

Abstract
Purpose
To investigate the analgesic effect and incidence of postoperative nausea and vomiting (PONV) between the opioid fentanyl and the non-steroidal anti-inflammatory drug ketorolac in patients who underwent eye amputation surgery.
Methods
Retrospective observational case series. Eighty-two patients underwent evisceration or enucleation surgery by one surgeon over a 2-year period. Fentanyl by intravenous patient-controlled analgesia (IV-PCA) at 20 µg/kg with 12 mg/kg ondansetron or intravenous ketorolac at 2 mg/kg/day was administered to patients at postoperative days 0, 1, and 2. The pain score was measured using an 11-point visual analog scale (VAS). The incidence of severe nausea requiring anti-emetics and the incidence of vomiting were reviewed.
Results
The mean postoperative VAS in the fentanyl group was significantly lower than that in the ketorolac group on the day of operation for both types of surgery (p = 0.001 and p = 0.004, respectively). At postoperative days 1 and 2, the mean VAS was not different between the two groups for either surgical type (p > 0.05 for both days). The mean VAS was significantly higher in eviscerated patients than in enucleated patients at postoperative days 0 and 1 in the fentanyl group (p = 0.023 and p = 0.016, respectively). However, this was not observed in the ketorolac group. The incidence of PONV was higher in the fentanyl group than in the ketorolac group, although this was not statistically significant for either surgical type (p > 0.05 for both groups).
Conclusions
Fentanyl was more effective as an analgesic than was ketorolac on the day of operation for both surgical types. There was no difference between the two analgesics on postoperative day 1. The analgesic effect of fentanyl in enucleated patients was significantly higher than in eviscerated patients at postoperative days 0 and 1. The use of fentanyl by IV-PCA was associated with greater PONV despite co-administration with anti-emetics, although this finding was not significant.
Keywords: Analgesic effect, Eye amputation, Fentanyl, Ketorolac, Postoperative nausea and vomiting
Eye amputation surgery, including evisceration and enucleation, is performed in patients with progressive phthisis bulbi, severe microphthalmia, endophthalmitis and intraocular neoplasm, or in patients who suffer from pain in a blind eye resulting from trauma, retinal detachment, or end-stage glaucoma [1]. Many patients who undergo these procedures may suffer from severe postoperative orbital pain, nausea, and vomiting that may delay a prompt recovery and their return to work. To minimize postoperative pain, diverse administration of analgesics, orally, intravenously, or intraorbitally, and intraoperative retrobulbar blockage have been used [2,3]. Fentanyl is a strong opioid analgesic usually administered intravenously by patient-controlled analgesia (IV-PCA) [4-6]. Postoperative nausea and vomiting (PONV) are the most distressing side effects of fentanyl, although anti-emetics are mixed with the PCA solutions [7-10]. Often, IV-PCA of fentanyl cannot be continued due to severe refractory PONV. This is especially true in patients who undergo eye amputation surgery. The use of fentanyl is sometimes problematic due to its emetic effect after eye amputation surgery in spite of its satisfactory pain-relieving effects. Though non-steroidal anti-inflammatory drugs have weaker analgesic effect than opioids, they can be used for safely controlling postoperative pain without physical or mental dependency, serious withdrawal, or PONV symptoms.
For these reasons, we investigated the efficacy and safety of IV-PCA fentanyl and IV ketorolac. The goal of our study was to determine which drug provided the strongest analgesic effect with the fewest side effects. We also compared the results between patients who underwent enucleation to those who underwent evisceration. To our knowledge, there has been no study investigating and comparing the postoperative pain-relieving efficacy and incidence of PONV in patients that were administered fentanyl in comparison with non-steroidal anti-inflammatory drugs (NSAIDs) after eyeball removal surgery.
Materials and Methods
A retrospective chart review of patients who underwent eye amputation surgery, including evisceration or enucleation, performed by one surgeon (JSY) at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea from January 2010 until December 2011 was performed. Informed consent was obtained from all patients in compliance with the World Medical Association Declaration of Helsinki. The pain score measurement used an 11-point visual analog scale (VAS; 0 = no pain, 10 = worst and intolerable pain) [11]. The incidence of severe nausea requiring anti-emetics, vomiting, or interrupting infusion of IV-PCA of fentanyl due to severe emesis was reviewed. A self-report of pain score was only achieved in patients over the age of 15 due to reliability, and patients under 15 years of age were excluded from this study. The survey of self-reported pain scores was conducted each evening from postoperative day 0 to day 2 after surgery. Pain was measured in the evening because that was when the last of the three daily doses of ketorolac was administered.
