

Abstract
OBJECTIVE:
To evaluate tuberculosis (TB) incidence rates and trends over a period of 20 years (1991-2010) and assess the impact of the National TB Control Program (NTP) on incidence trends.
METHODS:
This is a retrospective study of TB surveillance data reported by the Ministry of Health. We evaluated TB incidence data by nationality, age, and region of the country and assessed incidence trends over 20 years of study. Chi-squared test was used to assess trend change and its significance.
RESULTS:
There were a total of 64,345 reported TB cases over the study period. Of these 48% were Non-Saudis. TB annual incidence rate ranged between 14 and 17/100,000. For Saudis, the rate ranged between 8.6 and 12.2/100,000. Non-Saudis had 2-3 times higher incidence. Disease trend was rising over the first 10 years of the study period then it started to fall slightly. The incidence increased with age, but only people older than 45 years showed a declining trend. Regional variations were observed. Makkah and Jazan regions had the highest incidence rates. Disease trends were rising over the last 10 years in Makkah and Central regions.
CONCLUSION:
TB control seems to be facing some challenges in several regions of the Kingdom. NTP needs to evaluate and improve TB control strategies in order to reduce disease incidence to elimination levels.
Keywords: Epidemiology, incidence trend, Saudi Arabia, tuberculosis
The global burden of tuberculosis (TB) is enormous. There were an estimated 8.7 million cases of TB in 2011 and 1.4 million TB deaths.[1] Most of the cases were reported from Asia (59%), and Africa (26%). The Millennium Development Goals set a target to halt and reverse the incidence of the disease by 2015.[2] Global incidence rates have been falling, although slowly over the past few years in various regions of the world.
Saudi Arabia under-went vast economic expansion which led to improving social and health services. This was associated with an influx of large numbers of foreign workers. Most of these came from countries with a high burden of TB such as India, Pakistan, Bangladesh, Indonesia, and Yemen. This probably has adversely affected TB control in the kingdom. Saudi health authorities implemented a National TB Control Program (NTP) for over 30 years.[3] This is incorporated into the general health services. It depends mainly on finding and treating active TB patients, improving methods of reporting and laboratory services. Bacillus Calmette-Guérin (BCG) vaccination is mandatory to all children at birth, and TB treatment is offered freely to all patients in government hospitals. In the year 2000, the NTP started to implement directly observed treatment, short course (DOTS) in all regions of the Kingdom. These control strategies are expected to lower the incidence of the disease. This study aims to evaluate TB incidence trends over the past 20 years and to assess the impact of the NTP on the control of the TB.
Methods
TB is a notifiable disease in Saudi Arabia. New TB cases are reported monthly to the NTP in the Ministry of Health. Collected data are organized, tabulated and published within the annual statistical health report.[4] In this study, we reviewed TB surveillance data for the period between 1991 and 2010. The data included patient age, sex, nationality, and region. TB incidence was calculated based on population data obtained from the Department of Statistics and Information, Ministry of Economy and Planning. The data for Saudi population were studied for various provinces and regions of the country. For the sake of the study, the country was divided into five regions; the Central region included Riyadh, Qasseem and Hail provinces. The Western region included Al-Madinah and Taif provinces. The Eastern region included the Eastern province and Al-Hassa. The Northern region included Hafr Al-Baten, Tabuk, Al-Jouf, Al-Qurayyat and Northern Border provinces. The Southern region included Asir, Al-Baha, Bisha, Najran and Al-Qunfudah provinces. Two other regions were separated because they showed different incidence rates: These were Makkah and Jazan regions. Makkah region included Makkah and Jeddah provinces. TB incidence trends were analyzed for Saudis and Non-Saudis and for different age groups. Disease trends were also assessed for Saudi population in various regions of the kingdom. Data were analyzed using Epi Info (TM) statistical package (version 3.5.1). Chi-squared test was used to evaluate trend. The significance level was set at P < 0.05.
Results
There were a total of 64,345 TB cases reported to the Ministry of Health during 1991-2010. Of these, there were 46,827 (73%) pulmonary TB cases and 17,518 (27%) extra-pulmonary TB. There were 33,468 (52%) Saudi patients and 30,837 (48%) non-Saudis. The majority (62%) were males. Over 70% of the cases were reported from the Central and Makkah regions. These two regions have 52% of the population of the kingdom.
