

Abstract
Dietary iron absorption is regulated by hepcidin, an iron regulatory protein produced by the liver. Hepcidin production is regulated by iron stores, erythropoiesis and inflammation, but its physiology when repeated blood loss occurs has not been characterized. Hepcidin was assayed in plasma samples obtained from 114 first-time/reactivated (no blood donations in preceding 2 years) female donors and 34 frequent (≥3 red blood cell donations in preceding 12 months) male donors as they were phlebotomized ≥4 times over 18–24 months. Hepcidin levels were compared to ferritin and hemoglobin levels using multivariable repeated measures regression models. Hepcidin, ferritin and hemoglobin levels declined with increasing frequency of donation in the first-time/reactivated females. Hepcidin and ferritin levels correlated well with each other (Spearman’s correlation of 0.74), but on average hepcidin varied more between donations for a given donor relative to ferritin. In a multivariable repeated measures regression model the predicted inter-donation decline in hemoglobin varied as a function of hepcidin and ferritin; hemoglobin was 0.51 g/dL lower for subjects with low (>45.7 ng/mL) or decreasing hepcidin and low ferritin (>26 ng/mL), and was essentially zero for other subjects including those with high (>45.7 ng/mL) or increasing hepcidin and low ferritin (>26 ng/mL) levels (P<0.001). In conclusion, hepcidin levels change rapidly in response to dietary iron needed for erythropoiesis. The dynamic regulation of hepcidin in the presence of a low levels of ferritin suggests that plasma hepcidin concentration may provide clinically useful information about an individual’s iron status (and hence capacity to tolerate repeated blood donations) beyond that of ferritin alone. Clinicaltrials.gov identifier: NCT00097006
Introduction
Iron is an essential nutrient necessary for erythropoiesis and cellular metabolism. Since there is no physiological mechanism for excretion of excess iron, the absorption of dietary iron is a tightly regulated process. Increased dietary iron absorption occurs when the body’s iron stores are depleted or when the bone marrow is under stress to produce new red blood cells.1 Decreased dietary iron absorption occurs during inflammatory conditions through processes that have evolved as an innate defense mechanism to rapidly sequester iron that may aid the growth of invading micro-organisms.2 The body responds to the various biochemical and environmental stimuli that alter dietary iron absorption by altering production of hepcidin, the central iron regulatory hormone.3
Hepcidin is a 25-amino acid peptide made by the liver which has primary control of dietary iron absorption.4 Hepcidin induces the internalization and degradation of ferroportin located on the basolateral surface of enterocytes that line the gastrointestinal tract. In the absence of ferroportin, dietary iron becomes trapped within enterocytes and is not transported into circulating blood.5 In addition to limiting dietary iron absorption, elevated plasma hepcidin also traps iron within hepatocytes and macrophages preventing use of these iron stores for incorporation into hemoglobin and erythrocyte production. Recent advances in the knowledge of hepcidin physiology have led to improved understanding of the biochemical mechanisms underlying several types of anemia and iron overload syndromes3 as well as to the development of new diagnostic tests6 and treatments7,8 for these disorders.
The Retrovirus Epidemiology Donor Study-II (REDS-II) Iron Status Evaluation (RISE) study provided the opportunity to further investigate hepcidin physiology in a cohort of blood donors with well-characterized iron status as they underwent repeated phlebotomy over a period of 18 to 24 months. The enrollment and longitudinal phases of the RISE study have been described in detail previously.9,10 During routine volunteer blood donation in the United States, approximately 500 mL of whole blood containing between 200 and 250 mg of iron is removed from the donor. This amount of iron is approximately equal to the total available iron stores in females and one-fourth of the available iron stores in males. Consequently, many individuals who frequently donate blood become iron deficient.10–12 Subjects undergoing repeated blood donation during the REDS-II RISE study represent a unique population to examine how plasma hepcidin levels change compared to ferritin and hemoglobin levels as iron stores are progressively depleted in healthy individuals.
Design and Methods
Study participants
The REDS-II RISE study was a longitudinal, multicenter study conducted between December 2007 and December 2009.9,10 Institutional Review Boards from all sites approved the study protocol. A subset of subjects was selected from the RISE cohort to examine the relationship between plasma hepcidin, plasma ferritin and venous hemoglobin levels. Initial screening criteria included: (i) participation at one of four REDS-II blood centers performing venous complete blood count and reticulocyte analysis using ADVIA analyzers (Siemens Healthcare Diagnostics, Deerfield, IL, USA); (ii) consent to store blood samples in the RISE repository; (iii) provision of two or more interim blood donations; and (iv) completion of a final visit during which a blood sample was collected and the survey conducted. Using these inclusion criteria 884 male and female donors were identified from the total 2425 male and female donors enrolled in RISE for potential hepcidin testing.