Postoperative pain was controlled by either IV-PCA fentanyl or IV ketorolac (Keromin; Hana Pharmaceuticals, Seoul, Korea). The IV-PCA (Automed 3400; Acemedical, Seoul, Korea) consisted of fentanyl dosed at 20 µg/kg body weight and ondansetron (Onseran; Yuhan Products, Seoul, Korea) dosed at 12 mg in normal saline at a total volume of 100 mL. It was administered at a basal rate of 2 mL/h, with a bolus dose of 0.5 mL and a lockout time of 15 minute. Due to the emetic side effects of fentanyl, anti-emetics were routinely mixed with fentanyl during IV-PCA. Ketorolac tromethamine was administered intravenously at three different times at 2 mg/kg body weight per day. The selection of analgesics was dependent upon the patient's decision and economic status. Informed consent was obtained for the use of IV-PCA fentanyl or IV ketorolac.
The evisceration or enucleation was performed under general anesthesia using standard techniques with the placement of hydroxyapatite (HA) orbital implants. During evisceration, a corneal button was removed after a 360° peritomy, and the intraocular contents were curetted with a 360° posterior sclerotomy performed to allow the placement of a larger HA implant and to facilitate vascularization [12]. During enucleation, the superior and inferior oblique muscles were cut and not reattached. The size of the HA implant was determined using sizing spheres, which allowed for sufficiently deep placement of the implant. After making three small holes in the HA implant using a 19-gauge needle, the anterior surface was wrapped with prepared autogenous sclera with the optic nerve stump facing forward or with a Neuro-Patch (polyester-urethane; Aesculap Inc., Tuttlingen, Germany) and fixed with 5-0 Vicryl sutures posteriorly [12,13]. Four windows (4 × 2 mm) were made at the attachment sites of the rectus muscles, and the implant was inserted into the orbit. Four rectus muscles were then brought into contact with the implant by passing a double-armed 5-0 Vicryl suture through the anterior lip of the window and tying the muscles to the opening. The last step was careful closure of the anterior and posterior Tenon's capsules and conjunctiva as separate layers.
Statistical analysis was performed with SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) using independent t-tests, paired t-tests, and Pearson's chi-square tests to compare the mean VAS and incidence of PONV between the two analgesic groups. Differences between evisceration and enucleation were also compared. A value of p < 0.05 was considered significant.
Results
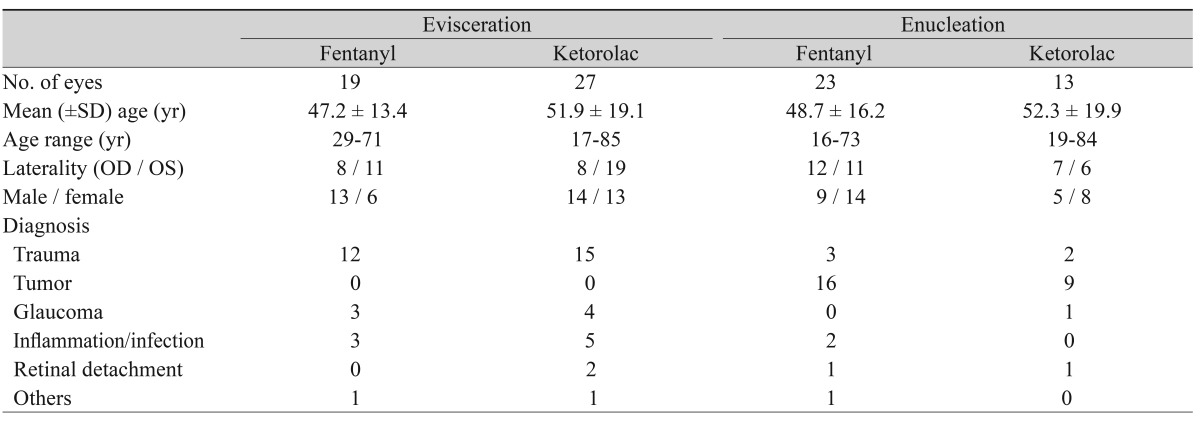
A total of 82 eyes from 82 patients (42 patients in the fentanyl group and 40 patients in the ketorolac group) were eligible for the study. Table 1 shows the demographic findings in patients given IV-PCA fentanyl or IV ketorolac after evisceration or enucleation.
