

Abstract
BACKGROUND:
Didactic lectures are frequently used to improve compliance with practice guidelines. This study assessed the knowledge of health-care providers (HCPs) at a tertiary-care hospital of its evidence-based thromboprophylaxis guidelines and the impact of didactic lectures on their knowledge.
METHODS:
The hospital launched a multifaceted approach to improve thromboprophylaxis practices, which included posters, a pocket-size guidelines summary and didactic lectures during the annual thromboprophylaxis awareness days. A self-administered questionnaire was distributed to HCPs before and after lectures on thromboprophylaxis guidelines (June 2010). The questionnaire, formulated and validated by two physicians, two nurses and a clinical pharmacist, covered various subjects such as risk stratification, anticoagulant dosing and the choice of anticoagulants in specific clinical situations.
RESULTS:
Seventy-two and 63 HCPs submitted the pre- and post-test, respectively (62% physicians, 28% nurses, from different clinical disciplines). The mean scores were 7.8 ± 2.1 (median = 8.0, range = 2-12, maximum possible score = 15) for the pre-test and 8.4 ± 1.8 for the post-test, P = 0.053. There was no significant difference in the pre-test scores of nurses and physicians (7.9 ± 1.7 and 8.2 ± 2.4, respectively, P = 0.67). For the 35 HCPs who completed the pre- and post-tests, their scores were 7.7 ± 1.7 and 8.8 ± 1.6, respectively, P = 0.003. Knowledge of appropriate anticoagulant administration in specific clinical situations was frequently inadequate, with approximately two-thirds of participants failing to adjust low-molecular-weight heparin doses in patients with renal failure.
CONCLUSIONS:
Education via didactic lectures resulted in a modest improvement of HCPs′ knowledge of thromboprophylaxis guidelines. This supports the need for a multifaceted approach to improve the awareness and implementation of thromboprophylaxis guidelines.
Keywords: Clinical practice guidelines, continuing medical education, health knowledge, practice guidelines, questionnaires, venous thromboembolism
Venous thromboembolism (VTE) is a major cause of morbidity and mortality in hospitalized patients, accounting for 5-10% of in-hospital fatalities.[1,2] Many studies have shown that VTE can be prevented in various surgical settings[3–5] and in medical patients[6] through appropriate prophylaxis. Despite its preventability, VTE prophylaxis remains underutilized as shown by multiple surveys.[7–10] In a prospective registry of 5,451 consecutive patients with ultrasonographically confirmed deep venous thrombosis (DVT) at 183 US institutions, only 42% of inpatients had received prophylaxis within 30 days before DVT development.[9] A cross-sectional survey that assessed the adherence to the 2004 American College of Chest Physicians (ACCP) VTE prophylaxis guidelines across 32 countries in 5 continents[10] showed considerable variation among countries, with adherence to guidelines ranging from 0.2 to 92% (mean = 59%) for surgical patients and 3 to 70% (mean = 40%) for medical patients. In Saudi Arabia, one retrospective study at a single center found that among 178 patients who developed VTE during hospitalization, only 44.1% of surgical patients and 21.7% of medical patients received VTE prophylaxis (P < 0.01) with case fatality of 3% for patients who received VTE prophylaxis and 31% for those who did not, P < 0.0001.[11]
It is obvious that practices of VTE prophylaxis guidelines are suboptimal. Lack of awareness or knowledge or lack of familiarity are potential barriers against their implementation.[12] Improving VTE prophylaxis practices has become an important strategy for hospitals to improve patient safety.[13] To that end, multiple interventions have been tried, including passive dissemination of guidelines, audit and feedback, computer-based decision aids and alerts[14] and continuing medical education.[15] Didactic lectures, as part of continuing medical education, are frequently used as educational tools to improve the healthcare providers′ (HCPs) knowledge of VTE prophylaxis guidelines, which is crucial for their appropriate implementation. However, their effectiveness is questionable. The objectives of this study were to assess the knowledge of HCPs working at a tertiary-care center of its VTE prophylaxis guidelines and evaluate the impact of didactic lectures on this knowledge.