From this initial group of 884 donors, two groups of interest were selected based on gender, donor status and low hemoglobin deferral history; 114 females who were first-time or reactivated donors (had not donated blood in the preceding 24 months). This group was of interest as many were likely to have begun the study iron replete and then developed iron deficiency following repeated blood donation. From this same initial group of 884 female and male donors a second group of 34 frequent male donors (at least three donations in the 12 months prior to enrollment) with at least one low hemoglobin deferral during the study period were also selected for hepcidin testing. This group was of interest as they likely had severely depleted iron stores at enrollment with continued iron stress during the study. A total of 880 samples were tested for hepcidin (629 samples from the 114 first-time female donors and 251 samples from the 34 frequent male donors). Iron supplement use was determined by survey. Subjects indicating that they took a multiple vitamin with iron or an iron supplement at least once per week were categorized as taking iron supplements. Of the subjects chosen for hepcidin testing 67 used iron supplements; 44 reported daily use, 10 reported use 4- to 6-times per week, 10 reported use 1–3 times per week and 3 did not report the frequency.
Laboratory testing
At enrollment and at the final visit, one 7-mL and one 4.5-mL EDTA sample were collected. At most interim visits, a 7-mL EDTA sample was collected. Plasma ferritin was assayed on enrollment samples and on selected samples obtained during follow-up blood donations. Ferritin, a measure of total body iron stores, was determined by immunoassay (ADVIA Centaur, Siemens, Deerfield, IL. USA). Fingerstick hemoglobin or hematocrit values were obtained to qualify subjects for blood donation using methods that varied by center.13 Plasma hepcidin concentration was determined by an enzyme-linked immunosorbent assay (ELISA) at Intrinsic LifeSciences (San Diego, CA, USA).6 All test results were transferred electronically to Westat, which was responsible for data quality, compilation and analysis.
Statistical analyses
A detailed description of the statistical analyses used is provided in the Online Supplementary Marterial.
Results
Study participants
The demographic characteristics of the subjects included in the longitudinal regression models are presented in Online Supplementary Table S1. The sample included 114 first time/reactivated female donors. These 114 donors donated at least four times during RISE, including at completion of the final visit at the end of the study. Of these 114 women, 3 had ferritin >12 ng/mL and 27 had plasma ferritin >26 ng/mL at enrollment. Thus, about 25% of the women would have been considered iron-depleted at the beginning of the study. The sample also included 34 repeat male donors. These 34 males donated at least four times during RISE, including at completion of the final visit at the end of the study. In addition all the male donors had at least one hemoglobin deferral donation attempt during the longitudinal phase of RISE.
Correlation of ferritin and hepcidin levels
The relationship between ferritin and hepcidin levels was examined using a scatter plot of these measures on a log10 scale (Figure 1). There is a correlation between the two values with a Spearman’s correlation indicating a significant association (rs=0.74, P<0.001).
Figure 1.
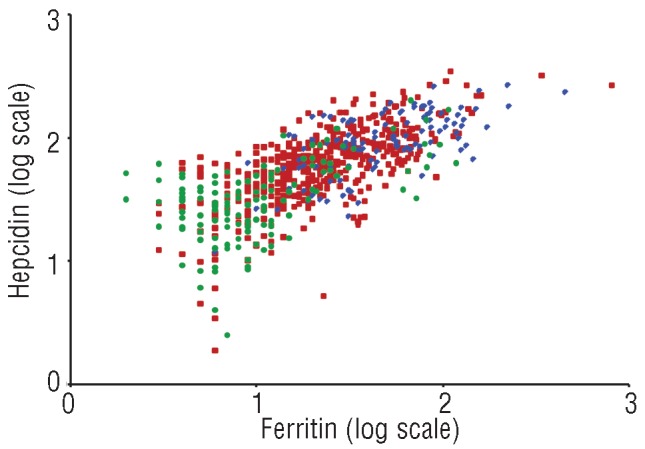
Scatter plot of log10 hepcidin (ng/mL) by log10 ferritin (ng/mL) demonstrates the correlation between the two plasma assays and the clustering of baseline female values in the upper right quadrant of the graph: ( ) Female baseline visits ( ) Female other visits ( ) Male visits.
Change in venous hemoglobin, ferritin and hepcidin levels with repeated donations by first-time females
Profile plots of donor laboratory measurements stratified by self-reported use of iron supplementation demonstrate the effect of repeated donations on venous hemoglobin, ferritin and hepcidin levels (Figure 2). Only the first-time/reactivated female donor cohort was used for these analyses to allow for comparison of how blood donation changes these parameters from baseline, non-donation values. Overall, 629 donations were given by the 114 female first-time donors. The figure illustrates the large amount of variability in the laboratory measures over repeated donations. The trend lines indicate a decrease in each laboratory measure over visits (P<0.001 for each laboratory measure); however, casual use of iron supplements had no effect (i.e. the black and red lines are statistically indistinguishable, P=0.95 for hemoglobin, P=0.73 for hepcidin, and P=0.12 for ferritin). Table 1 provides a model that quantifies the visit effect in terms of donation frequency and time since last donation while controlling for other factors (see next section of results). Of note, as estimated from Figure 2, the hepcidin within donor standard deviation of 0.25 on the log scale (or 78% on the natural scale) is statistically significantly larger (P<0.01) than the ferritin within donor standard deviation of 0.19 on the log scale (or 55% on the natural scale), evidenced by the apparent greater zigzag pattern of an individual’s hepcidin measures over visits compared to the zigzag pattern of an individual’s ferritin measures over visits.
