

Abstract
INTRODUCTION
Pulmonary artery dissection associated with patent ductus arteriosus is usually seen in patients with pulmonary hypertension and Eisenmenger's syndrome. This paper presents a case with pre-Eisenmenger patent ductus arteriosus complicated by pulmonary artery dissection, and explains how she was surgically treated.
PRESENTATION OF CASE
The transthoracic echocardiography of a 21-year-old woman complaining of effort dyspnea revealed patent ductus arteriosus. Contrast-enhanced thoracic computed tomography scan showed patent ductus arteriosus and dissection in the main pulmonary artery extending from the edge of the patent ductus arteriosus orifice to the pulmonary valve. The patent ductus arteriosus was divided with pledgeted prolene suture and the dissected aneurysmal portion of the pulmonary artery was resected by surgery. Dacron graft interposition was applied to the main pulmonary artery.
DISCUSSION
Because rupture causes cardiogenic shock and sudden death, diagnosis is rare in the living subject and pulmonary artery dissection is frequently detected in autopsy. A case with pulmonary artery dissection as a result of patent ductus arteriosus has been reported in the literature, but the patient died in the preoperative period. In our study, the patient was not diagnosed to have Eisenmenger's syndrome, but had pulmonary artery dissection, a complication arising from patent ductus arteriosus. The patient underwent curative surgery that included pulmonary artery dissection repair and closure of the patent ductus arteriosus.
CONCLUSION
In addition to pulmonary artery aneurysm, pulmonary artery dissection must also be considered as a complication in cases of patent ductus arteriosus with high pulmonary artery pressure diagnosed in adulthood.
Keywords: Patent ductus arteriosus, Pulmonary artery dissection
1. Introduction
Ductus arteriosus is a vessel in the fetus bypassing pulmonary circulation by connecting the pulmonary artery directly to the ascending aorta and closes at birth. And patent ductus arteriosus is a congenital anomaly caused by this vessel's failure to close. The condition is usually diagnosed in early childhood. Delayed diagnosis generally gives rise to following complications: pulmonary hypertension, Eisenmenger's syndrome, congestive heart failure, infective endarteritis, and pulmonary artery aneurysm. A rare but lethal complication is pulmonary artery dissection. Dissection occurs as a result of chronic pulmonary arterial hypertension associated with patent ductus arteriosus and is typically seen in patients with Eisenmenger's syndrome. Right-to-left blood flow through the septal defect is one of the complications of this syndrome observed in such congenital heart defects as patent ductus arteriosus. This is considered as a criterion for inoperability. Successful surgery has been reported in patients with pulmonary artery dissection associated with Eisenmenger's syndrome, which remained untreatable in some cases.1,2 This paper presents a case with pre-Eisenmenger patent ductus arteriosus complicated by pulmonary artery dissection, explaining how she was surgically treated.
2. Presentation of case
The electrocardiogram of a 21-year-old woman complaining of effort dyspnea showed sinus rhythm and signs of right ventricular hypertrophy, while chest radiography revealed widened pulmonary conus. Transthoracic echocardiography revealed patent ductus arteriosus, pulmonary hypertension (pulmonary artery pressure of 90 mmHg, systemic arterial pressure of 110/80 mmHg), aneurysmal expansion of the pulmonary artery, severe tricuspid insufficiency, and patent foramen ovale. Contrast-enhanced thoracic computed tomography scan showed patent ductus arteriosus and dissection in the main pulmonary artery extending from the edge of the patent ductus arteriosus orifice to the pulmonary valve. Heart catheterization was not attempted due to the presence of dissection.
