

Abstract
Recent studies suggest that facial attractiveness indicates immune responsiveness in men and that this relationship is moderated by stress hormones which interact with testosterone levels. However, studies testing whether facial attractiveness in women signals their immune responsiveness are lacking. Here, we photographed young Latvian women, vaccinated them against hepatitis B and measured the amount of specific antibodies produced, cortisol levels and percentage body fat. Latvian men rated the attractiveness of the women's faces. Interestingly, in women, immune responsiveness (amount of antibodies produced) did not predict facial attractiveness. Instead, plasma cortisol level was negatively associated with attractiveness, indicating that stressed women look less attractive. Fat percentage was curvilinearly associated with facial attractiveness, indicating that being too thin or too fat reduces attractiveness. Our study suggests that in contrast to men, facial attractiveness in women does not indicate immune responsiveness against hepatitis B, but is associated with two other aspects of long-term health and fertility: circulating levels of the stress hormone cortisol and percentage body fat.
Keywords: beauty, cortisol, humans, immune, mate choice, sexual selection
1. Introduction
The growing field of evolutionary psychology reports a large body of evidence to suggest that standards of beauty are not arbitrary cultural conventions, pointing to, for example, cross cultural agreement in preferences for cues to health and fertility [1]. Furthermore, a number of studies suggest that facial preferences emerge early in childhood, before any cultural standards of beauty are likely to be assimilated, suggesting we have a strong inborn universal standard of facial beauty [2]. Evolutionary psychologists interpret preferences as strategies evolved owing to the selective benefits accrued to those who chose their mates based on these criteria (reviewed in Rhodes [3]). To argue that such preferences are adaptive, however, it is necessary to show that preferred traits serve as cues to fecundity, health or other traits that enhance fitness, and contribute to higher reproductive success.
Studies linking facial attractiveness and health records in men, however, have found only weak or no association between facial attractiveness and health (reviewed in Rhodes [3]). Recently, Rantala et al. [4] found that men's ability to produce antibodies in response to the hepatitis B vaccine correlated positively with facial attractiveness, suggesting that men's facial attractiveness indicates immunity in humans. Thus, by choosing men with attractive faces as partners, women may get direct benefits by avoiding contagion and indirect benefit by increasing health and immunity of their offspring. Because, in humans, both sexes are choosy, one could predict that female facial attractiveness may also be associated with immune defence and sex hormone levels. However, to our knowledge, studies testing association between female facial attractiveness, immune defence and stress hormone levels are lacking. Studies linking facial attractiveness with indices of health have led to mixed results: while certain studies have found some evidence that facially attractive women are healthier [5–7], other studies have found no association [8–10]. Rantala et al. [11] found that the link between facial attractiveness and immune response in men was mediated by their facial adiposity, not their masculinity (facial masculinity was however associated with immune response, independently of facial adiposity). Thus, we could expect that adiposity in women is associated with the strength of immunity and attractiveness. The aim of this study was to test whether facial attractiveness in women is associated with the strength of their immune response, circulating levels of the stress hormone cortisol and adiposity.
2. Material and methods
(a). Participants
Fifty-two Latvian women (mean age = 20.40, s.d. = 1.24; a subset of 65 women that completed all aspects of the study) not taking hormonal contraception and who reported a normal menstrual cycle participated in the study. They were instructed to visit the laboratory during the fertile phase of their menstrual cycle (20–14 days before the onset of their next period of menstrual bleeding) between 09.00 and 11.00. This method of assigning women to groups according to fertility is based on the assumption that the luteal phase lasts 14 days and that the fertile phase does not exceed 6 days [12]. Facial photographs were taken in standardized lighting conditions against a common background. We measured each participant's percentage body fat by using Omron Body Composition Monitor BF500.
(b). Immune and hormone assays
We measured the production of anti-hepatitis B surface antigen after hepatitis B vaccination. All participants received two doses of the Engerix B vaccine (Glaxosmithkline). Before the first vaccination, we collected 6 ml of venous blood to measure the baseline level of antibodies and hormone levels. One month after the vaccination, we again collected venous blood to measure antibody production after which participants received their second dose. One month after the second vaccination, we again collected venous blood to measure antibody production. Because only 19 out of 52 women produced antibodies after the first dose but 49 out of 52 women produced antibodies after second dose, we used only the amount of antibody produced after second vaccination in statistical analyses. Cortisol levels were measured from plasma samples taken during the first testing session (when a facial photograph was also taken; for more detailed methods see the electronic supplementary material).
