

Abstract
INTRODUCTION
Primary endocrine cell tumors in the gallbladder are uncommon, and the coexistence of an endocrine cell tumor and adenocarcinoma, squamous cell carcinoma, and sarcomatoid components is extremely rare.
PRESENTATION OF CASE
A rare case of adeno-endocrine cell carcinoma of the gallbladder in an 81-year-old woman is reported. Abdominal ultrasonography (US) revealed a hypo-echoic, solid tumor, 2.0 cm × 1.8 cm in size, at the fundus of the gallbladder. On computed tomography (CT), the tumor was well-enhanced, well-demarcated, and homogeneous. The tumor, which was papillary, protruded into the gallbladder with no direct invasion to the liver. The tumor was diagnosed as gallbladder carcinoma; its depth appeared not to pass the subserosa layer. A cholecystectomy and hepatic bed resection with regional lymph node dissection were performed. Histologically, the tumor consisted of several components, including well to poorly differentiated papillary and tubular adenocarcinoma with squamous and sarcomatoid differentiations, and endocrine cell carcinoma. Histochemical studies of these tumor cells were positive for chromogranin A, synaptophysin, and cluster of differentiation 56 (CD56). The lymph node consisted of metastatic adeno-endocrine carcinoma. The patient survived and has remained disease-free for 4 years without adjuvant chemotherapy.
DISCUSSION
Adeno-endocrine cell carcinoma of the gallbladder generally has a poor prognosis.
CONCLUSION
The present case suggests that adeno-endocrine cell carcinoma with various components may be derived from a common precursor cell. This observation would require further investigation.
Keywords: Composite tumor, Gallbladder, Adeno-endocrine cell carcinoma
1. Introduction
Endocrine cell carcinoma is most commonly found in the gastrointestinal tract, especially in the appendix, and the lung. Tahara et al. proposed the term “endocrine cell carcinoma” in 1988, and it was classified into classical carcinoid and endocrine cell carcinoma with more malignant potential.1 Primary endocrine cell tumors in the gallbladder are uncommon, and the coexistence of an endocrine cell tumor and adenocarcinoma, squamous cell carcinoma, and sarcomatoid components is extremely rare. The present case may represent the first reported case of a varied “composite” tumor in the gallbladder. A review of the literature is also provided.
2. Presentation of case
An 81-year old woman was admitted to our hospital in August 2005 after she completed a routine annual medical examination. She had been treated for diabetes mellitus and hypertension. No clinical signs of tumor hormonal activity were observed. Physical examination was also unremarkable. Abdominal US showed a protruding, hypo-echoic mass with an irregular surface at the fundus of the gallbladder, and some gallbladder stones were detected (Fig. 1). The results of laboratory tests on admission revealed that aminotransferase, alanine aminotransferase, γ-guanosine triphosphate, and alkaline phosphatase levels were within the normal ranges. The levels of tumor markers, such as carbohydrate antigen 19-9 and carcinoembryonic antigen, were also within the normal ranges. On CT, the tumor was irregular, homogeneous, and strongly enhanced, and it appeared to extend no deeper than the subserosa layer. The lymph node behind the head of the pancreas was swollen (Fig. 2). T2-weighted magnetic resonance imaging (MRI) showed a papillary high-intensity tumor that did not directly invade the liver (Fig. 3). On laparotomy, neither ascites nor peritoneal dissemination was observed. A cholecystectomy and hepatic bed resection, including regional lymph node dissection, were performed. The operation time was 3 h and 12 min. Blood loss was 150 ml Macroscopically, the tumor was 20 × 40 mm in size, and it appeared to be an elastic, hard, white mass at the fundus of the gallbladder (Fig. 4). All specimens were processed in the routine manner for paraffin embedding, and 5-μm-thick sections were cut and stained with hematoxylin and eosin. Histologically, the tumor proliferation reached to the subserosa layer, but the liver parenchyma was intact. There was no vascular or lymphatic permeation. The tumor consisted of several components, well to poorly differentiated papillary and tubular adenocarcinoma with squamous and sarcomatoid components and endocrine cell carcinoma. Histochemical studies of these tumor cells were positive for chromogranin A, synaptophysin, and CD56 (Figs. 5a–c, 6a–c). In the enlarged lymph node, metastatic carcinoma cells were detected, although perineural tumor invasion was not noted.
Fig. 1.

Abdominal ultrasonography reveals a hypo-echoic, solid tumor, 2.0 × 1.8 cm, at the fundus of the gallbladder.
Fig. 2.
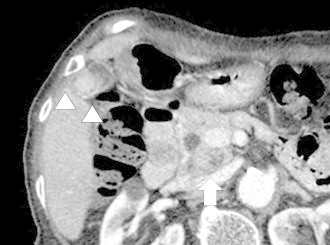
CT reveals that the tumor is irregular (white arrowheads), homogeneous, and enhanced, and the lymph node behind the head of the pancreas head is swollen (white arrow).