Figure 2.
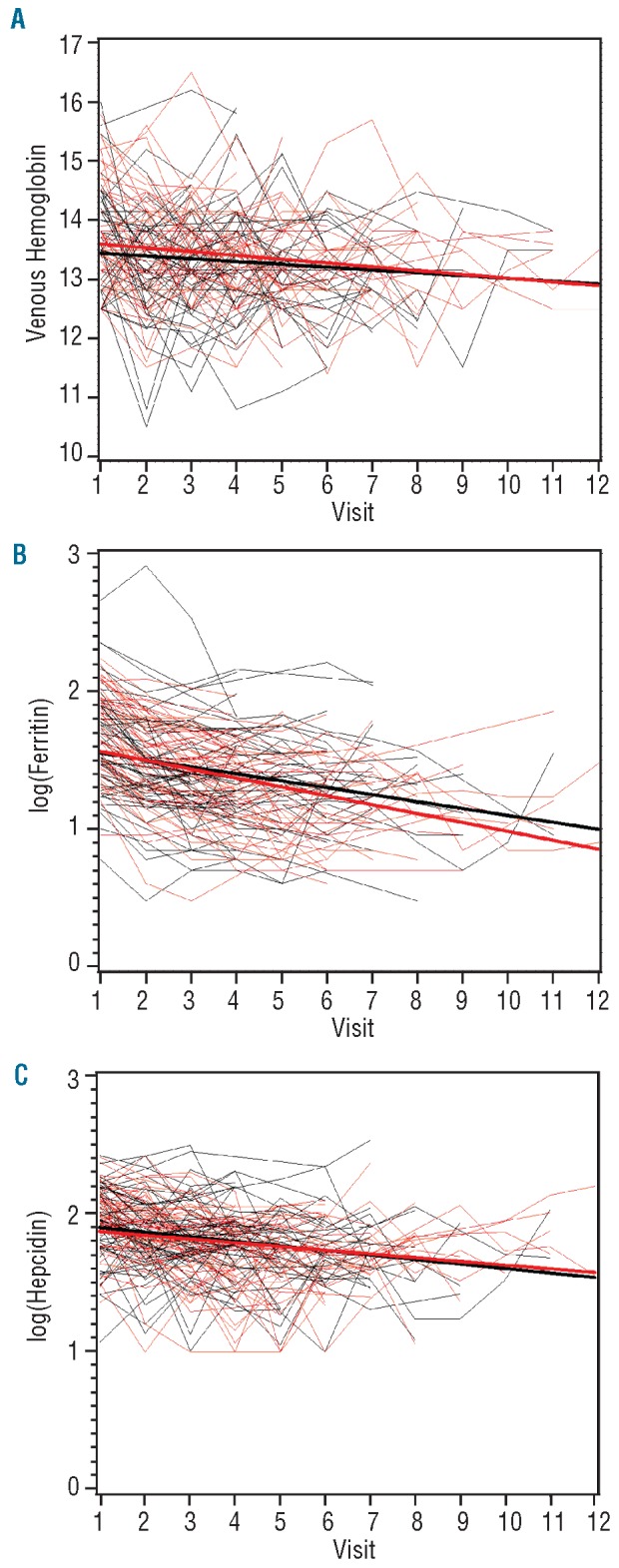
Trend lines of laboratory values from individual first-time/reactivated female donors over multiple visits. These trend lines help to illustrate the decrease in laboratory values over repeated blood donations; however, they are not adjusted for important modifiers, such as time between visits. Adjusted values along with P-values indicating statistical significance are presented in Table 1. Donations are stratified by those who reported use of iron supplements (black lines) and those who reported not using iron supplements (red lines). The bold lines are aggregate trend lines from donors reporting iron supplement use (black lines) and those who reported not using iron supplements (red lines). (A) Change in venous hemoglobin (g/dL); (B) change in log10 ferritin (ng/mL); (C) change in log10 hepcidin (ng/mL).