(c). Facial rating
Eighteen heterosexual men from the University of Daugavpils, Latvia (mean age = 21.7 years, s.d. = 1.53) rated women's facial attractiveness. Photographs were presented in random order on a computer screen, and participants were asked to rate the attractiveness of each face. Attractiveness ratings were recorded on an 11-point scale (−5 = very unattractive, 0 = neutral and +5 = very attractive). After the trial, each participant was given a brief questionnaire to fill out, asking about his age, the ethnic origin of his mother and father, and sexual orientation. Inter-rater reliability was very high for facial attractiveness (Cronbach's α = 0.90), so average attractiveness scores for each female were computed. The data is deposited in the Dryad Repository: doi:10.5061/dryad.11vs5.
3. Results
Bivariate scatterplots indicate that cortisol and Hepatitis B antibody levels are linearly related to attractiveness, whereas percentage body fat shows a curvilinear relationship with attractiveness; women with an intermediate level of body fat were rated more attractive than women who had a low or high level of body fat. Cortisol and percentage fat and percentage fat2 was significantly correlated with attractiveness, whereas Hepatitis B antibody response was not (table 1). We fitted a simultaneous linear regression with attractiveness as the dependent variable and cortisol, hepatitis B antibody response, percentage body fat and percentage body fat2 as independent variables. Using Mahalanobis distance, we identified one multivariate outlier according to the p < 0.001 criterion [13]. The outlier individual was deleted from the analysis. Collinearity diagnostics identified multicollinearity (condition index = 45.07; with two variable values above 0.5) between percentage fat and percentage fat2, which was solved by centring the values as recommended by Tabachnick & Fidell ([13]; percentage fat was centred before calculating percentage fat2). The overall model significantly predicted attractiveness (F = 8.46, p < 0.001, r2 = 0.42). Cortisol levels, percentage fat and percentage fat2 significantly predicted female facial attractiveness, whereas Hepatitis B antibody response did not (table 2).
Table 1.
Pearson's correlations between all variables. Percentage fat2 was included because of the curvilinear relationship between percentage fat and attractiveness (n = 52).
| attractiveness | antibody response | cortisol | percentage fat | |
|---|---|---|---|---|
| attractiveness | — | |||
| antibody response | −0.006 | — | ||
| cortisol | −0.384** | −0.084 | — | |
| percentage fat | −0.407** | −0.003 | 0.098 | — |
| percentage fat2 | −0.481*** | −0.041 | 0.124 | 0.977*** |
*p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001.
Table 2.
Regression analysis of facial attractiveness judgements.
| β | t | p | effect size | |
|---|---|---|---|---|
| cortisol | −0.003 | −2.710 | 0.009 | −0.368 |
| percentage fat | −0.065 | −4.016 | <0.001 | −0.505 |
| percentage fat2 | −0.004 | −3.268 | 0.002 | −0.430 |
| antibody response | 0.000 | −0.955 | 0.345 | −0.138 |
4. Discussion
In contrast to findings in men [4], we found that women's immune response (i.e. ability to produce antibodies) is not associated with their facial attractiveness. Thus, there seems to be a sex difference in association between immune defence and facial attractiveness in humans. However, it would be premature to say that the facial attractiveness does not signal the strength of immune defence in women, because the immune system is complex and different components of the immune system trade-off with each other (e.g. the Th1 and Th2 arms of the adaptive immune system; [14]). It is possible that facial attractiveness signals a different arm of the immune defence in women than men. This remains to be tested in future studies.
Interestingly, facial attractiveness correlated negatively with plasma cortisol level suggesting that stress reduces attractiveness in women (figure 1). This supports previous findings from male faces, which show that cortisol is inversely related to facial attractiveness [15,16]. This has been interpreted as a mediator of condition-dependent cues in the face (e.g. to health) or as a signal of the ability to cope with stressors [15,16]. Perhaps then, low levels of cortisol also signal health in female faces. This would be consistent with many studies in humans that have found that stress has strong negative effect on health, including immune function, heart disease and susceptibility to cancer, etc. [17]. An alternative explanation is that facial attractiveness signals reproductive potential [18], which is mediated partly by stress hormones, because many studies have demonstrated that stress disturbs fertility through the inhibition of the hypothalamic–pituitary–gonadal axis leading to anovulation or luteal dysfunction [19].
Figure 1.
