

Abstract
The purpose of this review is to summarize the pertinent literature published in the present era regarding the antiulcerogenic property of curcumin against the pathological changes in response to ulcer effectors (Helicobacter pylori infection, chronic ingestion of non-steroidal anti-inflammatory drugs, and exogenous substances). The gastrointestinal problems caused by different etiologies was observed to be associated with the alterations of various physiologic parameters such as reactive oxygen species, nitric oxide synthase, lipid peroxidation, and secretion of excessive gastric acid. Gastrointestinal ulcer results probably due to imbalance between the aggressive and the defensive factors. In 80% of the cases, gastric ulcer is caused primarily due to the use of non-steroidal anti-inflammatory category of drug, 10% by H. pylori, and about 8-10% by the intake of very spicy and fast food. Although a number of antiulcer drugs and cytoprotectants are available, all these drugs have side effects and limitations. In the recent years a widespread search has been launched to identify new antiulcer drugs from synthetic and natural resources. An Indian dietary derivative (curcumin), a yellow pigment found in the rhizome of Curcuma longa, has been widely used for the treatment of several diseases. Epidemiologically, it was suggested that curcumin might reduce the risk of inflammatory disorders, such as cancer and ulcer. These biological effects are attributed to its anti-inflammatory and antioxidant activities. It can, therefore, be reported from the literature that curcumin PRevents gastrointestinal-induced ulcer and can be recommended as a novel drug for ulcer treatment.
Keywords: Curcumin, gastroprotective, Helicobacter pylori, non-steroidal anti-inflammatory drugs, oxidative stress
INTRODUCTION
The pathogenesis of gastrointestinal problems caused by different etiologies was observed to be associated with the alterations of various physiologic parameters such as reactive oxygen species (ROS), nitric oxide synthase (NOS), lipid peroxidation, and secretion of excessive gastric acid.[1] Interference with normal protective mechanisms can result in mucosal injury, including erosions or ulceration, which may cause significant gastrointestinal bleeding. Gastrointestinal ulcer can be a life-threatening complication in patients with gastric mucosal injury.[2] It is a deep lesion penetrating through the entire thickness of the gastrointestinal mucosa and muscularis mucosa. Ulcer disease, which can occur in the esophagus, stomach, and/or in the duodenum, is one of the main PRevalent still unresolved medical problems facing numerous patients in a wide range of age of both sexes worldwide.[3] Ulceration involves the full thickness of the gastrointestinal mucosa. It is caused by disruption of the normal balance between the corrosive effect of the gastric juice and the protective effect of the mucus on the gastric epithelial cells.[4] It results probably due to imbalance between the aggressive (acid, pepsin, bile, and Helicobacter pylori) and the defensive (gastric mucus, bicarbonate secretion, prostaglandin, nitric oxide, and innate resistance of the mucosal cells) factors.[5] Ulceration refers to a site of inflammation where an epithelial surface of the skin, gastric epithelium, colonic mucosa, and bladder epithelium has become necrotic and eroded, often associated with subepithelial acute and chronic inflammation.[6] Gastric mucosal layers play the role of a barrier by limiting the exposure of the gastric mucosal cells to numerous injurious luminal agents and irritants of both exogenous and endogenous origin. The mucosal surface epithelium is subject to attack by physical, chemical, or microbiological agents from the gastric lumen, which are involved in multiple pathologies, such as gastritis, peptic ulcer, or gastric cancer. Pretreatment with different substances could effectively PRevent the gastric mucosa from developing erosions and ulcerations.[7]
In 80% of the cases, gastric ulceris caused primarily due to the use of nonsteroidal anti-inflammatory category of drugs, 10% by H. pylori, and about 8-10% by use of very spicy and fast food.[8] Although a number of antiulcer drugs, such as H2 receptor antagonists, proton pump inhibitors, and cytoprotectants, are available, all these drugs have side effects and limitations.[9] In the recent years, a widespread search has been launched to identify new antiulcer drugs from synthetic and natural resources. An Indian dietary derivative – curcumin– has been proved an invaluable therapeutic agent that has no side effects and is cheaper to treat gastric diseases.[10] Curcumin (C21H20O6), the principal curcuminoid, a yellow pigment found in the rhizome of Curcumaloga, also known as turmeric, has been used since ancient times in China to treat various human disorders, and it is well documented for its medicinal properties in the Indian and Chinese systems of medicine.[11] The presence of both phenollic OH and CH2 groups in β-diketone moiety of this natural compound contributes significantly to its potent antioxidant properties.[12] The gastro protective potentials of curcumin might protect patients from the adverse gastric side effects of many anti-inflammatory drugs, thereby improving the quality of life for patients and decreasing the treatment costs significantly.[13] Both in vitro and in vivo studies have shown curcumin to possess a wide range of pharmacological activities including, antiprotozoa, antimicrobial, antivenom, anti-HIV, antitumor, and antiangiogenic activities.[14,15] This article, therefore, intends to document only the gastro protective potentials of curcumin that have been reported in both in vitro and in vivo studies.
