

Abstract
INTRODUCTION
Bouveret's syndrome is a rare variant of gallstone ileus and describes gastric outlet obstruction secondary to an impacted stone in the duodenum. Its presentation is vague and clinical diagnosis is often difficult resulting in a delay in diagnosis.
PRESENTATION OF CASE
We report a patient who presented initially with non-specific symptoms and subsequently with features in keeping with acute pancreatitis, but eventually was found to have Bouveret's syndrome.
DISCUSSION
Different treatment strategies are discussed. Although endoscopic treatment combined with many newer modalities like lithotripsy have been tried, surgery remains the definitive management in the vast majority of cases.
CONCLUSION
Bouveret's syndrome is a rare condition, can also present as pancreatitis and often difficult to diagnose initially, but with appropriate treatment has a good outcome.
Keywords: Gallstone ileus, Bouveret's syndrome, Pancreatitis, Bowel obstruction
1. Introduction
Gallstone ileus is a rare cause of small bowel obstruction (SBO), representing 1–4% of all SBO.1,2 Bouveret's syndrome is a rare subcategory of gallstone ileus where a gallstone lodges itself into the duodenum and causes gastric outlet obstruction. It constitutes 2–3% of all gallstone related obstructions in the alimentary tract.3
2. Presentation of case
A 64 year old man was admitted with a week's history of nausea, and epigastric discomfort. His vital signs, clinical examination, and blood tests were unremarkable. He was treated conservatively for gastritis and was discharged home with arrangements for an outpatient oesophagogastroduodenoscopy (OGD).
He was re-admitted two weeks later with similar symptoms. On this admission, he also reported weight loss of about 10 kilograms and difficulty in tolerating oral intake. His abdomen was soft with mild tenderness in the epigastrium but with no peritoneal signs. His bloods revealed a WCC of 20.0 g/dl (normal 4–13). His amylase which was 73 units/L during his earlier admission had risen to 716 units/L (normal 0–90). His plain abdominal film showed calcified density in the right upper quadrant (Fig. 1). He was treated conservatively for acute pancreatitis and a CT was requested. This revealed a calcified intra-luminal abnormality in the second part of the duodenum (Figs. 2 and 3) with a dilated fluid filled proximal duodenum and stomach. The gallbladder was not visualised (patient had not had a previous cholecystectomy). He underwent an emergency OGD. At OGD a large gallstone was visualised in the second part of duodenum. It occupied more than 90% of the lumen and was impacted, hence endoscopic retrieval was not possible (Fig. 4). A midline laparotomy was therefore performed. Duodenum was kocherised and a longitudinal duodenotomy in the second part was made and the stone measuring about 7 cm × 3 cm, was removed (Fig. 5). No attempt was made to divide the adhesions in the right upper quadrant to visualise the gallbladder or the cholecystoduodenal fistula. The duodenum was closed in 2 layers with 2’0 polydioxanone sutures. His post-operative recovery was uneventful and he was entirely asymptomatic when reviewed in clinic 2 months later.
Fig. 1.

Plain abdominal film showing a calcified density in the right upper quadrant.
Fig. 2.
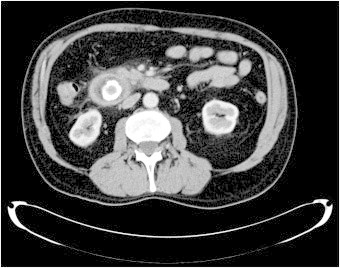
CT scan showing a well defined, calcified and intra-luminal abnormality at the junction of the second and third part of the duodenum (axial section).
Fig. 3.

CT scan showing a well defined, calcified and intra-luminal abnormality at the junction of the second and third part of the duodenum (coronal section).
Fig. 4.