Table 1.
Preoperative demographics for the evisceration and enucleation groups
In eviscerated patients (n = 46), the mean VAS at day 0 of surgery was significantly higher in patients using ketorolac (mean, 6.8; standard deviation [SD], 2.4) than in patients using fentanyl (mean, 3.6; SD, 1.5; p < 0.001; two sample t-test) (Table 2, Fig. 1A and 1B). However, the mean VAS values at days 1 and 2 were not significantly different between the two groups (p = 0.123 and 0.645, respectively). In addition, the pain score significantly decreased during the postoperative period in both analgesic groups (paired t-test at days 0 and 2, p = 0.004 in fentanyl group, p = 0.001 in ketorolac group).
Table 2.
Postoperative pain scores for the evisceration and enucleation groups (mean ± SD)

POD = postoperative day.
*Independent samples t-test; †Paired t-test (POD 0 and 2).
Fig. 1.

(A) Total postoperative pain analogue scores recorded by patients who received analgesics after evisceration or enucleation surgery. (B) Postoperative pain analogue scores compared by analgesic after eye amputation surgery. Circles (fentanyl group) and triangles (ketorolac group). (C) Postoperative pain analogue scores compared by surgical type. Circles (evisceration group) and triangles (enucleation group). POD = postoperative day.
Similarly, in patients who underwent enucleation surgery (n = 36), the mean VAS in the fentanyl group was significantly lower (mean, 2.5; SD, 1.3) than in the ketorolac group (mean, 5.7; SD, 3.2) at day 0 of surgery (p = 0.004, two sample t-test) (Table 2, Fig. 1A and 1B). However, the mean VAS values at days 1 and 2 were not significantly different between the two groups (p = 0.106 and p = 0.952, respectively). In addition, the pain score significantly decreased during the postoperative period in both analgesic groups (paired t-test at days 0 and 2, p = 0.007 in fentanyl group, p = 0.004 in ketorolac group).
In a comparison of postoperative pain scores between enucleated patients and eviscerated patients in the fentanyl group, enucleated patients had significantly lower postoperative pain than eviscerated patients at day 0 and day 1 (two sample t-test, p = 0.023 and p = 0.016, respectively) (Table 3, Fig. 1A and 1C). However, the mean pain scores were not different at day 2 (p = 0.550). The pain scores were not significantly different between eviscerated patients and enucleated patients in the ketorolac group through all postoperative days (two sample t-test; p = 0.225 at day 0, p = 0.419 at day 1, and p = 0.429 at day 2).
Table 3.
Postoperative pain scores for the fentanyl and ketorolac groups (mean ± SD)

POD = postoperative day.
*Independent samples t-test; †Paired t-test (POD 0 and 2).
The incidence of nausea requiring anti-emetics was higher in the fentanyl group (n = 10, 23.8%) than in the ketorolac group (n = 6, 15.0%), although these numbers are not significantly different (p = 0.361, Pearson's chi-square test) (Fig. 2). The incidence of vomiting was also higher in the fentanyl group (n = 9, 21.4%) than in the ketorolac group (n = 6, 15.0%), although there was not a significant difference (p = 0.856, Pearson's chi-square test) (Fig. 2). In each surgical type, the number of patients with severe nausea requiring anti-emetics was higher in the IV-PCA with fentanyl group (n = 5, 11.9%, eviscerated; n = 5, 11.9%, enucleated) than in the ketorolac group (n = 4, 10.0%; n = 2, 5.0%) (p = 0.528 and p = 0.841, respectively). Similarly, 9.5% (4 / 42) of patients in the IV-PCA fentanyl group who underwent evisceration suffered from vomiting compared to 10.0% (4 / 40) of patients in the ketorolac group; on the other hand, 11.9% (5 / 42) enucleation patients in the IV-PCA fentanyl group experienced vomiting compared to 5.0% (2 / 40) in the ketorolac group (p = 0.528 and p = 0.644, respectively). Of the 42 patients in the fentanyl group, temporal discontinuation of IV-PCA fentanyl was necessary in 11 patients (26.2%) due to severe PONV.