Methods
This study consisted of a cross sectional survey of HCPs working at our institution who attended a VTE awareness day held in June 2010. The institution was a 900-bed tertiary care academic hospital, which was staffed by multinational HCPs of different training backgrounds and accredited by the Joint Commission International. In 2005, the hospital established a multidisciplinary taskforce that developed institutional VTE prophylaxis guidelines, which mostly followed the 2004 ACCP evidence-based clinical practice guidelines.[16] These guidelines were then updated in 2010 according to the 2008 recommendations.[17] In addition, the hospital launched a multifaceted program to improve VTE prophylaxis practices. The program consisted of exhibiting reminder posters in the various hospital areas, distributing a pocket-size summary of thromboprophylaxis guidelines, distributing compact discs containing related educational material and presenting didactic lectures during annual VTE awareness days.
To evaluate the hospital-based HCPs′ knowledge of the VTE prophylaxis guidelines and the effect of continuing medical education using didactic lectures on this knowledge, a self-administered questionnaire on VTE prophylaxis was distributed to those attending a VTE awareness day. The questionnaire was formulated by one physician and was tested in a pilot study by five HCPs (two physicians, two nurses and a clinical pharmacist), none of whom was part of the study population. Appropriate changes in the questions were made as a result of the pilot study. The questionnaire consisted of a section on the participant′s demographics, specialty and number of years in the clinical practice and of 15 true/false statements that covered the following thromboprophylaxis-related subjects: VTE risk stratification, VTE prophylaxis management during neuraxial analgesia, dosing of low-molecular-weight heparin in patients with chronic renal failure and the appropriate choice of VTE prophylaxis agents for specific patients. Before the start of didactic lectures at the hospital auditorium, the questionnaires were distributed to all attendees who were asked to respond before the start of the educational activity. The didactic lectures were presented in English by physicians of different specialties with PowerPoint slides projected onto a large screen. They focused on VTE risk assessment and the evidence-based VTE prophylaxis guidelines. The same questionnaire was distributed again to attendees before the closing session. The completed questionnaires were gathered at the end of introductory lecture and of the closing session. The Institutional Review Board of the hospital approved this study.
SPSS was used for statistical analysis. For continuous variables, means with standard deviations were presented. For categorical variables, frequencies with percentages were given. Each HCP′s score was calculated as the number of correctly identified answers (range 0-15). A Pearson correlation was performed between scores and number of years of clinical practice. Differences among the different groups of HCPs were assessed using the Student′s t-test. Difference in the pre- and post-scores were assessed using the paired Student′s t-test. P < 0.05 were considered to be statistically significant. The 35 HCPs who completed the pre- and post-tests had a standard deviation of their score of 2.2, allowing for the detection of a score difference of 1.1 at an alpha of 0.05 and a power of 80%.
Results
More than 200 HCPs registered for the VTE awareness day. Seventy two and 63 HCPs submitted the pre- and post-test, respectively. Of these, 62% were physicians and 28% were nurses, with both groups representing different clinical disciplines. They had an average of 16.7 ± 7.8 years of experience in health-care practice (range = 1-41) and were from different clinical and non-clinical departments (19.4% Medicine, 16.7% Emergency Medicine, 15.3% Obstetrics and Gynecology and 5.6% Surgery).
In the pre-test, the mean scores were 7.8 ± 2.1 (maximum possible score = 15, median = 8.0, quartiles 1 and 3 = 7.0 and 9.0). There was no significant difference in the scores of nurses and physicians (7.9 ± 1.7 and 8.2 ± 2.4, respectively, P = 0.67). The median scores for the different specialties were as follows: 8.0 for surgeons, 8.0 for internists with or without a specialty, 9.0 for emergency care specialists and 8.0 for obstetricians. There was also no correlation between the pre-test score and the duration of experience in health-care (r = 0.14, P = 0.28). The mean score for the post-test was 8.4 ± 1.8, which was not different than that of the pre-test (P = 0.053).
For the 35 HCPs who completed the pre- and post-tests, their scores were 7.7 ± 1.7 and 8.8 ± 1.6, respectively, P = 0.003. The median score difference was +1.0. Six HCPs scored lower on the post-test than the pre-test, five had the same score and 22 had a higher score ranging between 1 and 6 points.