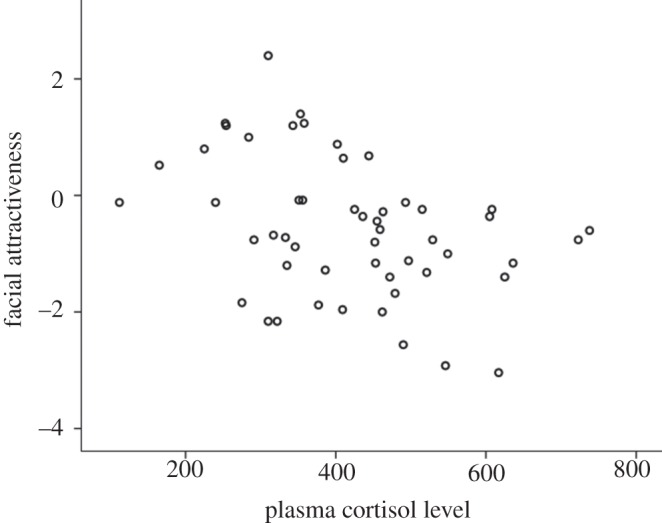
Correlation between facial attractiveness and plasma cortisol levels in women.
Consistent with previous studies [20], we found that body fat shows a significant curvilinear relationship with facial attractiveness. Facial attractiveness therefore has some association with long-term health and fertility. It is well known that obese and overweight individuals have more health problems compared with normal weight individuals [20–22]. Furthermore, body fat is associated with fertility, because both underweight and overweight women have reduced fertility compared with normal weight women [23], and Tinlin et al. [22] found a significant negative correlation between rated facial adiposity and the sex hormone progesterone. Interestingly, in contrast to our findings in men [12], women's adiposity did not correlate with immune responsiveness. Thus, there also seems to be a sex difference in the association between adiposity and immune function.
In summary, we found no association between female facial attractiveness and immune responsiveness in terms of hepatitis B antibody production. We did, however, find a significant association between female facial attractiveness and two other aspects of long-term health and fertility, plasma cortisol levels and percentage body fat. Together with previous studies, our study therefore suggests that facial attractiveness in women may not signal general immunocompetence, but maybe more probably long-term health and fertility.
Acknowledgements
The design of the study was approved by the Research Ethics Committee of the University of Daugavpils, Latvia.
The study was supported by Academy of Finland to M.J.R. F.R.M. was supported by a travel grant of the Carnegie Trust for the Universities of Scotland. V.C. was supported by a scarce skills postdoctoral fellowship from the South African National Research Foundation.
References
- 1.Langlois J, Kalakanis L, Rubenstein A, Larson A, Hallam M, Smoot M. 2000. Maxims or myths of beauty? A meta-analytic and theoretical review. Psychol. Bull. 126, 390–423 10.1037/0033-2909.126.3.390 (doi:10.1037/0033-2909.126.3.390) [DOI] [PubMed] [Google Scholar]
- 2.Rantala MJ, Marcinkowska UM. 2011. The role of sexual imprinting and the Westermarck effect in mate choice in humans. Behav. Ecol. Sociobiol. 65, 859–873 10.1007/s00265-011-1145-y (doi:10.1007/s00265-011-1145-y) [DOI] [Google Scholar]
- 3.Rhodes G. 2006. The evolutionary psychology of facial beauty. Ann. Rev. Psychol. 57, 199–226 10.1146/annurev.psych.57.102904.190208 (doi:10.1146/annurev.psych.57.102904.190208) [DOI] [PubMed] [Google Scholar]
- 4.Rantala MJ, Moore FR, Skrinda I, Krama T, Kivleniece I, Kecko S, Krams I. 2012. Evidence for the stress-linked immunocompetence handicap hypothesis in humans. Nat. Comm. 3, 694. 10.1038/ncomms1696 (doi:10.1038/ncomms1696) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gray AW, Boothroyd LG. 2012. Female facial appearance and health. Evol. Psychol. 10, 66–77 [PubMed] [Google Scholar]
- 6.Hume DK, Montgomerie R. 2001. Facial attractiveness signals different aspects of ‘quality’ in women and men. Evol. Hum. Behav. 22, 93–112 10.1016/S1090-5138(00)00065-9 (doi:10.1016/S1090-5138(00)00065-9) [DOI] [PubMed] [Google Scholar]
- 7.Shackelford TK, Larsen RJ. 1999. Facial attractiveness and physical health. Evol. Hum. Behav. 20, 71–76 10.1016/S1090-5138(98)00036-1 (doi:10.1016/S1090-5138(98)00036-1) [DOI] [Google Scholar]
- 8.Thornhill R, Gangestad S. 2006. Facial sexual dimorphism, developmental stability, and susceptibility to disease in men and women. Evol. Hum. Behav. 27, 131–144 10.1016/j.evolhumbehav.2005.06.001 (doi:10.1016/j.evolhumbehav.2005.06.001) [DOI] [Google Scholar]
