94 [DOI] [PubMed] [Google Scholar]
- 32.Kwaan HC, Keer HN. Fibrinolysis and cancer. Semin Thromb Hemost. 1990;16(3): 230–5 [DOI] [PubMed] [Google Scholar]
- 33.Connolly GC, Khorana AA, Kuderer NM, Culakova E, Francis CW, Lyman GH. Leukocytosis, thrombosis and early mortality in cancer patients initiating chemotherapy. Thromb Res. 2010;126(2):113–8 [DOI] [PMC free article] [PubMed] [Google Scholar]