Curcumin
Curcumin (curcuminoid), a yellow pigment obtained from the rhizomes of Curcumalonga (Family: Zingiberaceae), is a major component of turmeric and is commonly used as a spice and food-coloring agent.[16,17] Curcumin (diferuloylmethane), a polyphenol, is an active element of the perennial herb C. longa (commonly known as turmeric). The major curcuminoids present in turmeric are demethoxycurcumin (curcumin ll) and bisdemethoxycurcumin (curcumin lll), and the recently identified cyclocurcumin.[18] The major components of commercial curcumin are curcumin l (77%), curcumin ll (17%), and curcumin lll (3%).[3] The coloringnature of turmeric was isolated in the 19th century and was named curcumin. Curcuminoids refer to a group of phenolic compounds present in turmeric, which are chemically related to its principal ingredient curcumin.[14]
Three curcuminoids were isolated from turmeric: Curcumin, demethoxycurcumin, and bisdemethoxycurcumin [Figure 1]. All three impart the hallmark yellow pigmentation to the C. longa plant and particularly to its rhizomes. The chemical structure of curcumin was determined in the 1970s and the 1980s; recently, the potential uses of curcuminoids in medicine have been studied extensively. It was shown that oral consumption of curcumin in rats resulted in approximately 75% of it being excreted in the feces and only traces appearing in the urine, whereas intra-peritoneal administration of curcumin accounted for similar levels of fecal excretion of curcumin, with only 11% found in bile, suggesting the poor absorption of curcumin from the intestine.[19] It has also been shown to be bio-transformed to dihydrocurcumin and tetrahydrocurcumin. Subsequently, these products are converted to monoglucuronide conjugates, and reported that the main biliary metabolites of curcumin are glucuronide conjugates of tetrahydrocurcuminand hexahydrocurcumin.[20]
Figure 1.