- 9.Coetzee V, Barrett L, Greeff JM, Henzi SP, Perrett DI, Wadee AA, May R. 2007. Common HLA alleles associated with health, but not with facial attractiveness. PLoS ONE 2, e640. 10.1371/journal.pone.0000640 (doi:10.1371/journal.pone.0000640) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lie H, Rhodes G, Simmons L. 2008. Genetic diversity revealed in human faces. Evolution 62, 2473–2486 10.1111/j.1558-5646.2008.00478.x (doi:10.1111/j.1558-5646.2008.00478.x) [DOI] [PubMed] [Google Scholar]
- 11.Rantala MJ, Coetzee V, Moore FR, Skrinda I, Kecko S, Krama T, Kivleniece I, Krams I. 2013. Adiposity, compared with masculinity, serves as a more valid cue to immunocompetence in human mate choice. Proc. R. Soc. B 280, 20122495. 10.1098/rspb.2012.2495 (doi:10.1098/rspb.2012.2495) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wilcox AJ, Dunson D, Baird DD. 2000. The timing of the ‘fertile window’ in the menstrual cycle: day specific estimates from a prospective study. Br. Med. J. 321, 1259–1262 10.1136/bmj.321.7271.1259 (doi:10.1136/bmj.321.7271.1259) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tabachnick BG, Fidell LS. 2007. Using multivariate statistics. Boston, MA: Pearson [Google Scholar]
- 14.Keil D, Luebke RW, Pruett SB. 2001. Quantifying the relationship between multiple immunological parameters and host resistance: probing the limits of reductionism. J. Immunol. 167, 4543–4552 [DOI] [PubMed] [Google Scholar]
- 15.Moore FR, et al. 2011. Cues to sex- and stress-hormones in the human male face: functions of glucocorticoids in the immunocompetence handicap hypothesis. Horm. Behav. 60, 269–274 10.1016/j.yhbeh.2011.05.010 (doi:10.1016/j.yhbeh.2011.05.010) [DOI] [PubMed] [Google Scholar]
- 16.Moore FR, et al. 2011. Evidence for the stress-linked immunocompetence handicap hypothesis in human male faces. Proc. R. Soc. B 278, 774–780 10.1098/rspb.2010.1678 (doi:10.1098/rspb.2010.1678) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Glaser R, Kiecolt-Glaser JK. 2005. Science and society—stress-induced immune dysfunction: implications for health. Nat. Rev. Immunol. 5, 243–251 10.1038/nri1571 (doi:10.1038/nri1571) [DOI] [PubMed] [Google Scholar]
- 18.Thornhill R, Gangestad S. 1999. Facial attractiveness. Trends Cogn. Sci. 3, 452–460 10.1016/S1364-6613(99)01403-5 (doi:10.1016/S1364-6613(99)01403-5) [DOI] [PubMed] [Google Scholar]
- 19.Campagne DM. 2006. Should fertilization treatment start with reducing stress? Hum. Reprod. 21, 1651–1658 10.1093/humrep/del078 (doi:10.1093/humrep/del078) [DOI] [PubMed] [Google Scholar]
- 20.Coetzee V, Perrett DI, Stephen ID. 2009. Facial adiposity: a cue to health? Perception 38, 1700–1711 10.1068/p6423 (doi:10.1068/p6423) [DOI] [PubMed] [Google Scholar]
- 21.Pisunyer FX. 1993. Medial hazards of obesity. Ann. Int. Med. 119, 655–660 10.7326/0003-4819-119-7_Part_2-199310011-00006 (doi:10.7326/0003-4819-119-7_Part_2-199310011-00006) [DOI] [PubMed] [Google Scholar]
- 22.Tinlin RM, Watkins CD, Welling LLM, DeBruine LM, Al-Dujaili EAS, Jones BC. 2013. Perceived facial adiposity conveys information about women's health. Brit. J. Psychol. 104, 235–248 10.1111/j.2044-8295.2012.02117.x (doi:10.1111/j.2044-8295.2012.02117.x) [DOI] [PubMed] [Google Scholar]
- 23.Richedwards JW, et al. 1994. Adolescent body-mass index and infertility caused by ovulatory disorder. Am. J. Obst. Gynecol. 171, 171–177 10.1016/0002-9378(94)90465-0 (doi:10.1016/0002-9378(94)90465-0) [DOI] [PubMed] [Google Scholar]