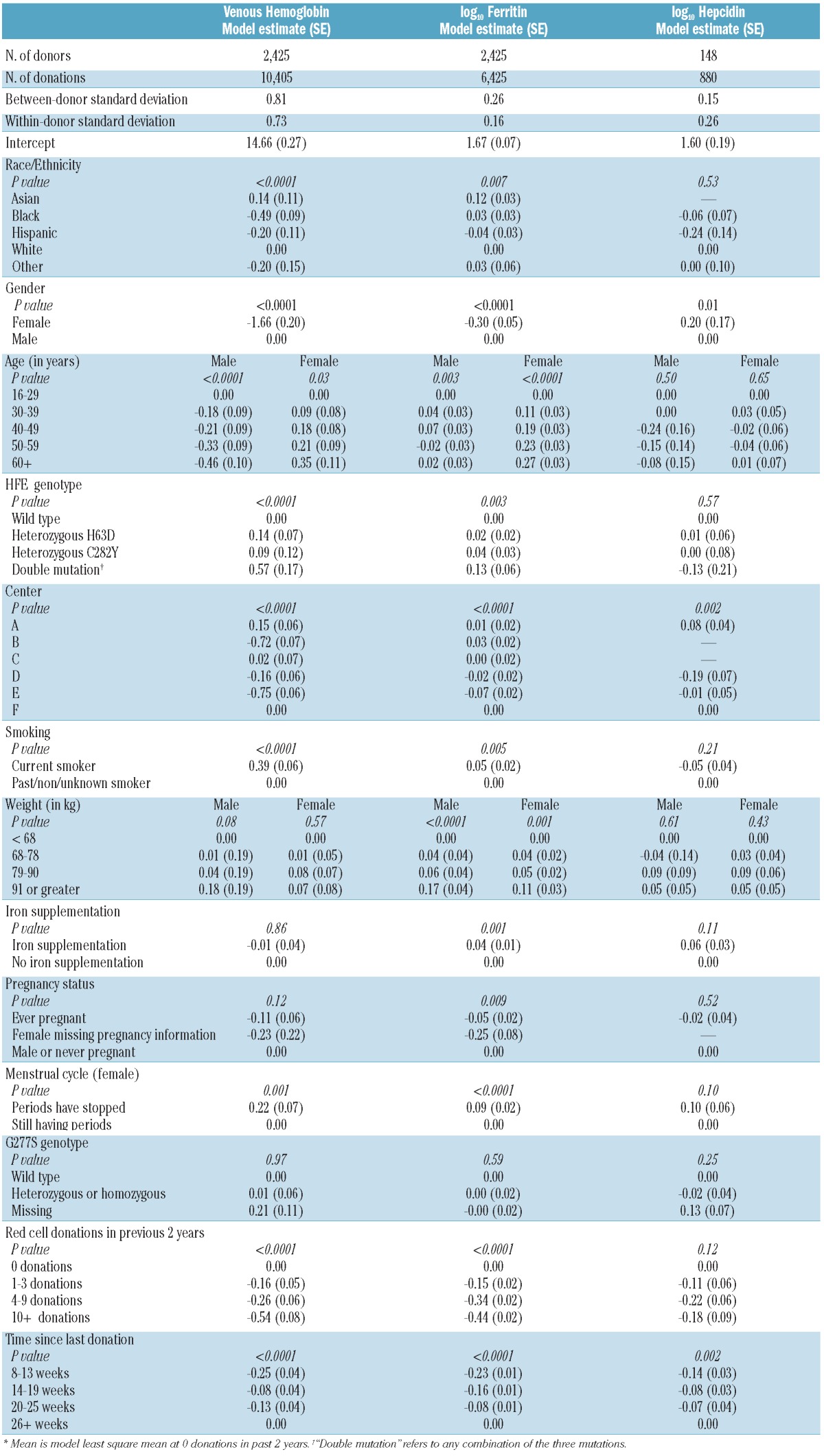
Table 1.
Parameter estimates for venous hemoglobin (g/dL), log10 ferritin (ng/mL) and log10 hepcidin (ng/mL).
Venous hemoglobin concentration declines with donations (Figure 2A). Based on the slope of the aggregate trend lines, the decrease in hemoglobin concentration is 0.05 g/dL with each donation in the average female first-time/reactivated donor regardless of whether they reported taking iron supplements at least once per week (test of different slopes, P=0.95). As has been reported previously,10–12 ferritin levels steadily decrease with donations (Figure 2B). Examination of the separate trend lines demonstrates that in most instances the ferritin concentration decreases with each visit for each individual donor (−0.05 log10 decrease per donation for those reporting use of iron supplements and 0.07 log10 decrease per donation for those not taking iron supplements). However, the apparent lesser slope for those reporting use of iron supplements is not statistically significant (test of different slopes, P=0.12). Nonetheless, the trend lines suggest that the average donor, regardless of iron supplement use, would have a ferritin concentration <10 ng/mL (log ferritin <1) and be severely iron deficient after 12 donations (Figure 2B). In contrast to ferritin, examination of the separate hepcidin trend lines (Figure 2C) demonstrates highly variable values in individual donors who made repeated donations, which is consistent with the greater standard deviation for hepcidin than for ferritin described in the previous paragraph. The trend lines show a decrease in hepcidin level of 0.03 log10 per donation (test of different slopes, P=0.73). These trend lines provide a visual aid to illustrate the decrease in laboratory measures over multiple blood donations. However, the lines do not quantify important factors affecting these laboratory measures, for example, the time between visits. To obtain a more accurate estimate of the relationship between hemoglobin, hepcidin and ferritin levels while controlling for iron supplementation and other characteristics, multivariable regression analyses were performed.