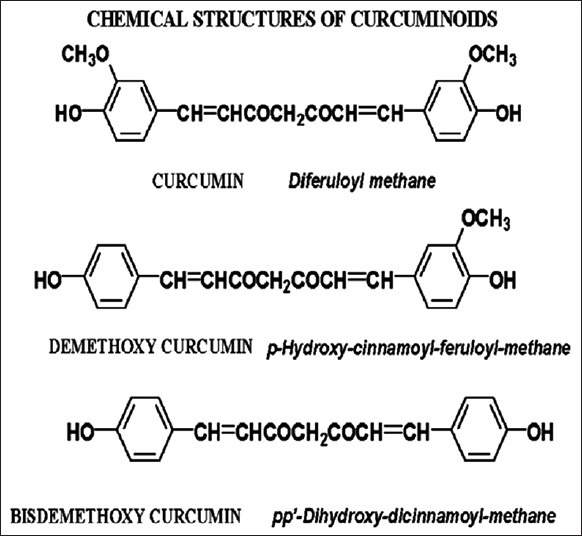
Chemical structure of curcuminoids curcumin, demethoxycurcumin, and bisdemetohxy curcumin that have shown antioxidant and anti-inflammatory properties[15]
Gastric diseases and its significance
A gastric ulcer is a hole in the gut lining of the stomach, duodenum, or esophagus. An ulcer is agastric ulcer of the stomach, a duodenal ulcer is an ulcer of the duodenum, and an esophageal ulcer is an ulcer of the esophagus. An ulcer occurs when the acidic digestive juices that are secreted by the stomach cells corrode the lining of these organs. For many years, excess acid has been believed to be the major factor responsible for ulcer disease. Accordingly, treatment emphasis was on neutralizing and inhibiting the secretion of stomach acid. Although acid is considered a primary factor in ulcer formation, the leading cause of ulcer disease currently is believed to be infection of the stomach by the bacteria called H. pylori. Another major cause of ulcers is the chronic use of anti-inflammatory medications, commonly referred to as non-steroidal anti-inflammatory drugs (NSAIDs) including aspirin. Cigarette smoking and ingestion of exogenous substances such as alcohol and fast foods are also important causes of ulcer formation and ulcer treatment failure.[8,10,21] These major effectors of gastric ulcer trigger the secretion of messenger chemicals called the ulcer chemical mediators (e.g., gastric acid, histamine, acetylcholine, Prostaglandin I2 etc.).
Helicobacter pylori
The interaction of this bacterium with the host cells (epithelial cells) had been reported to be implicated in various gastric diseases, such as gastric ulcer, adenocarcinoma, and lymphoproliferative disorders.[22] H. pylori-infected gastric mucosa showed infiltration of polymorphonuclear leukocytes, lymphocytes, monocytes, and intraepithelial severe neutrophil infiltration.[23] These changes would increase apoptosis and proliferation in the mucosal layer.[24]
NSAIDS
NSAIDs-induced ulcer is an intricate process involving inhibition of prostaglandin synthesis in the gastric tract, which causes increased gastric acid secretion, diminished bicarbonate secretion, diminished mucus secretion, diminished trophic effects on epithelial mucosa,[25] and increased microvascular permeability, nitric oxide imbalance, and free radical production. These anti-inflammatory drugs inhibit the activities of cyclooxygenase (COX) enzymes, block prostaglandin synthesis, increase gastric acid secretion, cause mucus depletion, and increase mucosal wall damage.[21]
Oxidative stress
This is caused by exogenous substances such as cigarette smoking, and consumption of alcohol and fast foods. This factor causes gastric lesion by hemorrhage, resulting from the intense production of free radicals ROS, ruptured lysosome membrane, released hydrolytic enzymes, thereby causing damage to gastric epithelial cells.[10] This damage leads to the constriction of gastric mucosa veins and arteries, causing congestion, inflammation, and tissue injury.[26]
Curcumin gastroprotective potentials
C. longa has been used in traditional remedy for a wide range of ailments, including wound healing, urinary and gastrointestinal tract infections, and liver ailments.[27] Curcumin has been defined as the most active component in C. longa and has considerable gastroprotective and antiulcerogenic effect. Its antiulcer potential activity was recently confirmed and reviewed in our laboratory.[28] The antiulcer activity of curcumin was displayed by attenuating the different ulcerative effectors including gastric acid hypersecretion, total peroxides, myeloperoxiase activity, IL-6, and apoptotic incidence, along with its inhibitory activity for pepsin.[21]
One study carried out with curcumin and dimethoxycurcumin to investigate the major functional group in curcumin reported that phenolic OH plays a major role in the activity of curcumin.[29] It is evident that the antiulcer activity of curcumin arises from its antioxidant activity. Since, the antioxidant or scavenging reactive free radicals ability of curcumin arise whether from the phenolic OH group or from the CH2 group of the b-diketone moiety.[30] Free radical-mediated peroxidation of membrane lipids and oxidative damage of cellular molecules are believed to be associated with various chronic pathological complications such as cancer, ulcer, and other inflammatory diseases.[31] Curcumin is assumed to play a vital role against these pathological conditions, and could be an antiulcer potent agent.