Fig. 2.

Incidence of postoperative nausea and vomiting symptoms during the study period. IV-PCA = intravenous patient-controlled analgesia.
Discussion
Postoperative pain, nausea, and vomiting are the most common and distressing complications after enucleation or evisceration surgery. Many studies on the management of postoperative morbidity have been investigated [4-8]. Optic nerve-related surgery such as eye amputation is related to severe orbital pain and to the oculo-emetic reflex. Prior studies indicate that approximately 50% to 75% of enucleated patients under general anesthesia experience nausea and vomiting on the day of surgery [2]. Therefore, immediate and proper control of pain, nausea, and vomiting is important for prompt recovery and psychological adaptation to loss of the eye.
Currently, intravenous analgesics have been widely administered for pain control. These pain relievers have some advantages over procedures such as indwelling intraorbital cannula or retrobulbar anesthetics in that they are simple and safe for patients. They also exhibit good pain-relieving effects. Opioids have strong analgesic effects, so they are generally used as part of routine postoperative pain management [4,5]. The benefit of IV-PCA, which offers greater patient satisfaction compared to intermittent intramuscular injection of opioids, has been studied [14,15]. Analgesics such as opioids are well known causes of PONV, which is the most common side effect. Sex (females have greater potential), smoking status, history of PONV and/or motion sickness, duration of surgery >1 hour, and the use of postoperative opioids were determined to be the strongest predictors of PONV [16,17]. To reduce PONV, an opioid-free pain management regimen can be effective [7,8]. The use of supplemental pain relievers such as cyclooxygenase-2-selective NSAIDs could reduce opioid use and the incidence of PONV [18,19]. Ketorolac tromethamine is a potent non-narcotic analgesic NSAID agent for treating moderate to severe pain and can be successfully used as an alternative to opiates. With its superior analgesic activity, reduced emetic effect, and non-sedative properties, it is safe and cost effective compared with opioids ($7.6 vs. $131.5 with total dosage, respectively). Thus, ketorolac is recommended as an appropriate alternative pain-control medication. We studied whether fentanyl-based PCA or ketorolac is a more effective management strategy for reducing pain, nausea, and vomiting symptoms after eyeball removal surgery.
We observed significant differences in the mean postoperative pain scores on the day of surgery between the fentanyl and ketorolac groups undergoing evisceration or enucleation surgery. There was significantly less pain noted by the fentanyl group vs. the ketorolac group (p = 0.001 and p = 0.004, respectively). This indicates that the onset of analgesia with fentanyl is immediate and very effective in patients with acute, severe pain. After the day of surgery, ketorolac also showed good analgesic effects similar to those of fentanyl. There were no differences in the mean pain scores between groups of patients undergoing either evisceration or enucleation (p > 0.05, both groups).
In patients in the fentanyl group, the mean VAS of eviscerated patients was significantly higher than that of enucleated patients at days 0 and 1 (p = 0.023 and p =0.016, respectively). Fentanyl provided a more significant analgesic effect in patients after enucleation than after evisceration. Also, in the ketorolac group, eviscerated patients experienced more pain than enucleated patients, but this difference was not significant. This may be because of the large standard deviation of the mean VAS in the ketorolac group caused by variability of assessed pain score after intravenous injection. Similar to a previous report [20], patients undergoing evisceration may experience more pain than those undergoing enucleation. This is thought to be due to exposure of ciliary nerves in evisceration but not in enucleation [3].
As mentioned above, female sex has been shown to be a predictive factor of PONV. There was a significant sex difference in PONV in the fentanyl group but not in the ketorolac group. In the fentanyl group (n = 42), the incidence of severe nausea in females (n = 8, 19.0%) was greater than in males (n = 2, 4.8%), and the female patients (n = 7, 16.7%) tended to have more frequent vomiting events than male patients (n = 2, 4.8%). These scores are significantly different (p = 0.011 and p = 0.024, respectively).