Effect of repeated donations on venous hemoglobin, ferritin and hepcidin levels in male and female donors
Multivariable repeated measures regression models have been developed previously for venous hemoglobin and ferritin14 and are included for convenience in Table 1. Major findings of these regressions are that hemoglobin and ferritin levels decrease with repeated donations in the preceding 2 years and that hemoglobin and ferritin levels take 26 weeks or more to recover after the last donation. A new model was developed for hepcidin using the same set of predictors (Table 1). Hemoglobin concentration was measured at all donations for all RISE donors (‘hemoglobin’ dataset). Ferritin level was measured at the first, the last, and some interval donations for all RISE donors (‘ferritin’ dataset). Hepcidin was measured for all donations when a sample was available for the donors selected for this study (‘hepcidin’ dataset). In supplemental analyses (not shown), ferritin regressions among the ‘hepcidin’ dataset generated specifically for this study and among the ‘ferritin’ dataset used in previous studies were statistically indistinguishable. Further, hemoglobin regressions among the ‘hepcidin’ dataset, among the ‘ferritin’ dataset, and among the ‘hemoglobin’ dataset were also statistically indistinguishable. Hence, there is no evidence of bias due to analyses of the different datasets presented in Table 1, and indicator variables for the varying datasets were dropped from the regressions presented.
In order to be consistent with the venous hemoglobin and ferritin models, interactions between recovery time and gender and/or donation intensity and gender were not developed for the hepcidin model. Although it is conceivable that such interactions may exist, the relatively small sample size for males in this study would poorly support this type of hepcidin model. Since a high proportion of donors reported using iron supplements at least once a week (42%), we were able explore models that included interactions between recovery time and iron supplementation and/or donation intensity and iron supplementation. There was some evidence of an interaction between iron supplementation and donation intensity, however this effect did not meet the statistical significance level of P=0.05. It is likely that not meeting the statistical significance criterion in this case may be attributed to the relatively small sample size of donors in whom hepcidin testing was performed. For consistency with the venous hemoglobin and ferritin models, and because of the P=0.05 criterion for statistical significance, we excluded interactions with iron supplementation from the hepcidin model reported in Table 1. The hepcidin regression indicates, like the hemoglobin and ferritin regressions, that hepcidin requires 26 weeks or longer to recover after the last donation. An effect due to repeated donations in the preceding 2 years was not statistically significant (although the smaller sample size of the hepcidin regression may have precluded detection of such an effect).
The standard deviations provided in Table 1 indicate the variability for each laboratory measure after controlling for the predictors in the model. The between-donor standard deviation indicates variability between any two alike donors. The within-donor standard deviation indicates variability from visit to visit for an individual donor. The hemoglobin concentration within the donor standard deviation (0.73) indicates hemoglobin changes of 0.73 g/dL or more from visit to visit are not unusual. The hepcidin within the donor standard deviation (0.26) indicates that hepcidin changes of 0.26 on the log scale (or 82% on the natural scale) are not unusual, while the ferritin within the standard deviation (0.16) indicates ferritin changes of 0.16 on the log scale (or 45% on the natural scale) are not unusual. Since the hepcidin and ferritin regressions were developed on the log scale, the percent standard deviation on the natural scale approximates the coefficient of variation on the natural scale. A key observation from these numbers is that the within-donor standard deviation is surprisingly larger for hepcidin than for ferritin, a finding that is consistent with the observations in Figure 2. The relatively large within-donor standard deviation of hepcidin suggests that there may be important predictor(s) missing from the model.
Race, gender, age, center, smoking status, menstrual status, HFE genotype, red cell donations in the preceding 2 years and the time since last donation were all statistically significant predictors of venous hemoglobin and ferritin levels in analyses performed using the entire RISE data set of 2,425 donors. Among these same characteristics, gender, center and the time since last donation were significant predictors of hepcidin even though only 148 subjects were included in the hepcidin analyses. It is likely that many of the other variables would also have been significant for hepcidin if the sample size had been larger.