A study also indicated that indomethacin inactivates gastric peroxidase to induce reactive-oxygen-mediated gastric mucosa injury, and concluded that indomethacin-induced oxidative damage by ROS as shown by increased lipid peroxidation and thiol depletion was almost completely blocked by curcumin.[32] That is, curcumin protects gastric peroxidase from inactivation by indomethacin for efficient enzymatic removal of H2O2 to block gastric damage by ROS.[33]
Surprisingly, curcumin showed immense therapeutic potential against H. pylori infection, as it was highly effective in the eradication of H. pylori from infected mice as well as in restoration of H. pylori-induced gastric damage. Curcumin does this by PReventing the growth of H. pylori cagA + Strain to control H. pylori-mediated ulcer, suggesting its antiulcer potential.[34]
It has been suggested that NSAIDs could induce gastric injury through increases in inflammatory cytokines and leukocyte adhesions. Curcumin, an antioxidant herbal substance, can PRevent these adverse effects and hence might be used as a PReventive method for NSAIDs-induced gastropathy.[33] It was also reported that curcumin is more active against COX-2 and TXA2 compared to COX-1.[35] This is supported by the findings of Morimoto et al.[36] that curcumin possesses COX-2 and TXA2 inhibitory activity without affecting COX-1 activity. That is, curcumin can only block the inflammatory prostaglandin (PGI2) synthesis without affecting the synthesis of protective prostaglandin (PGE2), which is a protective mediator against gastric-induced damage. Equally, it was reported that the anti-inflammatory effect of curcumin is most likely mediated through its ability to inhibit COX-2, lipoxygenase (LOX), and inducible nitric oxide synthase (iNOS). COX-2, LOX, and iNOS are important enzymes that mediate inflammatory processes.[33,34] Recently, it has been suggested that curcumin affected arachidonic acid metabolism by blocking the phosphorylation of cytosolic phospholipase and decreasing the expression of COX-2. Furthermore, it also inhibited the catalytic activities of 5-LOX.[37] These activities may contribute to the anti-inflammatory and antiulcer actions of curcumin and its analogs.[37] This could also serve as an evidence that curcumin is a potent antiulcer agent.
A research also reported that turmeric powder has beneficial effect on the stomach. It increases mucin secretion in rabbits and may thus act as a gastroprotectant against irritants.[38] Curcumin has been shown to protect the stomach from the ulcerogenic effects of phenylbutazone in guinea pigs at 50 mg/kg doses.[39,40] It also protects from 5-hydroxytryptamine-induced ulceration at 20 mg/kg doses.[39] Recently, it was confirmed that curcumin can block indomethacin, ethanol, and stress-induced gastric ulcer and can PRevent pylorus-ligation-induced acid secretion.[40] Rafatullah et al. (1990) reported that an oral dose of 500 mg/kg of the ethanol extract of turmeric produced significant antiulcerogenic activity in rats subjected to hypothermic restraint stress, pyloric ligation indomethacin, and reserpine administration. He suggested that turmeric extract not only increased gastric wall mucus but also restored the non-protein sulfhydryl content in the glandular stomachs of rats, and finally concluded that the extract has significant antiulcer, antisecretory, and gastroprotective effects in rats.[2]