The annual incidence of TB ranged between 14 and 17/100,000 over the study period [Table 1]. Saudis had an incidence between 8.6 and 12.2/100,000 while non-Saudis had an incidence of 24.3-32.3/100,000. TB incidence showed a rising trend over the first 10 years of the study period (P < 01). The trend for Non-Saudis then started to decline (P < 0.01). Disease trend for Saudis remained flat over the last 10 years [Figure 1]. TB incidence increased with age and was highest for those older than 45 years (27.4-37/100,000). Children had an incidence of 1.8-2.8/100,000 [Table 2]. There was no significant change in TB incidence trend for children and adults younger than 45 years [Figure 2]. Those older than 45 showed a declining trend over the last 10 years (P < 01).
Table 1.
Annual TB patient numbers and incidence rate/100,000 in Saudi Arabia (1991-2010)
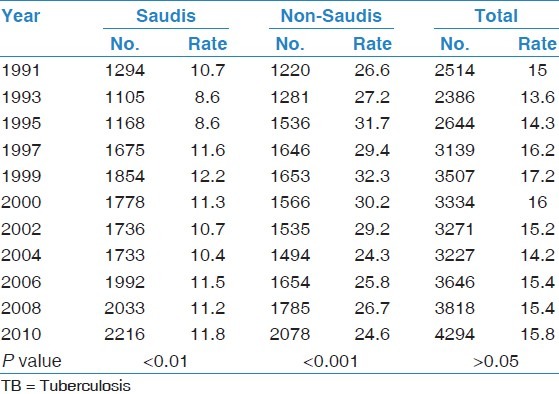
Figure 1.

Tuberculosis incidence rates and trend in Saudi Arabia (1991-2010)
Table 2.
TB patient numbers and incidence rates/100,000 by age group in Saudi Arabia (1991-2010)

Figure 2.
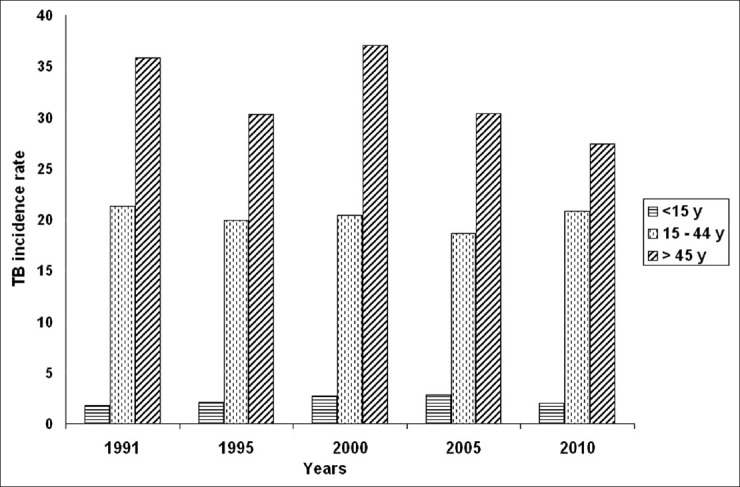
Tuberculosis incidence rates and trends by age group in Saudi Arabia (1991-2010)
TB incidence for Saudis showed a clear variation in different regions [Table 3]. Makkah and Gizan regions showed the highest incidence rate that reached up to 29.5/100,000. The trend was rising significantly in Makkah over the last 20 years (P < 01). The Central region had a significant rise in incidence climbing from 6.4 to 14.2/100,000 over the study period (P < 01). Other regions showed a much lower and stable incidence of 4-9/100,000 [Figure 3].
Table 3.