Impact of hepcidin trend and concurrent ferritin levels on venous hemoglobin
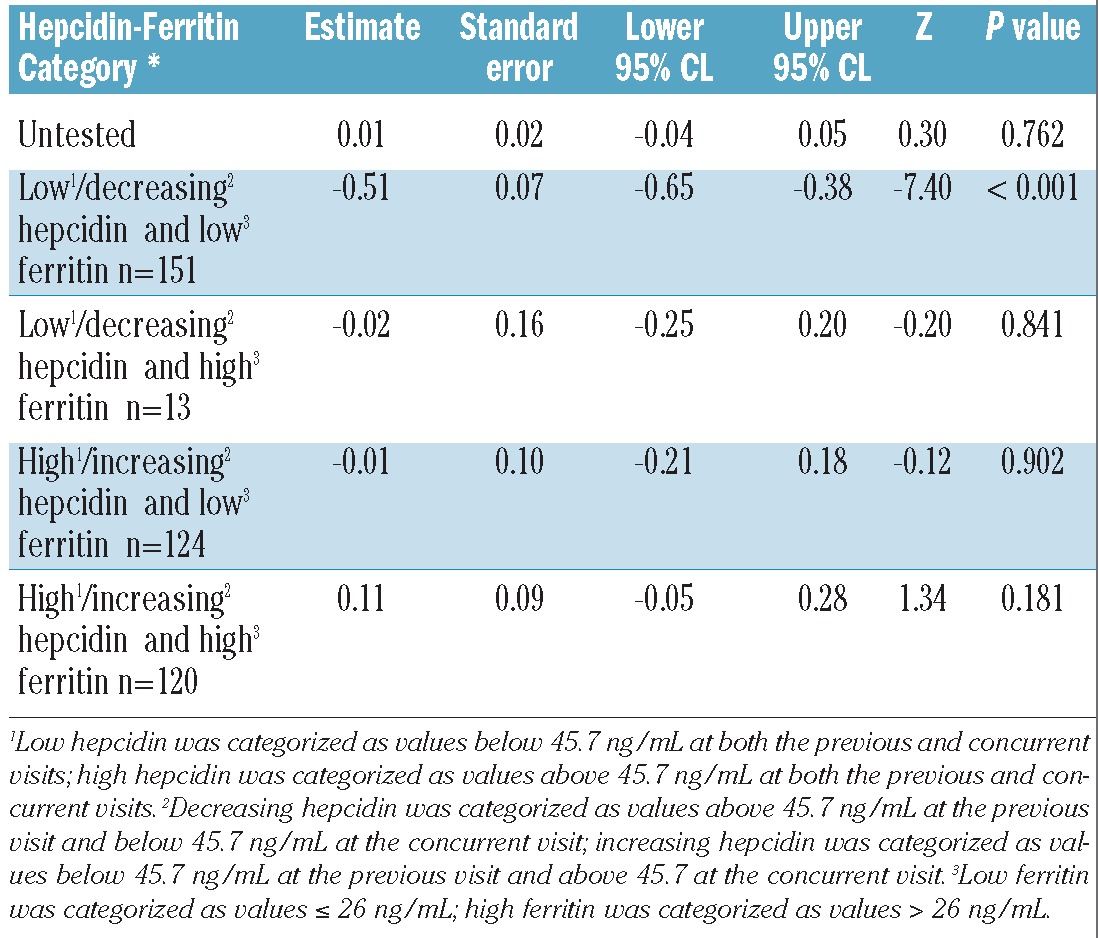
Low or decreasing levels of hepcidin between visits suggest a systemic response to iron deficiency. Decreased hepcidin would be expected to increase dietary iron absorption to compensate for iron lost during blood donation. A two-stage model was developed to assess how different combinations of hepcidin/hepcidin trend and ferritin predict inter-donation changes in hemoglobin. Results from this model (Table 2) indicate a significant decrease in venous hemoglobin of 0.51 g/dL (P<0.001) among donors with low or decreasing hepcidin and low ferritin levels, suggesting that this combination is indicative of a more profound iron deficit that affects erythropoiesis. There was no significant change in hemoglobin concentration in the other three groups of donors described in Table 2, which most notably includes donors with high hepcidin and low ferritin levels.
Table 2.
Parameter estimates for inter-donation change in venous hemoglobin (g/dL) (adding hepcidin and ferritin as covariates to the hemoglobin model presented in Table 1).
Discussion
Hepcidin physiology was examined using longitudinally acquired samples from 114 first-time female subjects and 34 repeat male subjects participating in the REDS-II RISE study of blood donors.9,10 The data demonstrate that plasma hepcidin and ferritin values tended to decrease as first-time donors underwent repeated donations and that these biomarkers correlated with each other. The correlation was not perfect, however, and hepcidin values tended to be more variable than ferritin. In addition, hepcidin values were significantly related to the time since the last donation (P=0.002), but not to the total number of donations during the preceding 2 years (P=0.12). Consequently, in some donors, hepcidin fully recovered during the inter-donation interval, while ferritin was much more likely to consistently fall with each subsequent donation. When hepcidin and ferritin values were analyzed in a two-stage multivariable repeated measures regression model, the donors presenting with low or decreasing hepcidin levels in the context of a concurrent low ferritin had a 0.51 g/dL lower hemoglobin concentration than all other donors, including those with high hepcidin levels in the context of concurrent low ferritin values.