CONCLUSION
Gastrointestinal ulcer could be induced by infection of the stomach by a bacterium called H. pylori, by chronic ingestion of NSAIDs, and exogenous substances such as cigarette, alcohol, and fast foods. A dietary natural drug (curcumin) could be used to protector treat the inflammation induced by the ulcer effectors. The biological effect of curcumin to combat these induced pathological disorders is due to its anti-inflammatory and antioxidant activities. Therefore, this review confirmed curcumin as an antiulcer potent agent.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Carr ZA, Kleinerman RA, Stovall M, Weinstock RM, Griem ML, Land CE. Malignant neoplasms after radiation therapy for peptic ulcer. Radiat Res. 2002;157:668–77. doi: 10.1667/0033-7587(2002)157[0668:mnartf]2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 2.Rafatullah S, Tariq M, Al-Yahya MA, Mossa JS, Ageel AM. Evaluation of turmeric (Curcuma longa) for gastric and duodenal antiulcer activity in rats. J Ethnopharmacol. 1990;29:25–34. doi: 10.1016/0378-8741(90)90094-a. [DOI] [PubMed] [Google Scholar]
- 3.Abdulla MA, Ahmed KA, Bayaty FH, Masood Y. Gastroprotective effect of Phyllanthus niruri leaf extract against ethanol-induced gastric mucosal injury in rats. AJPP. 2010;4:226–30. [Google Scholar]
- 4.Waugh A, Grant A. 10th ed. Edinburgh, UK: Churchill Livingstone; 2006. The digestive system. Ross and Wilson anatomy and physiology in health and illness; p. 320. [Google Scholar]
- 5.Tripathi KD. 6th ed. New Delhi, India: Jaypee Brothers Medical Publishers; 2008. Drugs for peptic ulcer. Essential of medical pharmacology; p. 627. [Google Scholar]
- 6.Kumar V, Cotran R, Robbins S. 7th ed. USA: Saunders; 2002. Acute and chornic inflammation. Robbins basic pathology; p. 58. [Google Scholar]
- 7.Zayachkivska OS, Konturek SJ, Drozdowicz D, Konturek PC, Brzozowski T, Ghegotsky MR. Gastroprotective effects of flavonoids in plant extracts. J Physiol Pharmacol. 2005;56:219–31. [PubMed] [Google Scholar]
- 8.Patel R, Jawaid T, Gautam P, Dwivedi P. Herbal remedies for gastroprotective action: A review. IJPR. 2012;2:30–8. [Google Scholar]
- 9.Muchandi AA, Chandrashekhar VM. Antiulcer and gastroprotective potential of Stereospermum suaveolens in wistar rats. J Pharmacol Pharmacother. 2011;2:117–9. doi: 10.4103/0976-500X.81908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Juorkey MJ, Abdul-Aziz KK. Gastric ulcer's diseases pathogenesis, complications and strategies for PRevention. Webmed Central Gastroenterol. 2011;2:WMC001684. [Google Scholar]
- 11.Ravindran PN, Babu KN, Sivaraman K. Turmeric the genus curcuma India. CRC Press; 2009. The golden spice of life; pp. 1–13. [Google Scholar]
- 12.Mahattanadul S, Nakamura T, Panichayupakaranant P, Phdoongsombut N, Tungsinmunkong K, Bouking P. Comparative antiulcer effect of bisdemethoxycurcumin and curcumin in a gastric ulcer model system. Phytomedicine. 2009;16:342–51. doi: 10.1016/j.phymed.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 13.Xueting M, Donghui X, Sika X, Yanping Z, Shibo X. Gastroprotective and antidepressant effects of a new zinc (ll)-curmin complex rodent models of gastric ulcer and depression induced by stresses. Pharmacol Biochem Behav. 2011;99:66–74. doi: 10.1016/j.pbb.2011.04.002. [DOI] [PubMed] [Google Scholar]