TB patient numbers and incidence rates/100,000 among Saudi population by region (1991.2010)
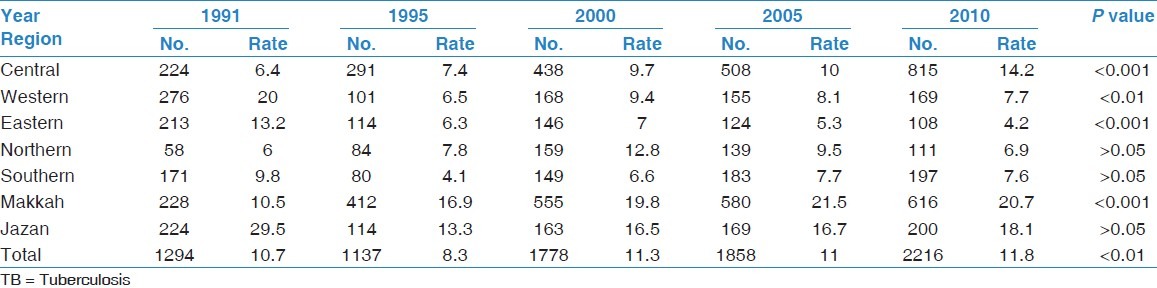
Figure 3.
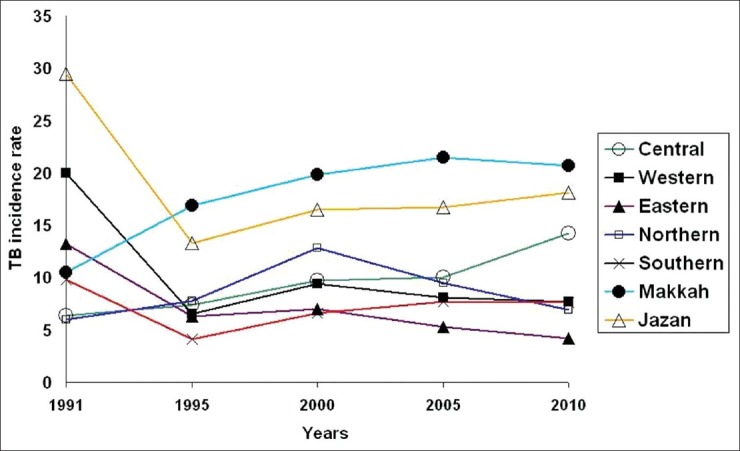
Tuberculosis incidence rates and trends for Saudi population by region (1991-2010)
Discussion
The NTP had an ambitious goal to reduce the incidence of TB to 1/100,000 by the year 2010.[3] This goal unfortunately could not be achieved. Since 1992, the incidence showed a rising trend that peaked in 1999, and then it started to fall but only slightly. Foreign population had 2-3 times higher incidence than Saudi nationals. This is similar to findings in other developed countries.[5–7] The majority of Non-Saudis came from countries with high burden of TB such as India, Pakistan, Bangladesh, Indonesia, and Yemen. Most of them are unskilled workers that tend to live in crowded housing conditions with poor nutrition and stressful work. These circumstances make them liable to have reactivation of latent TB. Foreigners coming to work in the kingdom are not screened for TB at entry, except for house workers and health professionals. TB incidence for Non-Saudis showed a falling trend over the last 10 years while the trend for Saudis remained stationary. In the year 2000, the NTP started to implement a strategy of DOTS to all regions in the Kingdom. This may partially explain the falling overall trend among non-Saudis over the last decade. For Saudis, the trend showed a significant rise between 1995 and 2010 (P < 0.01). It was not affected by the implementation of DOTS. The absence of an effect on Saudis trend is difficult to explain. As the rise in trend was mainly in the Central and Makkah regions, it may be related to the higher proportion of Non-Saudis in urban areas of these regions. Globally, TB incidence trends showed variations among countries and regions of the world. In some areas, the rates have stabilized while in others, they continue to decline slowly.[8–10] Improved control efforts and widespread implementation of DOTS did not lead to the expected fall in TB trends.[11] More efforts are required to improve early case detection and treatment.
There was an increasing TB incidence with age. Children less than 15 years of age had an incidence of 1.8-2.8/100,000 with a stable trend. Childhood TB is more reflective of new infections and transmission from adults in the community.[12] BCG vaccination is compulsory at birth in Saudi Arabia, with coverage of 97% of children.[3,4] The fact that TB trend in children did not fall over the last 20 years is an indication of inability of TB control efforts to reduce the infection rate and halt transmission of the disease.