Because of the emetic effect of fentanyl, prophylactic use of anti-emetics such as ondansetron can be beneficial. Ondansetron binds to 5-HT3 receptors both in the central chemoreceptor trigger zone and the gastrointestinal tract to inhibit emetic symptoms and is widely used to prevent PONV [7,8,10]. This treatment was also used in our study. The recommended dose for prophylaxis is 4 to 8 mg IV in adults [21]. Therefore, we mixed 12 mg of ondansetron into the PCA. In another study, despite the addition of ondansetron to the PCA, the incidence of PONV in patients with fentanyl with PCA was reported to be as high as 58% [19]. In our study, ten of 42 patients receiving IV-PCA with fentanyl (23.8%) and six patients of the 40 patients receiving ketorolac (15.0%) had PONV symptoms requiring anti-emetics. The incidence of PONV with patients receiving fentanyl-based PCA was higher than those administered ketorolac in spite of adding anti-emetics to the PCA solution. However, this difference between the two groups was not significant. Prophylactic anti-emetic addition to the PCA made it difficult to compare the incidence of PONV between IV-PCA fentanyl and ketorolac alone. This was a limitation in our study. Overall, the PONV frequency in our study was much lower than that reported in prior studies, which reported 50% to 75% incidence of PONV after enucleation under general anesthesia [2]. This may be because we only recorded the incidence of severe nausea and vomiting requiring anti-emetics and excluded the cases of mild to moderate PONV. We could consider using a more objective measurement of PONV, such as a postoperative verbal numerical rating scale (VNRS), after eyeball removal surgery.
To assess the severity of pain or nausea and vomiting symptoms, patients were asked to assess the degree of severity. Therefore, one limitation in this study was dependent upon the patient recall during the study period. Patients were asked to estimate the level of pain only once a day in the evening. This does not reflect changes or variation of pain throughout the day.
Meanwhile, more effective options to reduce both postoperative pain and PONV after eye amputation surgery should be considered. As an alternative to opioids, µ-opioid receptor antagonists such as naloxone can also be considered to reduce emetic effects along with relieving pain [7]. A preliminary study comparing naloxone with placebo treatment demonstrated its effectiveness in reducing the incidence of PONV [22]. An additional method is synergic use of an NSAID-opioid combination. Prior reports demonstrated that the NSAID ketorolac combined with lower doses of the opioid fentanyl was associated with the same analgesic efficacy but reduced nausea and vomiting after thyroid surgery. This demonstrates the excellent opioid-sparing effect of ketorolac [19].
In conclusion, fentanyl was a significantly stronger pain reliever than ketorolac for the immediate postoperative period. However, the effect of pain reduction was similar to that of ketorolac after postoperative day 1 for eye amputation surgery. As patients receiving fentanyl-based PCA are more likely to experience PONV, more active administration of anti-emetics, if needed, should be considered.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Nakra T, Simon GJ, Douglas RS, et al. Comparing outcomes of enucleation and evisceration. Ophthalmology. 2006;113:2270–2275. doi: 10.1016/j.ophtha.2006.06.021. [DOI] [PubMed] [Google Scholar]
- 2.Yen KG, Elner VM, Musch DC, Nelson CC. Periocular versus general anesthesia for ocular enucleation. Ophthal Plast Reconstr Surg. 2008;24:24–28. doi: 10.1097/IOP.0b013e3181607461. [DOI] [PubMed] [Google Scholar]
- 3.Giligson A, Dolman PJ, Buffam F. Comparison of retrobulbar analgesics for evisceration. Ophthal Plast Reconstr Surg. 2002;18:258–260. doi: 10.1097/00002341-200207000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Peng PW, Sandler AN. A review of the use of fentanyl analgesia in the management of acute pain in adults. Anesthesiology. 1999;90:576–599. doi: 10.1097/00000542-199902000-00034. [DOI] [PubMed] [Google Scholar]