Fig. 3.
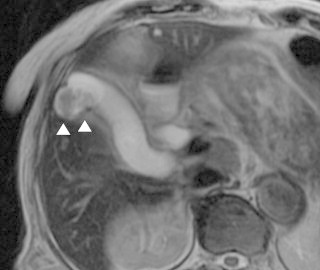
T2-weighted MRI shows a papillary high-intensity tumor that does directly invade the liver (white arrowheads).
Fig. 4.
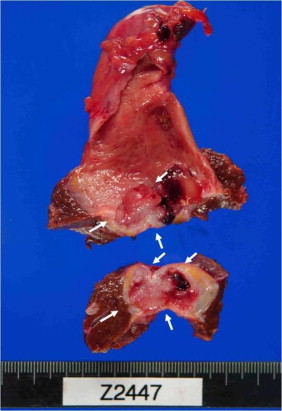
Macroscopic observation shows that the specimen is an elastic, hard, white tumor at the fundus of the gallbladder (white arrow).
Fig. 5.
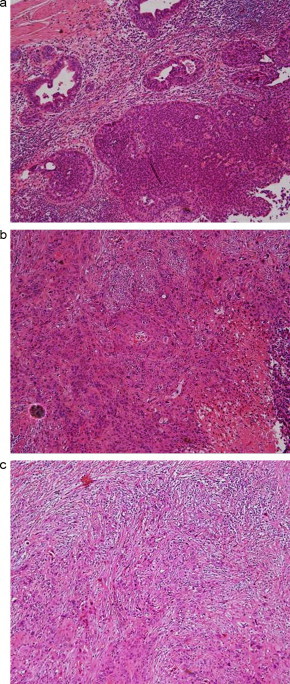
(a–c): Histologically, the gallbladder tumor consists of three components: (a) well to poorly differentiated papillary adenocarcinoma; (b) squamous differentiation; and (c) sarcomatoid differentiation.
Fig. 6.
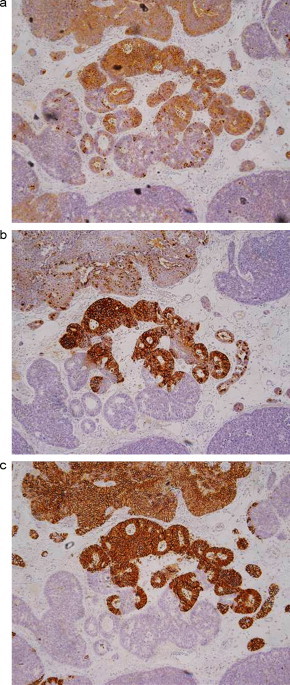
(a–c): (a) The tumor cells are positive for synaptophysin (synaptophysin, ×200). (b) In addition, the tumor cells show positivity for chromogranin (chromogranin, ×200). (c) The tumor cells are also positive for CD56 (CD56, ×200).
Thus, a nonfunctioning and well to poorly differentiated endocrine adenocarcinoma with various differentiations was diagnosed based on the above pathologic findings. The patient was discharged on the 13th day after the operation without any complications. This patient underwent a curative surgical resection and remains disease-free 4 years later.
3. Discussion
To the best of our knowledge, this is very rare report of a composite tumor of adeno-endocrine cell and squamous cell carcinoma and sarcoma arising from the gallbladder. The typical classification of carcinoid tumors is based on their embryonic gut origin, but the literature shows widespread and inconsistent dualistic classifications of “typical” versus “atypical” carcinoid with the usual reference to their degree of differentiation. “Typical” carcinoids, by definition, are tumors with neuroendocrine differentiation and the classical histological architecture of trabecular, insular, or ribbon-like cell clusters, with no or minimal cellular pleomorphism and sparse mitoses.2 “Atypical” carcinoids refer to aggressive forms of poorly differentiated carcinoid tumors with increased mitotic activity and absent or limited necrosis with a poor prognosis.2,3
Joel first described a case of carcinoid tumor of the gallbladder in 1929.4 Since then, almost 50 cases, including the present case, have been reported, accounting for 0.2% of all carcinoid tumors.5–10 The typical clinical symptoms are jaundice and right upper quadrant pain. In most cases, the diagnosis was incidental after histological examination of gallbladder specimens. The difficulty of making the current diagnosis was due to the similarity of the radiological findings to those of carcinoma of the gallbladder.