Older population had a higher incidence of TB that ranged between 27 and 37/100,000 for those more than 45 years of age. The high incidence in adults is probably due to reactivation of latent TB.[13,14] A nationwide community survey of TB done in the early 1990s revealed a high prevalence of Tuberculin skin test positivity ranging from 45% in the 25-34 year age group to over 60% in those older than 45 years.[15] This large pool of latent TB is likely to be the source of active TB in adults and would explain the high incidence rate of the disease in the older age groups.[16]
There were clear regional differences in the incidence of the disease among Saudi nationals. Makkah region showed an incidence around 20/100,000 over the last 15 years, with a rising trend. This incidence is 2-3 times that of the western, eastern, northern and southern regions. The proportion of non-Saudis in Makkah region is over 40%. In addition, this region receives more than two million foreign visitors every year for pilgrimage (Hajj and Umra), many of them come from countries with a high burden of TB. Some of them stay for work in the region. These illegal immigrants tend to live in poor housing conditions, and have limited access to health care because of fear of deportation. It is likely that they contribute significantly to the high incidence of the disease in Makkah region. Jazan region also had an incidence of 16.5-18/100,000 over the last 10 years. This is more than 2 times the incidence of the rest of the Southern region. Jazan is a border area with Yemen, and receives many illegal immigrants from that country. Other illegal immigrants land in Jazan by sea from Sudan, Somalia, and other African countries. Like other illegal immigrants, they stay in poor housing conditions and have difficult access to health care. We speculate that these immigrants play an important role in the high incidence of TB in this region.
The Eastern, Western, Northern and Southern regions had an incidence rate of 4-9.5/100,000 among Saudi population. They showed a declining trend over the past 10 years. On the other hand, TB incidence among Saudis in the Central region increased from 6.4/100,000 in 1991 to 14.2 in 2010. This region has several large tertiary care hospitals caring for thousands of patients with debilitating and immune compromising diseases from other parts of the Kingdom. This may explain the rising disease trend in this region. Studies from low incidence countries have shown that major cities and urban areas have higher rates of TB than national levels.[17–19] In a recent study, many USA cities did not show a decreasing incidence of TB.[20] Migration to urban areas, increased population densities and larger proportion of foreign born population are the likely reasons for the higher incidence rates in these regions.
The remarkable economic and social developments and the large investments in health care services over the past 20 years are expected to have a positive impact on the incidence of TB in Saudi Arabia. Unfortunately, TB control seems to be facing challenges in several regions. The high influx of workers from high burden countries and the large volume of religious visitors together with many illegal immigrants in Makkah and Jazan regions are some of these challenges. There may also be some defects in NTP strategies that need to be evaluated and improved. One of the important handicaps in TB control is late diagnosis. Pulmonary TB patients are often diagnosed many weeks after the onset of symptoms. This diagnostic delay allows for transmission of the disease to many contacts. Emphasis on timely contact tracing and treatment of those with active or latent disease is one of the most important aspects of TB control. Clinicians caring for TB patients complain of defects in this particular area. The NTP needs to review its strategies, correct defects and improve TB control practices to make TB elimination an achievable goal.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.World Health organization. WHO Report 2012: Global Tuberculosis Control. 2012 [Google Scholar]
- 2.Dye C, Maher D, Weil D, Espinal M, Raviglsone M. Targets for global tuberculosis control. Int J Tuberc Lung Dis. 2006;10:460–2. [PubMed] [Google Scholar]
- 3.Al-Kahtani NH, Al-Jeffri MH. Manual of the National TB Control Program. Ministry of Health. 2003 [Google Scholar]
- 4.MOH; KSA. Annual statistical report 2011 (Arabic-English) [Last accessed on 2013 December 6]. Available from: http://www.moh.gov.sa/Ministry/MediaCenter/News/Documents/healthybook.pdf .