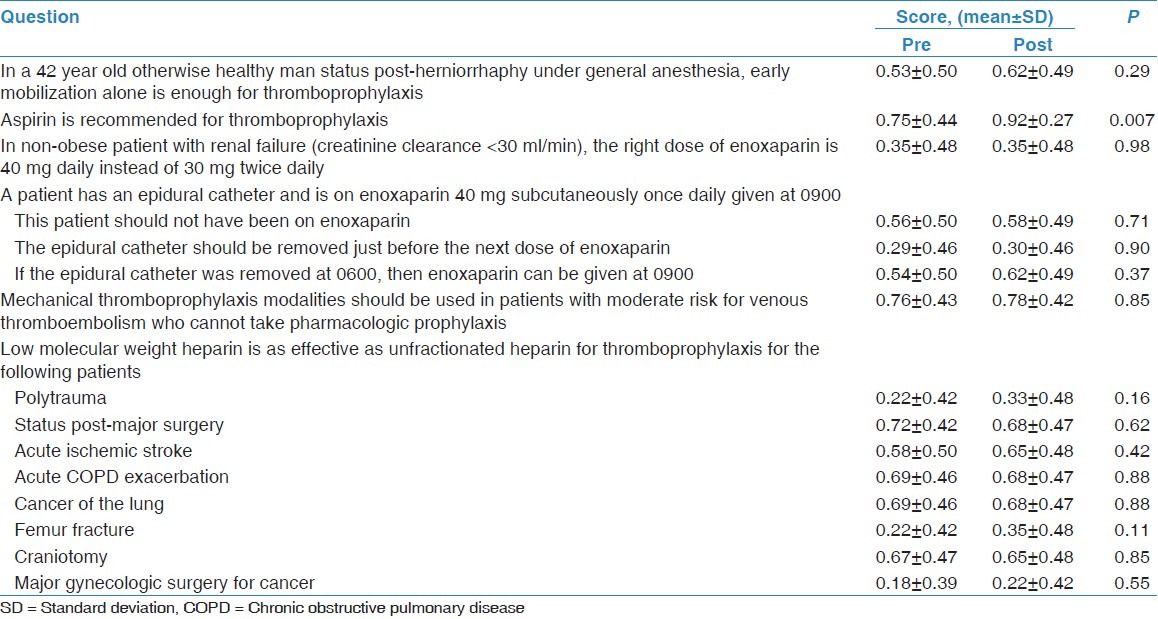
Table 1 describes the scores for the different questions. In the pre-test, only 53% of HCPs correctly stratified the VTE risk of a surgical patient admitted for herniorrhaphy (score of surgeons was 0.75 ± 0.5). Minority of the surveyed HCPs had the correct knowledge of VTE prophylaxis management during neuraxial analgesia and 25% of them thought that aspirin could be used for VTE prophylaxis. Additionally, the knowledge to adjust the dose of low-molecular-weight heparin in the setting of renal failure was unknown for the almost two-thirds of participants. There was also a significant knowledge deficit regarding the choice of the appropriate pharmacologic agent for VTE prophylaxis in specific patients [Table 1]. There was no significant difference in the post-test scores for most questions, except for the question regarding the use of aspirin for VTE prophylaxis.
Table 1.
Questionnaire items and the score of the participants before and after the educational program
Discussion
The main findings of this study were that the HCPs′ knowledge of specific VTE prophylaxis guidelines was only fair and that education via didactic lectures resulted in a modest improvement of this knowledge.
The practice of VTE prophylaxis in acute care hospitals remains suboptimal world-wide,[10] despite clear evidence of its benefits[3–6] and the presence of clinical guidelines. This deficiency is likely related to the general barriers that hinder physicians′ adherence to clinical practice guidelines. These barriers were identified by Cabana et al. and include the lack of awareness or knowledge or lack of familiarity, attitude issues such as the lack of agreement, lack of self-efficacy or lack of outcome expectancy and the inertia of previous practices and behaviors such as lack of resources, organizational constraints and guideline characteristics.[12] The results of this study reflect some of these barriers and identified the presence of a large knowledge gap regarding evidence-based VTE prophylaxis guidelines among different HCPs.