Studies performed by Finch and colleagues in the 1950s found that dietary iron absorption is influenced by both the rate of erythropoiesis and the size of iron stores.15 The regulator of iron stores has the capacity to increase iron absorption up to about 2 mg per day, while the capacity of the erythroid regulator is much greater, perhaps up to 40 mg per day in patients with severe anemia receiving oral iron supplementation.1 Furthermore, the erythroid regulator has the capacity to drive continued dietary iron absorption, even in the presence of severe iron overload, to protect against iron-deficient erythropoiesis. This is best demonstrated in patients with β-thalassemia, who have a greatly expanded erythroid compartment and continued dietary iron absorption despite total body iron overload.16 Since hepcidin production is inappropriately low in these patients, it is thought that the erythroid regulator mediates its activity, at least in part, by decreasing hepcidin production.17 This concept is supported by studies of mice undergoing phlebotomy in the presence of inhibitors of erythropoiesis which have shown that increased erythropoiesis, as opposed to anemia, tissue hypoxia or erythropoietin, is necessary to reduce hepcidin synthesis and increase iron available for synthesis of new red blood cells.18,19
This dynamic regulation of hepcidin synthesis contrasts with that of ferritin, which is a specific measure of iron stores that does not vary with erythropoietic need for iron. These properties are reflected in the larger within-donor variation observed for hepcidin values than for ferritin values in the donors undergoing repeated phlebotomy studied here. Although these differences could partially result from intrinsic measurement variation of the two assays, they also reflect natural biological variations resulting from phlebotomy, as well as other influences, such as the use of oral iron supplements, which can alter circulating hepcidin values within hours.6 Thus, the data suggest that measurement of plasma hepcidin levels may provide clinically useful information about an individual’s iron status beyond that of ferritin alone. This has been demonstrated in a recent study of children with anemia in Africa by Prentice and co-workers.20 These investigators found that hepcidin concentration was the most consistent predictor of the incorporation of dietary iron into hemoglobin in patients with complex and competing signals for iron absorption, such as anemia, iron deficiency and inflammation. The studies presented here are limited because non-fasting samples were obtained at different times of the day, and there is diurnal variation in hepcidin concentration,6 and by the relatively small sample size, particularly for men, a highly selected population who had experienced deferral for low hemoglobin which is not necessarily representative of other males. Despite these limitations, the data demonstrate that plasma hepcidin tended to recover to normal levels in blood donors with sufficient iron available to support new red blood cell synthesis and maintain pre-donation hemoglobin values regardless of the amount of remaining iron stores. In contrast, plasma hepcidin concentration was low or decreasing in donors whose hemoglobin had not recovered to pre-donation levels. Thus, if hepcidin recovers following blood donation then adequate iron is probably available for new red blood cell synthesis during the inter-donation interval, whereas if hepcidin does not recover, it is an indicator of a lack of adequate iron available for new red blood cell synthesis with an associated decrease in hemoglobin. These results suggest that the erythroid regulator may be a more powerful regulator of hepcidin biosynthesis than the regulator of iron stores in healthy human subjects undergoing phlebotomy, as has previously been shown in mice.18
Previous studies by us, as well as others, have demonstrated that measures of iron status such as ferritin and reticulocyte hemoglobin content are useful predictors of future venous hemoglobin levels in frequent blood donors.14,21,22 Although hepcidin measurements correlate with serum ferritin levels and multivariable repeated measures regression analyses generated findings consistent with hepcidin serving as a hormonal sensor that rapidly changes in response to dietary iron needed for erythropoiesis, larger studies with a broader representation of donors are warranted to determine whether the distinctive rapid response of hepcidin to changes in iron status may contribute to the predictive model for the development of iron deficiency in frequent blood donors, and hence prove useful for guiding donation frequency criteria.
Appendix
The authors thank the staff at all six participating blood centers. Without their help, this study would not have been possible. Also, special thanks to Yu Sun from Westat for her work on the analyses.
The Retrovirus Epidemiology Donor Study-II was the responsibility of the following persons:
American Red Cross Blood Services, New England Region: R. Cable, J. Rios and R. Benjamin; American Red Cross Blood Services, Southern Region/Department of Pathology and Laboratory Medicine, Emory University School of Medicine: J.D. Roback; Hoxworth Blood Center, University of Cincinnati Academic Health Center: R.A. Sacher, S.L. Wilkinson and P.M. Carey; Blood Centers of the Pacific, University of California San Francisco, Blood Systems Research Institute: E.L. Murphy, B. Custer and N. Hirschler; The Institute for Transfusion Medicine. D. Triulzi, R. Kakaiya and J. Kiss; Blood Center of Wisconsin: J.L. Gottschall and A.E. Mast; Coordinating Center: Westat, Inc: J. Schulman and M. King; National Heart, Lung, and Blood Institute, NIH: G. Nemo; Central Laboratory: Blood Systems Research Institute: M.P. Busch and P. Norris.
Footnotes
The online version of this article has a Supplementary Appendix.