- 5.Talbot EA, Moore M, McCray E, Binkin NJ. Tuberculosis among foreign-born persons in the United States, 1993-1998. JAMA. 2000;284:2894–900. doi: 10.1001/jama.284.22.2894. [DOI] [PubMed] [Google Scholar]
- 6.Littleton J, Park J, Thornley C, Anderson A, Lawrence J. Migrants and tuberculosis: Analysing epidemiological data with ethnography. Aust N Z J Public Health. 2008;32:142–9. doi: 10.1111/j.1753-6405.2008.00191.x. [DOI] [PubMed] [Google Scholar]
- 7.Kim J, Langevin M, Wylie EL, McCarthy AE. The epidemiology of tuberculosis in Ottawa, Canada, 1995-2004. Int J Tuberc Lung Dis. 2008;12:1128–33. [PubMed] [Google Scholar]
- 8.Dye C, Lönnroth K, Jaramillo E, Williams BG, Raviglione M. Trends in tuberculosis incidence and their determinants in 134 countries. Bull World Health Organ. 2009;87:683–91. doi: 10.2471/BLT.08.058453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.China Tuberculosis Control Collaboration. The effect of tuberculosis control in China. Lancet. 2004;364:417–22. doi: 10.1016/S0140-6736(04)16764-0. [DOI] [PubMed] [Google Scholar]
- 10.Suárez PG, Watt CJ, Alarcón E, Portocarrero J, Zavala D, Canales R, et al. The dynamics of tuberculosis in response to 10 years of intensive control effort in Peru. J Infect Dis. 2001;184:473–8. doi: 10.1086/322777. [DOI] [PubMed] [Google Scholar]
- 11.Dowdy DW, Chaisson RE. The persistence of tuberculosis in the age of DOTS: Reassessing the effect of case detection. Bull World Health Organ. 2009;87:296–304. doi: 10.2471/BLT.08.054510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sandgren A, Hollo V, Huitric E, Kodmon C. Epidemiology of tuberculosis in the EU/EEA in 2010: Monitoring the progress towards tuberculosis elimination. Euro Surveill. 2012;17:4–7. [PubMed] [Google Scholar]
- 13.Korzeniewska-Kosela M, Krysl J, Müller N, Black W, Allen E, FitzGerald JM. Tuberculosis in young adults and the elderly. A prospective comparison study. Chest. 1994;106:28–32. doi: 10.1378/chest.106.1.28. [DOI] [PubMed] [Google Scholar]
- 14.Rajagopalan S. Tuberculosis and aging: A global health problem. Clin Infect Dis. 2001;33:1034–9. doi: 10.1086/322671. [DOI] [PubMed] [Google Scholar]
- 15.Al-Kassimi FA, Abdullah AK, al-Hajjaj MS, al-Orainey IO, Bamgboye EA, Chowdhury MN. Nationwide community survey of tuberculosis epidemiology in Saudi Arabia. Tuber Lung Dis. 1993;74:254–60. doi: 10.1016/0962-8479(93)90051-X. [DOI] [PubMed] [Google Scholar]
- 16.Dubrow EL. Reactivation of tuberculosis: A problem of aging. J Am Geriatr Soc. 1976;24:481–7. doi: 10.1111/j.1532-5415.1976.tb03269.x. [DOI] [PubMed] [Google Scholar]
- 17.McGowan JE, Jr, Blumberg HM. Inner-city tuberculosis in the USA. J Hosp Infect. 1995;30(Suppl):282–95. doi: 10.1016/0195-6701(95)90031-4. [DOI] [PubMed] [Google Scholar]
- 18.Hayward AC, Darton T, Van-Tam JN, Watson JM, Coker R, Schwoebel V. Epidemiology and control of tuberculosis in Western European cities. Int J Tuberc Lung Dis. 2003;7:751–7. [PubMed] [Google Scholar]
- 19.Horwitz O, Knudsen J. A follow-up study of tuberculosis incidence and general mortality in various occupational-social groups of the Danish population. Bull World Health Organ. 1961;24:793–805. [PMC free article] [PubMed] [Google Scholar]
- 20.Oren E, Winston CA, Pratt R, Robison VA, Narita M. Epidemiology of urban tuberculosis in the United States, 2000-2007. Am J Public Health. 2011;101:1256–63. doi: 10.2105/AJPH.2010.300030. [DOI] [PMC free article] [PubMed] [Google Scholar]