Improving the adherence to clinical guidelines is an important goal. Many tools have been used to achieve this, including the different forms of continuing medical education. However, their effectiveness in improving clinical practices in general has been controversial, with some studies showing improvement in a knowledge[18,19] and a clinical behavior[20,21] whereas others did not.[22–24] A systemic review of randomized trials or well-designed quasi-experimental studies that examined the effect of continuing education meetings (including lectures, workshops, and courses) on the clinical practice of HCPs or health-care outcomes found that the combination of workshops and didactic presentations had effects ranging from small to moderately large.[25] However, didactic presentations alone had no statistically significant effect, with the exception of one out of four outcome measures in one study.[25]
Pronovost et al. described an integrated model to translate evidence into practice.[26] This model could be applied to various settings and was based on a “four Es” approach (engage, educate, execute, and evaluate) and targeted key stakeholders from the front line staff to executives. In the “educate” step, all staff are provided with the literature supporting the proposed interventions, along with concise summaries and a checklist of the evidence.[26] Using this model, Pronovost et al. demonstrated a significant reduction in the rates of central line-associated infections in 103 intensive care units from a median of 2.7/1000 catheter days in the baseline period to 0 in the 18 months after the intervention.[26] With respect to improving VTE prophylaxis practices, Anderson et al. conducted a cluster randomized trial that evaluated the effects of continuing medical education with or without quality assurance on VTE prophylaxis strategies in 3,158 high-risk medical patients at 15 teaching and non-teaching acute care hospitals in central Massachusetts and found significant increases in the proportion of patients receiving prophylaxis in all hospitals (including control hospitals) between the two study periods (from 29% in 1986 to 52% in 1989; P < 0.001). The increase was greater in hospitals using continuing medical education compared to control hospitals (+11% vs. +28%; P < 0.001). However, there was no significant difference between hospitals using continuing medical education together with quality assurance activities and those using continuing medical education alone.[15] We found that didactic lectures have modest effects on the knowledge of health-care professionals. This result suggests that this intervention alone is unlikely to improve the practice of VTE prophylaxis in acute care hospitals.
A multifaceted approach in which multiple interventions are used to improve VTE prophylaxis practices is thought to be more effective. In addition to HCP education, these include active reminders to the providers and regular audit and feedback to the hospital staff. Scaglione et al. found that the implementation of a multi-strategy approach made up of educational presentations, pocket guidelines, the implementation of a working group to identify barriers to change and the introduction of risk-reminder cards in an Italian teaching hospital increased the appropriate use of VTE prophylaxis among surgical patients from 64% to 97%.[27] Cohn et al. demonstrated that the implementation of a multi-faceted VTE prophylaxis quality improvement program that combined regular education, dissemination of a decision support tool and regular audit-and-feedback to resident physicians in a US hospital resulted in an increase in the appropriate use of VTE prophylaxis from 43% to 68% and 85% after 12 and 18 months, respectively.[28] At an Australian hospital, Gallagher et al. evaluated a multifaceted approach, which consisted of highlighting the VTE burden. This highlighting included the extent of the failure to adhere to evidence-based guidelines and the development and application of a hospital-wide risk assessment tool that focuses on routine clinical care and enhanced feedback on VTE to clinical teams. This approach showed an increase in the VTE risk assessment in the ward setting (7.7-100%, P < 0.001), an increase in the proportion of patients receiving anticoagulant prophylaxis (48-74%, P = 0.01) and a reduction in the annual VTE rate in all the years following the intervention from 2.57/1000 cost-weighted separations in 2001 to 1.87 in 2003 (relative risk = 0.68, 95% confidence interval, 0.47-0.99, P = 0.04).[29] A systematic review of studies which were performed between 1996 and May 2003 and focused on strategies to improve VTE prophylaxis practices observed that a passive dissemination of guidelines was associated with poor adherence to both the guidelines and the provision of adequate prophylaxis, and multiple strategies were more effective than any single strategy.[30] Auditing, feedback and a system for reminding clinicians to assess patients for VTE risk (either by electronic decision-support systems or by paper-based reminders) were the most effective strategies.[30] Computer-based alerts have been shown to reduce VTE events. Kucher et al. randomized 1,255 patients at risk for a DVT into an intervention group, in which the responsible physician received a computer alert of this risk while 1,251 patients were assigned to a control group, in which no alert was issued.[31] The computer alert reduced the risk of DVT or pulmonary embolism at 90 days by 41% (hazard ratio = 0.59; 95% confidence interval, 0.43-0.81; P = 0.001).[31]
The findings of this study should be interpreted in the light of its limitations. First, the study was performed at a single center. Second, the number of participants was low relative to the size of the hospital. Third, some of the participants may not be directly involved in ordering VTE prophylaxis. Fourth, the questions may have been too specialty-specific that at least some were irrelevant to many practitioners. This study did not test the effect of educational activities on the actual compliance with the VTE prophylaxis guidelines and only examined one component of a multi-faceted intervention; therefore, the results did not reflect the effect of the whole campaign. Nonetheless, it uncovered important information and areas for improvement, which can be the focus of future interventions. Additionally, the results of this survey indirectly highlight the complexity of the VTE prophylaxis guidelines.