Funding
This work was supported by NHLBI contracts N01-HB-47168, -47169, -47170, -47171, -47172, -47174, -47175, and -57181.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Finch C. Regulators of iron balance in humans. Blood. 1994;84(6):1697–702 [PubMed] [Google Scholar]
- 2.Weinberg ED. Iron availability and infection. Biochim Biophys Acta. 2009;1790(7): 600–5 [DOI] [PubMed] [Google Scholar]
- 3.Ganz T, Nemeth E. Hepcidin and iron homeostasis. Biochim Biophys Acta. 2012; 1823(9):1434–43 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nicolas G, Bennoun M, Devaux I, Beaumont C, Grandchamp B, Kahn A, et al. From the cover: lack of hepcidin gene expression and severe tissue iron overload in upstream stimulatory factor 2 (USF2) knockout mice. PNAS. 2001;98(15):8780–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nemeth E, Tuttle MS, Powelson J, Vaughn MB, Donovan A, Ward DM, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science. 2004;306(5704):2090–3 [DOI] [PubMed] [Google Scholar]
- 6.Ganz T, Olbina G, Girelli D, Nemeth E, Westerman M. Immunoassay for human serum hepcidin. Blood. 2008;112(10):4292–7 [DOI] [PubMed] [Google Scholar]
- 7.Preza GC, Ruchala P, Pinon R, Ramos E, Qiao B, Peralta MA, et al. Minihepcidins are rationally designed small peptides that mimic hepcidin activity in mice and may be useful for the treatment of iron overload. J Clin Invest. 2011;121(12):4880–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ramos E, Ruchala P, Goodnough JB, Kautz L, Preza GC, Nemeth E, et al. Minihepcidins prevent iron overload in a hepcidin-deficient mouse model of severe hemochromatosis. Blood. 2012;120(18):3829–36 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cable RG, Glynn SA, Kiss JE, Mast AE, Steele WR, Murphy EL, et al. Iron deficiency in blood donors: analysis of enrollment data from the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion. 2011; 51(3):511–22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cable RG, Glynn SA, Kiss JE, Mast AE, Steele WR, Murphy EL, et al. Iron deficiency in blood donors: the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion. 2012;52(4):702–11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Finch CA, Cook JD, Labbe RF, Culala M. Effect of blood donation on iron stores as evaluated by serum ferritin. Blood. 1977;50(3):441–7 [PubMed] [Google Scholar]
- 12.Simon TL, Garry PJ, Hooper EM. Iron stores in blood donors. JAMA. 1981;245(20):2038–43 [PubMed] [Google Scholar]
- 13.Mast AE, Schlumpf KS, Wright DJ, Custer B, Spencer B, Murphy EL, et al. Demographic correlates of low hemoglobin deferral among prospective whole blood donors. Transfusion. 2010;50(8):1794–802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mast AE, Lee TH, Schlumpf KS, Wright DJ, Johnson B, Carrick DM, et al. The impact of HFE mutations on haemoglobin and iron status in individuals experiencing repeated iron loss through blood donation. Br J Haematol. 2012;156(3):388–401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bothwell TH, Pirzio-Biroli G, Finch CA. Iron absorption. I. Factors influencing absorption. J Lab Clin Med. 1958;51(1):24–36 [PubMed] [Google Scholar]
- 16.Rund D, Rachmilewitz E. Beta-thalassemia. N Engl J Med. 2005;353(11):1135–46 [DOI] [PubMed] [Google Scholar]
- 17.Papanikolaou G, Tzilianos M, Christakis JI, Bogdanos D, Tsimirika K, MacFarlane J, et al. Hepcidin in iron overload disorders. Blood. 2005;105(10):4103–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pak M, Lopez MA, Gabayan V, Ganz T, Rivera S. Suppression of hepcidin during anemia requires erythropoietic activity. Blood. 2006;108(12):3730–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vokurka M, Krijt J, Sulc K, Necas E. Hepcidin mRNA levels in mouse liver respond to inhibition of erythropoiesis. Physiol Res. 2006;55(6):667–74 [DOI] [PubMed] [Google Scholar]
- 20.Prentice AM, Doherty CP, Abrams SA, Cox SE, Atkinson SH, Verhoef H, et al. Hepcidin is the major predictor of erythrocyte iron incorporation in anemic African children. Blood. 2012;119(8):1922–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Radtke H, Meyer T, Kalus U, Rocker L, Salama A, Kiesewetter H, et al. Rapid identification of iron deficiency in blood donors with red cell indexes provided by Advia 120. Transfusion. 2005;45(1):5–10 [DOI] [PubMed] [Google Scholar]
- 22.Semmelrock MJ, Raggam RB, Amrein K, Avian A, Schallmoser K, Lanzer G, et al. Reticulocyte hemoglobin content allows early and reliable detection of functional iron deficiency in blood donors. Clin Chim Acta. 2012;413(7–8):678–82 [DOI] [PubMed] [Google Scholar]