The origin of adeno-endocrine cell carcinoma of the gallbladder is still unclear. Some studies suggest that genetically unstable progenitor cells or undifferentiated, omnipotent stem cells can play not only an important role in embryonic development, but also in oncogenesis. This supports the hypothesis that the histogenesis of carcinoid tumors is that they originate from multipotential stem cells that have the ability to differentiate towards neuroendocrine and glandular cell types.6 In the current case, the apparent transitional zone was not detected, but the presence of various components, such as adeno-endocrine cell and squamous and sarcomatoid differentiations, in the same tumor suggests that they may arise from a common precursor cell.7,11 Only four cases of composite tumor of adeno-endocrine cell carcinoma and squamous cell carcinoma of the gallbladder have been reported (Table 1).12–15 The present case is the first to show multidirectional differentiation, with squamous and sarcomatoid components.
Table 1.
Previous case reports of composite tumor (adeno-endocrine cell carcinoma and squamous cell carcinoma) of the gallbladder.
| No | Author | Year | Age (years) | Sex | Size (mm) | Depth | Metastasis | Therapy | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Iida et al. | 1992 | 62 | F | 6.5 | hinv (+) | Liver | Cholecystectomy Resection of the tumor |
5 Months Deceased |
| 2 | Maitra et al. | 2001 | 82 | F | 10 | ss | Liver | ND | 8 Months Deceased |
| 3 | Wakabayashi | 2003 | 71 | F | 100 | se | None | Extended right lobectomy Partial resection of colon |
36 Months Alive |
| 4 | Mori | 2005 | 70 | F | 36 × 15 | ss | LN | Cholecystectomy Resection of liver bed |
32 Months Deceased |
| 5 | Present case | 2013 | 81 | F | 40 | ss | LN | Cholecystectomy Resection of liver bed |
48 Months Alive |
LN, lymph node; ND, not described; hinv(+), liver invasion, positive; ss, subserosal; se, tumor penetrated the serosa without invasion of adjacent structures.
Squamous cell carcinoma is a rare tumor of the gallbladder, with a reported incidence of 0.5–12.7% of all malignant tumors of the gallbladder.16,17 Most form a large mass with invasive growth, which involves the neighboring organs, such as the duodenum or transverse colon, but lymph node metastases and peritoneal dissemination occur less frequently. The prognosis is extremely poor. Death occurs within 6 months after the diagnosis in almost all patients.
Adeno-endocrine cell carcinoma of the gallbladder generally has a poor prognosis. The present case is only the second case that achieved long-term survival; the longest survival was 12 years.18 The usual treatment consists of complete removal of the diseased gallbladder, with the extent of surgery ranging from laparoscopic cholecystectomy for small lesions to radical cholecystectomy and regional lymphadenectomy for advanced lesions.8,19 There is no general agreement on when, or even whether patients with adeno-endocrine cell carcinoma should receive chemotherapy. Various drugs, such as doxorubicin, 5-fluorouracil, cisplatin, and streptozocin, have been used either alone or in combination, with poor overall response rates. Biotherapy using somatostatin analogs such as octreotide or lanreotide has been assessed in the treatment of metastatic disease; it has demonstrated tumorostatic effects with symptomatic improvement.10,20
4. Conclusion
Adeno-endocrine cell carcinoma of the gallbladder is an uncommon neoplasm of the gallbladder, and the diagnosis is often made postoperatively on histopathological examination. The present case suggests that adeno-endocrine cell carcinoma with various components may be derived from a common precursor cell. This observation would require further investigation.
Conflict of interest statement
We have no financial and personal relationships with other people or organizations that could influence our work.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
T.A. and K.K. evaluated the patient and wrote the manuscript. K.K., T.G, K.S and N.H. performed the surgery. T.N was the leader of the treatment.