Informed consent was obtained prior to the operation. Median sternotomy was performed under general anesthesia. Pulmonary artery was seen to be aneurysmal. Cardiopulmonary bypass was performed using bicaval venous cannulation, and the patient was cooled to 22 °C. After cross-clamping, the heart was arrested with antegrade blood cardioplegia with potassium. Pulmonary artery was opened longitudinally after the pump flow rate was reduced to 10 ml/kg/min. There was a chronic dissection extending from the patent ductus arteriosus to the pulmonary valve on the pulmonary artery. The pump rate was increased after dividing the patent ductus arteriosus with pledgeted prolene suture. The dissected aneurysmal portion of the pulmonary artery was resected. Dacron graft interposition was applied to the main pulmonary artery. Ring annuloplasty was performed on the tricuspid valve. The patent foramen ovale was closed primarily with Prolene suture. The cardiopulmonary bypass operation was completed uneventfully. The patient had no problems during her 3-day intensive care stay and was discharged on the 7th postoperative day.
3. Discussion
Patent ductus arteriosus is an acyanotic congenital heart disease resulting from the postnatal closure defect of the ductus arteriosus and sometimes continues into adulthood. However, right-to-left blood flow through the septal defect gives rise to cyanosis. This condition is known as Eisenmenger's syndrome and is a contraindication to the surgical closure of patent ductus arteriosus. Patent ductus arteriosus represents 5–10% of all congenital heart diseases, with a female-to-male ratio of 2:1. Delayed treatment may lead to certain complications including pulmonary hypertension, Eisenmenger's syndrome, congestive heart failure, and infective endarteritis. Though rare, pulmonary artery dissection may also be included in the above list of complications.
Posing a high mortality risk, pulmonary artery dissection results from congenital heart disease, pulmonary hypertension and cardiac interventions.3 Right heart endocarditis, amyloidosis, trauma and severe atherosclerosis may also result in pulmonary artery dissection.4 The most common cause is pulmonary hypertension associated with congenital heart disease. Loss of elastic fibers and degeneration in the media layer due to chronic pulmonary hypertension cause the arterial wall to weaken, and the increasing intravascular pressure and shear stress lead to the formation of intimal tears. The main pulmonary artery is involved in 80% of the cases. However, isolated cases with right or left pulmonary artery involvement can also be seen. Localized small dissections are rare. Because rupture causes cardiogenic shock and sudden death, diagnosis is rare in the living subject and pulmonary artery dissection is frequently detected in autopsy.5 Rousou et al. stated that only 8 (12.6%) out of 63 cases were diagnosed to have pulmonary artery dissection while living, and that 34 (53.9%) of the cases had congenital heart disease.3 Pulmonary artery dissection is diagnosed by echocardiography, contrast-enhanced thoracic computed tomography, and magnetic resonance imaging in the living subject. In the present study, we performed a contrast-enhanced thoracic computed tomography since our case had aneurysmal expansion of the pulmonary artery and dissection.
A case with pulmonary artery dissection as a result of patent ductus arteriosus has been reported in the literature, but the patient died in the preoperative period.1 Various cases with pulmonary artery dissection, a complication caused by Eisenmenger's syndrome, were successfully treated by surgery.2 In our study, the patient was not diagnosed to have Eisenmenger's syndrome, but had pulmonary artery dissection, a complication arising from patent ductus arteriosus. The patient underwent curative surgery that included pulmonary artery dissection repair and closure of the patent ductus arteriosus (Figs. 1–5).
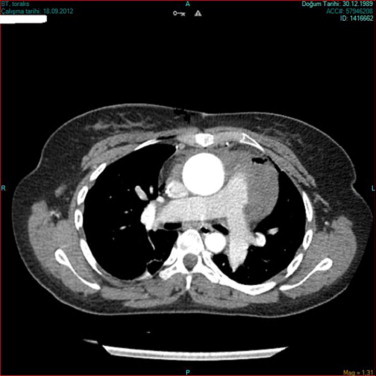
Fig. 1.
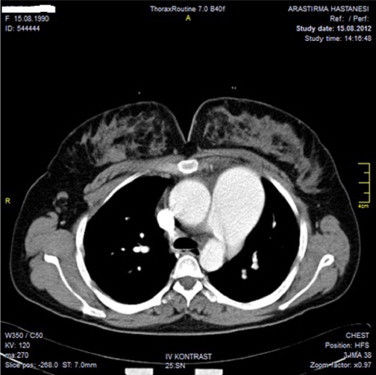
Pulmonary artery dissection beginning from the edge of the PDA.