- 14.Jayaprakash GK, Rao LJ, Sakariah KK. Antioxidant activities of curcumin, demethoxycurcumin and bisdemethoxycurcumin. Food chem. 2005;98:720–4. [Google Scholar]
- 15.Maheshwari RK, Singh AK, Gaddipati J, Srimal RC. Multiple biological activities of curcumin: A short review. Life Sci. 2006;78:2081–7. doi: 10.1016/j.lfs.2005.12.007. [DOI] [PubMed] [Google Scholar]
- 16.Huang MT, Lou YR, Ma W, Newmark HL, Reuhl KR, Conney AH. Inhibitory effects of dietary curcumin on forestomach, duodenal, and colon carcinogenesis in mice. Cancer Res. 1994;54:5841–7. [PubMed] [Google Scholar]
- 17.Rukkumani R, Aruna K, Varma PS, Rajasekaran KN, Menon VP. Comparative effects of curcumin and an analog of curcumin on alcohol and PUFA induced oxidative stress. J Pharm Pharm Sci. 2004;7:274–83. [PubMed] [Google Scholar]
- 18.Safwan AK. Gastroprotective Effect of tabernaemontana divaricata (Linn.) R. Br. Flower methanolic extract in wistar rats. BJPR. 2011;1:88–98. [Google Scholar]
- 19.Khan MN, Lee YS. Cyclooxygenase inhibitors: Scope of their use and development in cancer chemotherapy. Med Res Rev. 2011;31:161–201. doi: 10.1002/med.20182. [DOI] [PubMed] [Google Scholar]
- 20.Pan MH, Lin-Shiau SY, Lin JK. Comparative studies on the suppression of nitric oxide synthase by curcumin and its hydrogenated metabolites through down-regulation of Ikappa B kinase and NFkappa B activation in macrophages. Biochem Pharmacol. 2000;60:1665–76. doi: 10.1016/s0006-2952(00)00489-5. [DOI] [PubMed] [Google Scholar]
- 21.Mei X, Xu D, Wang S, Xu S. Pharmacological researches of curcumin solid dispersions on experimental gastric ulcer. Zhongguo Zhong Yao Za Zhi. 2009;34:2920–3. [PubMed] [Google Scholar]
- 22.Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345:784–9. doi: 10.1056/NEJMoa001999. [DOI] [PubMed] [Google Scholar]
- 23.Phan TT, See P, Lee ST, Chan SY. Protective effects of curcumin against oxidative damage on skin cells in vitro: Its implication for wound healing. J Trauma. 2001;51:927–31. doi: 10.1097/00005373-200111000-00017. [DOI] [PubMed] [Google Scholar]
- 24.Ohkura Y, Furihata T, Kawamata H, Tabuchi M, Kubota K, Terano A, et al. Evaluation of cell proliferation and apoptosis in Helicobacter pylori gastritis using an image analysis processor. Gastric Cancer. 2003;6:49–54. doi: 10.1007/s101200300006. [DOI] [PubMed] [Google Scholar]
- 25.Meade EA, Smith WL, DeWitt DL. Differential inhibition of prostaglandin endoperoxide synthase (cyclooxygenase) isozymes by aspirin and other non-steroidal anti-inflammatory drugs. J Biol Chem. 1993;268:6610–4. [PubMed] [Google Scholar]
- 26.Repetto MG, Llesuy SF. Antioxidant properties of natural compounds used in popular medicine for gastric ulcers. Braz J Med Biol Res. 2002;35:523–34. doi: 10.1590/s0100-879x2002000500003. [DOI] [PubMed] [Google Scholar]
- 27.Kim DC, Kim SH, Choi BH, Baek NI, Kim D, Kim MJ, et al. Curcuma longa extract protects against gastric ulcers by blocking H2 histamine receptors. Biol Pharm Bull. 2005;28:2220–4. doi: 10.1248/bpb.28.2220. [DOI] [PubMed] [Google Scholar]