Conclusions
In conclusion, our study found that the HCPs′ knowledge of evidence-based VTE prophylaxis guidelines was only fair. This finding represents an important barrier for the implementation of these guidelines. We also found that continuing medical education on VTE prophylaxis using didactic lectures resulted in only a modest improvement of this knowledge. This finding supports the need for a more effective, and probably a multi-faceted, approach to improve the awareness of the complex VTE prophylaxis guidelines and their implementation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Alikhan R, Peters F, Wilmott R, Cohen AT. Fatal pulmonary embolism in hospitalised patients: A necropsy review. J Clin Pathol. 2004;57:1254–7. doi: 10.1136/jcp.2003.013581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sandler DA, Martin JF. Autopsy proven pulmonary embolism in hospital patients: Are we detecting enough deep vein thrombosis? J R Soc Med. 1989;82:203–5. doi: 10.1177/014107688908200407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Iorio A, Agnelli G. Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: A meta-analysis. Arch Intern Med. 2000;160:2327–32. doi: 10.1001/archinte.160.15.2327. [DOI] [PubMed] [Google Scholar]
- 4.Palmer AJ, Koppenhagen K, Kirchhof B, Weber U, Bergemann R. Efficacy and safety of low molecular weight heparin, unfractionated heparin and warfarin for thrombo-embolism prophylaxis in orthopaedic surgery: A meta-analysis of randomised clinical trials. Haemostasis. 1997;27:75–84. doi: 10.1159/000217437. [DOI] [PubMed] [Google Scholar]
- 5.Mismetti P, Laporte S, Darmon JY, Buchmüller A, Decousus H. Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery. Br J Surg. 2001;88:913–30. doi: 10.1046/j.0007-1323.2001.01800.x. [DOI] [PubMed] [Google Scholar]
- 6.Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1476–86. doi: 10.1001/archinte.167.14.1476. [DOI] [PubMed] [Google Scholar]
- 7.Ageno W, Squizzato A, Ambrosini F, Dentali F, Marchesi C, Mera V, et al. Thrombosis prophylaxis in medical patients: A retrospective review of clinical practice patterns. Haematologica. 2002;87:746–50. [PubMed] [Google Scholar]
- 8.Keane MG, Ingenito EP, Goldhaber SZ. Utilization of venous thromboembolism prophylaxis in the medical intensive care unit. Chest. 1994;106:13–4. doi: 10.1378/chest.106.1.13. [DOI] [PubMed] [Google Scholar]
- 9.Goldhaber SZ, Tapson VF. DVT FREE Steering Committee A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:259–62. doi: 10.1016/j.amjcard.2003.09.057. [DOI] [PubMed] [Google Scholar]
- 10.Cohen AT, Tapson VF, Bergmann JF, Goldhaber SZ, Kakkar AK, Deslandes B, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): A multinational cross-sectional study. Lancet. 2008;371:387–94. doi: 10.1016/S0140-6736(08)60202-0. [DOI] [PubMed] [Google Scholar]
- 11.Essam AE, Sharif G, Al-Hameed F. Venous thromboembolism-related mortality and morbidity in King Fahd General Hospital, Jeddah, Kingdom of Saudi Arabia. Ann Thorac Med. 2011;6:193–8. doi: 10.4103/1817-1737.84772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don′t physicians follow clinical practice guidelines. A framework for improvement? JAMA. 1999;282:1458–65. doi: 10.1001/jama.282.15.1458. [DOI] [PubMed] [Google Scholar]
- 13.Geerts W. Prevention of venous thromboembolism: A key patient safety priority. J Thromb Haemost. 2009;7(Suppl 1):1–8. doi: 10.1111/j.1538-7836.2009.03384.x. [DOI] [PubMed] [Google Scholar]
- 14.Durieux P, Nizard R, Ravaud P, Mounier N, Lepage E. A clinical decision support system for prevention of venous thromboembolism: Effect on physician behavior. JAMA. 2000;283:2816–21. doi: 10.1001/jama.283.21.2816. [DOI] [PubMed] [Google Scholar]
- 15.Anderson FA, Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Forcier A, Patwardhan NA. Changing clinical practice. Prospective study of the impact of continuing medical education and quality assurance programs on use of prophylaxis for venous thromboembolism. Arch Intern Med. 1994;154:669–77. doi: 10.1001/archinte.154.6.669. [DOI] [PubMed] [Google Scholar]