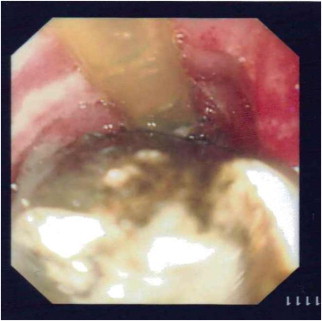
Photograph of endoscopic view of gallstone at the junction of second and third parts of duodenum.
Fig. 5.

Photograph of the gallstone that was removed measuring 7 cm × 3 cm.
3. Discussion
SBO secondary to gallstone ileus, although rare, is well recognised. Duodenal obstruction from gallstones (Bouveret's syndrome) presents with non-specific symptoms.4 Due to its rarity, the diagnosis and management remains challenging. The classical triad of distended stomach, pneumobilia and ectopic radio-opaque gallstone on plain radiograph (Rigler's triad) is seen in only a third of cases. CT, Ultrasound and endoscopy have been helpful diagnostic tools but in most cases, diagnosis is done only at laparotomy.4–6 Furthermore, to our knowledge there are only 2 reported cases in the literature where Bouveret's syndrome had presented with acute pancreatitis.7,8 We believe this patient developed pancreatitis because the large size of the stone almost blocked the lumen of the second part of the duodenum and closed the ampullary outlet causing pancreatic duct obstruction, a mechanism similar to acute pancreatitis secondary to gallstones impacted at the ampulla. However it is interesting to note that his liver function tests were normal. One possible explanation for this would be a slight movement of the stone within the duodenal lumen allowing for drainage of bile on an intermittent fashion (a ball-valve type effect). His pancreatitis settled soon after the stone was extracted with no early or delayed complications.
Endoscopic retrieval of stone from duodenum is generally accepted as first line treatment, though seldom successful.9,10 Other methods of stone destruction such as Intracorporeal Laser Lithotripsy (ILL),11 Extracorporeal Shockwave Lithotripsy (ESWL)12 or Intracorporeal Electrohydraulic Lithotripsy (IEHL)13 have all been used with limited success, however face the risk of causing a distal gallstone ileus secondary to smaller fragments.10,14
Surgery remains the definitive management in most cases, however there is much debate regarding operative management as to whether a one stage procedure with enterolithotomy, cholecystectomy and closure of fistula is superior to enterotolithotomy alone. Some report a lower morbidity and mortality with a one stage procedure1 whereas others advocate enterolithotomy alone.15 It must be noted however that most of the evidence is based upon distal gallstone ileus and therefore may not apply directly to proximal obstruction such as Bouveret's syndrome.16 We felt that further dissection in the right upper quadrant to visualise the gallbladder or the fistulous tract would risk vascular or biliary injuries and so performed only an enterolithotomy.
4. Conclusion
Bouveret's syndrome is a rare variant of gallstone ileus and its presentation as pancreatitis is an interesting feature. Non-specific clinical presentation of this syndrome makes diagnosis difficult, however when the diagnosis is made and appropriate treatment instituted, the final outcome is satisfactory.
Conflict of interest statement
Arif Zafar and other co-authors have no conflict of interest.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Arif Zafar – Main author/writer. Gemma Ingham – Co-Author/writer. Jainudeen. K. A. Jameel – Co-Author/writer and editor.
Contributor Information
Arif Zafar, Email: hawkeye_wolf@hotmail.com.
Jainudeen K.A. Jameel, Email: jainudeen.jameel@midyorks.nhs.uk.