- 28.Tuorkey M, Karolin K. Anti-ulcer activity of curcumin on experimental gastric ulcer in rats and its effect on oxidative stress/antioxidant, IL-6 and enzyme activities. Biomed Environ Sci. 2009;22:488–95. doi: 10.1016/S0895-3988(10)60006-2. [DOI] [PubMed] [Google Scholar]
- 29.Priyadarsini KI, Maity DK, Naik GH, Kumar MS, Unnikrishnan MK, Satav JG, et al. Role of phenolic O-H and methylene hydrogen on the free radical reactions and antioxidant activity of curcumin. Free Radic Biol Med. 2003;35:475–84. doi: 10.1016/s0891-5849(03)00325-3. [DOI] [PubMed] [Google Scholar]
- 30.Jovanovic SV, Boone CW, Steenken S, Trinoga M, Kaskey RB. How curcumin works preferentially with water soluble antioxidants. J Am Chem Soc. 2001;123:3064–8. doi: 10.1021/ja003823x. [DOI] [PubMed] [Google Scholar]
- 31.Kapoor S, Priyadarsini KI. Protection of radiation-induced protein damage by curcumin. Biophys Chem. 2001;92:119–26. doi: 10.1016/s0301-4622(01)00188-0. [DOI] [PubMed] [Google Scholar]
- 32.Chattopadhyay I, Bandyopadhyay U, Biswas K, Maity P, Banerjee RK. Indomethacin inactivates gastric peroxidase to induce reactive-oxygen-mediated gastric mucosal injury and curcumin protects it by PReventing peroxidase inactivation and scavenging reactive oxygen. Free Radic Biol Med. 2006;40:1397–408. doi: 10.1016/j.freeradbiomed.2005.12.016. [DOI] [PubMed] [Google Scholar]
- 33.Thong-Ngam D, Choochuai S, Patumraj S, Chayanupatkul M, Klaikeaw N. Curcumin PRevents indomethacin-induced gastropathy in rats. World J Gastroenterol. 2012;18:1479–84. doi: 10.3748/wjg.v18.i13.1479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.De R, Kundu P, Swarnakar S, Ramamurthy T, Chowdhury A, Nair GB, et al. Antimicrobial activity of curcumin against helicobacter pylori isolates from India and during infections in mice. Antimicrob Agents Chemother. 2009;53:1592–7. doi: 10.1128/AAC.01242-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lantz RC, Chen GJ, Solyom AM, Jolad SD, Timmermann BN. The effect of turmeric extracts on inflammatory mediator production. Phytomedicine. 2005;12:445–52. doi: 10.1016/j.phymed.2003.12.011. [DOI] [PubMed] [Google Scholar]
- 36.Morimoto T, Sunagawa Y, Kawamura T, Takaya T, Wada H, Nagasawa A, et al. The dietary compound curcumin inhibits p300 histone acetyltransferase activity and PRevents heart failure in rats. J Clin Invest. 2008;118:868–78. doi: 10.1172/JCI33160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hung CR, Wang PS. Role of histamine and acid back-diffusion in modulation of gastric microvascular permeability and hemorrhagic ulcers in Salmonella typhimurium-infected rats. Life Sci. 2004;74:2023–36. doi: 10.1016/j.lfs.2003.08.043. [DOI] [PubMed] [Google Scholar]
- 38.Lee CJ, Lee JH, Seok JH, Hur GM, Park YC, Seol IC, et al. Effects of baicalein, berberine, curcumin and hesperidin on mucin release from airway goblet cells. Planta Med. 2003;69:523–6. doi: 10.1055/s-2003-40655. [DOI] [PubMed] [Google Scholar]
- 39.Dasgupta SR, Sinha M, Sahana CC, Mukherjee BP. A study of the effect of an extract of Curcuma longaLinn. on experimental gastric ulcers in animals. Indian J Pharmacol. 1969;1:49–54. [Google Scholar]
- 40.Sinha M, Mukherjee BP, Mukherjee B, Dasgupta SR. Study on the 5-hydroxytryptamine contents in guinea pig stomach with relation to phenylbutazone induced gastric ulcers and the effects of curcumin thereon. Indian J Pharmacol. 1974;6:87–96. [Google Scholar]