- 16.Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW, et al. Prevention of venous thromboembolism: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126:338S–400S. doi: 10.1378/chest.126.3_suppl.338S. [DOI] [PubMed] [Google Scholar]
- 17.Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest. 2008;133:381S–453S. doi: 10.1378/chest.08-0656. [DOI] [PubMed] [Google Scholar]
- 18.Fordis M, King JE, Ballantyne CM, Jones PH, Schneider KH, Spann SJ, et al. Comparison of the instructional efficacy of Internet-based CME with live interactive CME workshops: A randomized controlled trial. JAMA. 2005;294:1043–51. doi: 10.1001/jama.294.9.1043. [DOI] [PubMed] [Google Scholar]
- 19.Stewart M, Marshall JN, Østbye T, Feightner JW, Brown JB, Harris S, et al. Effectiveness of case-based on-line learning of evidence-based practice guidelines. Fam Med. 2005;37:131–8. [PubMed] [Google Scholar]
- 20.Herbert CP, Wright JM, Maclure M, Wakefield J, Dormuth C, Brett-MacLean P, et al. Better Prescribing Project: A randomized controlled trial of the impact of case-based educational modules and personal prescribing feedback on prescribing for hypertension in primary care. Fam Pract. 2004;21:575–81. doi: 10.1093/fampra/cmh515. [DOI] [PubMed] [Google Scholar]
- 21.Rahme E, Choquette D, Beaulieu M, Bessette L, Joseph L, Toubouti Y, et al. Impact of a general practitioner educational intervention on osteoarthritis treatment in an elderly population. Am J Med. 2005;118:1262–70. doi: 10.1016/j.amjmed.2005.03.026. [DOI] [PubMed] [Google Scholar]
- 22.Chung S, Mandl KD, Shannon M, Fleisher GR. Efficacy of an educational Web site for educating physicians about bioterrorism. Acad Emerg Med. 2004;11:143–8. [PubMed] [Google Scholar]
- 23.Elliott TE, Murray DM, Oken MM, Johnson KM, Braun BL, Elliott BA, et al. Improving cancer pain management in communities: Main results from a randomized controlled trial. J Pain Symptom Manage. 1997;13:191–203. doi: 10.1016/s0885-3924(96)00275-8. [DOI] [PubMed] [Google Scholar]
- 24.Zuckerman IH, Weiss SR, McNally D, Layne B, Mullins CD, Wang J. Impact of an educational intervention for secondary prevention of myocardial infarction on Medicaid drug use and cost. Am J Manag Care. 2004;10:493–500. [PubMed] [Google Scholar]
- 25.Thomson O′Brien MA, Freemantle N, Oxman AD, Wolf F, Davis DA, Herrin J. Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2001;2:CD003030. doi: 10.1002/14651858.CD003030. [DOI] [PubMed] [Google Scholar]
- 26.Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: A model for large scale knowledge translation. BMJ. 2008;337:a1714. doi: 10.1136/bmj.a1714. [DOI] [PubMed] [Google Scholar]
- 27.Scaglione L, Piobbici M, Pagano E, Ballini L, Tamponi G, Ciccone G. Implementing guidelines for venous thromboembolism prophylaxis in a large Italian teaching hospital: Lights and shadows. Haematologica. 2005;90:678–84. [PubMed] [Google Scholar]
- 28.Cohn SL, Adekile A, Mahabir V. Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention. J Hosp Med. 2006;1:331–8. doi: 10.1002/jhm.137. [DOI] [PubMed] [Google Scholar]
- 29.Gallagher M, Oliver K, Hurwitz M. Improving the use of venous thromboembolism prophylaxis in an Australian teaching hospital. Qual Saf Health Care. 2009;18:408–12. doi: 10.1136/qshc.2007.024778. [DOI] [PubMed] [Google Scholar]
- 30.Tooher R, Middleton P, Pham C, Fitridge R, Rowe S, Babidge W, et al. A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals. Ann Surg. 2005;241:397–415. doi: 10.1097/01.sla.0000154120.96169.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kucher N, Koo S, Quiroz R, Cooper JM, Paterno MD, Soukonnikov B, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969–77. doi: 10.1056/NEJMoa041533. [DOI] [PubMed] [Google Scholar]