- 5.Ghodse AH, Edwards RE. Opioid analgesics and narcotic antagonists. Side Eff Drugs Annu. 1999;22:97–106. [Google Scholar]
- 6.Patanwala AE, Keim SM, Erstad BL. Intravenous opioids for severe acute pain in the emergency department. Ann Pharmacother. 2010;44:1800–1809. doi: 10.1345/aph.1P438. [DOI] [PubMed] [Google Scholar]
- 7.Fero KE, Jalota L, Hornuss C, Apfel CC. Pharmacologic management of postoperative nausea and vomiting. Expert Opin Pharmacother. 2011;12:2283–2296. doi: 10.1517/14656566.2011.598856. [DOI] [PubMed] [Google Scholar]
- 8.Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg. 2003;97:62–71. doi: 10.1213/01.ane.0000068580.00245.95. [DOI] [PubMed] [Google Scholar]
- 9.Song JW, Park EY, Lee JG, et al. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia. 2011;66:263–267. doi: 10.1111/j.1365-2044.2011.06648.x. [DOI] [PubMed] [Google Scholar]
- 10.Johnston KD, Quinlan J. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia. 2011;66:840–841. doi: 10.1111/j.1365-2044.2011.06830.x. [DOI] [PubMed] [Google Scholar]
- 11.McDowell I. Measuring health: a guide to rating scales and questionnaires. 3rd ed. New York: Oxford University Press; 2006. pp. 477–482. [Google Scholar]
- 12.Yoon JS, Lew H, Kim SJ, Lee SY. Exposure rate of hydroxyapatite orbital implants: a 15-year experience of 802 cases. Ophthalmology. 2008;115:566–572.e2. doi: 10.1016/j.ophtha.2007.06.014. [DOI] [PubMed] [Google Scholar]
- 13.Yoon JS, Lew H, Kook KH, Lee SY. The use of autogenous sclera as wrapping material in hydroxyapatite implantation. Ophthalmologica. 2009;223:7–11. doi: 10.1159/000161876. [DOI] [PubMed] [Google Scholar]
- 14.Walder B, Schafer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain: a quantitative systematic review. Acta Anaesthesiol Scand. 2001;45:795–804. doi: 10.1034/j.1399-6576.2001.045007795.x. [DOI] [PubMed] [Google Scholar]
- 15.Ballantyne JC, Carr DB, Chalmers TC, et al. Postoperative patient-controlled analgesia: meta-analyses of initial randomized control trials. J Clin Anesth. 1993;5:182–193. doi: 10.1016/0952-8180(93)90013-5. [DOI] [PubMed] [Google Scholar]
- 16.Koivuranta M, Laara E, Snare L, Alahuhta S. A survey of postoperative nausea and vomiting. Anaesthesia. 1997;52:443–449. doi: 10.1111/j.1365-2044.1997.117-az0113.x. [DOI] [PubMed] [Google Scholar]
- 17.Apfel CC, Laara E, Koivuranta M, et al. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91:693–700. doi: 10.1097/00000542-199909000-00022. [DOI] [PubMed] [Google Scholar]
- 18.Sinha VR, Kumar RV, Singh G. Ketorolac tromethamine formulations: an overview. Expert Opin Drug Deliv. 2009;6:961–975. doi: 10.1517/17425240903116006. [DOI] [PubMed] [Google Scholar]
- 19.Kim SY, Kim EM, Nam KH, et al. Postoperative intravenous patient-controlled analgesia in thyroid surgery: comparison of fentanyl and ondansetron regimens with and without the nonsteriodal anti-inflammatory drug ketorolac. Thyroid. 2008;18:1285–1290. doi: 10.1089/thy.2008.0007. [DOI] [PubMed] [Google Scholar]
- 20.Calenda E, Retourt A, Muraine M. Is evisceration of the eye more painful than enucleation? Eur J Anaesthesiol. 1999;16:117. doi: 10.1046/j.1365-2346.1999.00434.x. [DOI] [PubMed] [Google Scholar]
- 21.Tramer MR, Reynolds DJ, Moore RA, McQuay HJ. Efficacy, dose-response, and safety of ondansetron in prevention of postoperative nausea and vomiting: a quantitative systematic review of randomized placebo-controlled trials. Anesthesiology. 1997;87:1277–1289. doi: 10.1097/00000542-199712000-00004. [DOI] [PubMed] [Google Scholar]
- 22.Gan TJ, Ginsberg B, Glass PS, et al. Opioid-sparing effects of a low-dose infusion of naloxone in patient-administered morphine sulfate. Anesthesiology. 1997;87:1075–1081. doi: 10.1097/00000542-199711000-00011. [DOI] [PubMed] [Google Scholar]