Fig. 2.
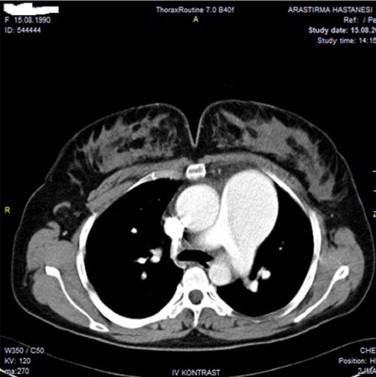
Pulmonary artery dissection.
Fig. 3.
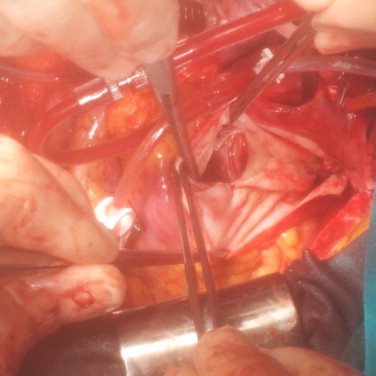
Operative view of pulmonary artery dissection.
Fig. 4.
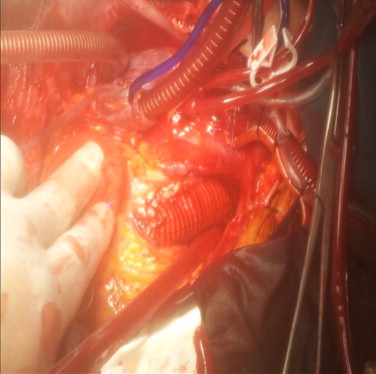
Graft interposition to pulmonary artery.
Fig. 5.
Postoperative CT view of pulmonary artery.
4. Conclusion
In addition to pulmonary artery aneurysm, pulmonary artery dissection must also be considered as a complication in cases of PDA with high pulmonary artery pressure diagnosed in adulthood.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Yasin Ay, study design, writing, data collection. Nuray Kahraman Ay, writing, data collection. Cemalettin Aydın, assistant surgeon in the operation. İbrahim Kara, data analysis. Rahmi Zeybek, review manuscript, head of the department.
References
- 1.Zhao Y., Li Z.A., Henein M.Y. PDA with Eisenmenger complicated by pulmonary artery dissection. European Journal of Echocardiography. 2010;11(September (8)):E32. doi: 10.1093/ejechocard/jeq054. [DOI] [PubMed] [Google Scholar]
- 2.Rousou A.J., Haddadin A., Badescu G., Geirsson A. Surgical repair of pulmonary artery dissection. European Journal of Cardio-Thoracic Surgery. 2010;38(December (6)):805. doi: 10.1016/j.ejcts.2010.03.064. [DOI] [PubMed] [Google Scholar]
- 3.Wunderbaldinger P., Bernhard C., Uffmann M., Kürkciyan I., Senbaklavaci O., Herold C.J. Acute pulmonary trunk dissection in a patient with primary pulmonary hypertension. Journal of Computer Assisted Tomography. 2000;24(January–February (1)):92–95. doi: 10.1097/00004728-200001000-00019. [DOI] [PubMed] [Google Scholar]
- 4.Khattar R.S., Fox D.J., Alty J.E., Arora A. Pulmonary artery dissection: an emerging cardiovascular complication in surviving patients with chronic pulmonary hypertension. Heart. 2005;91(February (2)):142–145. doi: 10.1136/hrt.2004.045799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Westaby S., Evans B.J., Ormerod O. Pulmonary-artery dissection in patients with Eisenmenger's syndrome. New England Journal of Medicine. 2007;356(May (20)):2110–2112. doi: 10.1056/NEJMc063492. [DOI] [PubMed] [Google Scholar]