References
- 1.Clavien P.A., Richon J., Burgan S., Rohner A. Gallstone ileus. British Journal of Surgery. 1990;77:737–742. doi: 10.1002/bjs.1800770707. [DOI] [PubMed] [Google Scholar]
- 2.Ayantunde A.A., Agrawal A. Gallstone ileus: diagnosis and management. World Journal of Surgery. 2007;31:1292–1297. doi: 10.1007/s00268-007-9011-9. [DOI] [PubMed] [Google Scholar]
- 3.Brennan G.B., Rosenberg R.D., Arora S. Bouveret syndrome. Radiographics. 2004;24:1171–1175. doi: 10.1148/rg.244035222. [DOI] [PubMed] [Google Scholar]
- 4.Cappell M.S., Davis M. Characterization of Bouveret's syndrome: a comprehensive review of 128 cases. American Journal of Gastroenterology. 2006;101:2139–2146. doi: 10.1111/j.1572-0241.2006.00645.x. [DOI] [PubMed] [Google Scholar]
- 5.Tuney D., Cimsit C. Bouveret's syndrome: CT findings. European Radiology. 2000;10:1711–1712. doi: 10.1007/s003300000444. [DOI] [PubMed] [Google Scholar]
- 6.Trubek S., Bhama J.K., Lamki N. Radiological findings in Bouveret's syndrome. Emergency Radiology. 2001;8:335–337. [Google Scholar]
- 7.Fenchel R.F., Krige J.E., Bornman P.C. Bouveret's syndrome complicated by acute pancreatitis. Digestive Surgery. 1999;16:525–527. doi: 10.1159/000018782. [DOI] [PubMed] [Google Scholar]
- 8.Sica G.S., Sileri P., Gaspari A.L. Laparoscopic treatment of Bouveret's syndrome presenting as acute pancreatitis. JSLS. 2005;9:472–475. [PMC free article] [PubMed] [Google Scholar]
- 9.Schweiger F., Shinder R. Duodenal obstruction by a gallstone (Bouveret's syndrome) managed by endoscopic stone extraction: a case report and review. Canadian Journal of Gastroenterology. 1997;11:493–496. doi: 10.1155/1997/182768. [DOI] [PubMed] [Google Scholar]
- 10.Wittenburg H., Mossner J., Caca K. Endoscopic treatment of duodenal obstruction due to a gallstone (“Bouveret's syndrome”) Annals of Hepatology. 2005;4:132–134. [PubMed] [Google Scholar]
- 11.Holl J., Sackmann M., Hoffmann R., Schüssler P., Sauerbruch T., Jüngst D. Shock-wave therapy of gastric outlet syndrome caused by a gallstone. Gastroenterology. 1989;97:472–474. doi: 10.1016/0016-5085(89)90086-3. [DOI] [PubMed] [Google Scholar]
- 12.Dumonceau J.M., Delhaye M., Devière J., Baize M., Cremer M. Endoscopic treatment of gastric outlet obstruction caused by a gallstone (Bouveret's syndrome) after extracorporeal shock-wave lithotripsy. Endoscopy. 1997;29:319–321. doi: 10.1055/s-2007-1004197. [DOI] [PubMed] [Google Scholar]
- 13.Zielinski M.D., Ferreira L.E., Baron T.H. Successful endoscopic treatment of colonic gallstone ileus using electrohydraulic lithotripsy. World Journal of Gastroenterology. 2010;16:1533–1536. doi: 10.3748/wjg.v16.i12.1533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gencosmanoglu R., Inceoglu R., Baysal C., Akansel S., Tozun N. Bouveret's syndrome complicated by a distal gallstone ileus. World Journal of Gastroenterology. 2003;9:2873–2875. doi: 10.3748/wjg.v9.i12.2873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Doko M., Zovak M., Kopljar M., Glavan E., Ljubicic N., Hochstädter H. Comparison of surgical treatments of gallstone ileus: preliminary report. World Journal of Surgery. 2003;27:400–404. doi: 10.1007/s00268-002-6569-0. [DOI] [PubMed] [Google Scholar]
- 16.Doycheva I, Limaye A, Suman A, Forsmark CE, Sultan S. Bouveret's syndrome: case report and review of the literature. Gastroenterol Res Pract 2009;914951. Available from http://www.ncbi.nlm.nih.gov/pubmed/19360112. [DOI] [PMC free article] [PubMed]