References
- 1.Tahara E. Endocrine tumors of the gastrointestinal tract: classification, function and biological behavior. Digestive Disease Pathology. 1988;1:121–147. [Google Scholar]
- 2.Pilichiwska M., Kimura N., Ouchi A. Primary hepatic carcinoid and neuroendocrine carcinoma: clinicopathological and immunohistochemical study of five cases. Pathology International. 1999;49:318–324. doi: 10.1046/j.1440-1827.1999.00866.x. [DOI] [PubMed] [Google Scholar]
- 3.Arrigoni M.G., Woolner L.B., Beraatz P.E. Atypical carcinoid of the lung. Journal of Thoracic and Cardiovascular Surgery. 1972;49:413–421. [PubMed] [Google Scholar]
- 4.Joel W. Karzinoid tumor der gallenblase. Zentralblatt fur Allgemeine Pathologie und Pathologische Anatomie. 1929;46:14. [Google Scholar]
- 5.Carriage M.T., Henson D.E. Liver, gallbladder, extrahepatic bile duct and pancreas. Cancer. 1995;75(Suppl 1):171–190. doi: 10.1002/1097-0142(19950101)75:1+<171::aid-cncr2820751306>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 6.Yamamoto M., Nakajo S., Miyoshi N., Nakai S., Tahara E. Endocrine cell carcinoma (carcinoid) of the gallbladder. American Journal of Surgical Pathology. 1989;13:292–302. doi: 10.1097/00000478-198904000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Wada A., Ishiguro S., Tateishi R., Ishikawa O., Matsui Y. Carcinoid tumor of the gallbladder associated with adenocarcinoma. Cancer. 1983;51:1911–1917. doi: 10.1002/1097-0142(19830515)51:10<1911::aid-cncr2820511026>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 8.Angelini C., Mussi C., Crippa S., Sartori P., Isimbaldi G., Bonardi C. Gallbladder carcinoid: a case report. Chirurgia Italiana. 2003;55:571–573. [PubMed] [Google Scholar]
- 9.Eriguchi N., Aoyagi S., Noritomi T., Imamura M., Sato S., Fujiki K., Furukawa S., Shirozu K., Hayashi I. Adeno-endocrine cell carcinoma of the gallbladder. Journal of Hepato-Biliary-Pancreatic Surgery. 2000;7:97–101. doi: 10.1007/s005340050161. [DOI] [PubMed] [Google Scholar]
- 10.Mallika T., Vinay K., Raghvendra R.M., Hari S.S. Gallbladder carcinoid masquerading as gallbladder carcinoma. Hepatobiliary and Pancreatic Diseases International. 2009;8:326–328. [PubMed] [Google Scholar]
- 11.Muto Y., Okamoto K., Uchimura M. Composite tumor (ordinary adenocarcinoma, typical carcinoid, and goblet cell adenocarcinoid) of the gallbladder: a variety of composite tumor. American Journal of Gastroenterology. 1984;79:645–649. [PubMed] [Google Scholar]
- 12.Iida Y., Tsutsumi Y. Small cell (endocrine cell) carcinoma of the gallbladder with squamous and adenocarcinomatous components. Acta Pathologica Japonica. 1992;42:119–125. doi: 10.1111/j.1440-1827.1992.tb03086.x. [DOI] [PubMed] [Google Scholar]
- 13.Maitra A., Tascilar M., Hruban R.H., Offerhaus G.J., Saavedra J.A. Small cell carcinoma of the gallbladder. American Journal of Surgical Pathology. 2001;25:596–601. doi: 10.1097/00000478-200105000-00005. [DOI] [PubMed] [Google Scholar]
- 14.Wakabayashi H., Ushiyama T., Sao K., Maeta H. Successful resection of a large rare composite tumor (endocrine cell carcinoma and squamous cell carcinoma) of the gallbladder after preoperative arterial and portal embolization. Digestive Surgery. 2003;20:457–460. [Google Scholar]
- 15.Mori M., Sato T., Yamamoto K., Seki H., Ishikawa H., Tsutsumi Y. A case of adenoendocrine cell carcinoma of the gallbladder with squamous differentiation in metastatic lymph node: a case report (in Japanese) The Japanese Journal of Gastroenterological Surgery. 2005;38:63–68. [Google Scholar]
- 16.Karasawa T., Itoh K., Komukai M., Ozawa U., Sakurai I., Shikata T. Squamous cell carcinoma of the gallbladder, report of two cases and review of literatures. Acta Pathologica Japonica. 1981;31:299–308. [PubMed] [Google Scholar]
- 17.Miyazaki K., Tsutsumi N., Kitahara K., Mori M., Sasatomi E., Tokunaga O., Hisatsugu T. Hepatopancreatoduodenectomy for squamous and adeno-squamous carcinoma of the gallbladder. Hepato-Gastroenterology. 1995;42:47–50. [PubMed] [Google Scholar]
- 18.Mizukami Y., Nagashima T., Ikuta K., Chikamatsu E., Kurachi K., Kanemoto H., Yagi T., Ohhira S., Nimura Y. Advanced endocrine cell carcinoma of the gallbladder: a patient with 12-year survival. Hepato-Gastroenterology. 1998;45:1462–1467. [PubMed] [Google Scholar]
- 19.Oku T., Ono K., Nagamachi Y., Misu K., Senmaru N., Fujitaz M. Pedunculated carcinoid tumor of the gallbladder—analysis of the relationship between location and morphology in carcinoid tumor of the gallbladder. Nippon Shokakibyo Gakkai Zasshi. 2008;105:397–403. [PubMed] [Google Scholar]
- 20.Doherty G.M. Carcinoid tumors and the carcinoid syndrome. In: Devita V.T.J., Hellman S., Rosenberg S.A., editors. Cancer principles and practice of oncology. 8th ed. Lippincott Williams & Wilkins; Philadelphia: 2008. pp. 1721–1735. [Google Scholar]