

Abstract
Gingival recession is a complex phenomenon that may present numerous therapeutic challenges to the clinician. The laterally positioned flap is commonly used to cover isolated, denuded roots that have adequate donor tissue laterally and vestibular depth. Various modifications in laterally sliding flap have been proposed in order to avoid the reported undesirable results on the donor teeth. Recently, use of growth factors has been proposed in combination with surgical techniques. This article highlights the use of laterally positioned pedicle flap-revised technique as a modification of laterally sliding flap technique along with autologous suspension of growth factors, platelet rich fibrin membrane (PRF) for the management of localized Miller class-II gingival recession. After 6 months of follow-up, the clinical condition was stable with 80% root coverage and satisfactory gingival tissue healing at both donor and recipient site with no signs of inflammation. An excellent esthetical outcome was achieved and the patient was satisfied with case resolution.
Keywords: Pedicled flap, platelet rich fibrin, recession, regeneration
INTRODUCTION
Gingival recession is the apical shift of the gingiva from its normal position on the crown of the tooth to levels on the root surface beyond the cemento-enamel junction.[1] Gingival recession has been an esthetic and functional problem recognized for many years and several procedures have been proposed to preserve or enhance patient esthetics. Multiple surgical procedures have been developed to obtain predictable esthetic root coverage. The laterally positioned flap is commonly used to cover isolated, denuded roots that have adequate donor tissue laterally and vestibular depth.[2] Various modifications in laterally sliding flap have been proposed in order to avoid the reported undesirable results on the donor site. Laterally positioned pedicle flap-revised technique have been introduced by Ruben, Goldman and Jonson[3] as a modification of lateral sliding flap technique first described by Harvey (1970).[4] This flap is elevated from donor zone as full thickness in the mesial portion of the flap (near the recession) and a split thickness on the distal portion (away from the recession). The objective of full thickness (mucoperiosteal) flap design in the mesial portion of flap is to place periosteum over the exposed root to utilize its potentially dynamic reparative potential to provide more tenacious connective tissue-cementum fixation of the flap. The distal portion of the flap i.e., away from the recession reflected as split thickness flap which limits the post-operative complication of bone resorption by preserving the periosteal protection and blood supply to the septum.[5]
In the recent years for the root coverage procedures, a combination of treatment modalities involving use of surgical procedures along with growth factors has been postulated. Among the known polypeptide growth factors, platelet derived growth factor (PDGF) and transforming growth factor-β (TGF-β) has been studied most extensively. These factors, abundant in alpha granules of platelets, may control the growth of cells and, hence, the number of cells available to produce a tissue. Platelet rich plasma (PRP) and platelet concentrates made from autologous blood are used to deliver growth factors. A novel approach in dentistry is preparation and use of platelet rich fibrin (PRF), a concentrated suspension of the growth factors found in platelets. These growth factors are involved in wound healing and act as promoters of tissue regeneration. It represents a new step in the platelet gel therapeutic concept with simplified processing minus artificial biochemical modification as in PRP.[6]
The goal of the present study was to evaluate the effectiveness of use PRF along with laterally positioned flap-revised technique in the management of localized Miller class II gingival recession.
CASE REPORT
A 36-year-old male patient came to Department of Periodontia, Government Dental College and Hospital, Patiala with chief complaint of receding gums and sensitivity of lower teeth. On clinical examination a Miller class-II recession defect was present in 41 on buccal aspect along with shallow vestibule. There was clinical attachment loss of 7 mm. The distance between the cemento-enamel junction and gingival margin was 5 mm and the distance between the gingival margin and the base of the pocket was 2 mm. Base of the pocket was extending above the mucogingival junction [Figure 1].
Figure 1.

Preoperative view
Treatment plan
A two stage treatment modality was contemplated. In the first stage, to increase the vestibular depth a vestibular extension (Fenestration technique)[7] was planned. In the second stage, laterally positioned flap-revised technique[8] along with PRF membrane was speculated to cover gingival recession.
Presurgical therapy
A general assessment of patient was made through history and routine laboratory investigations. The surgical procedure was explained to the patient and the informed consent obtained. Preparation of the patient included scaling and root planing and oral hygiene instructions. Modified Stillman's brushing technique was prescribed to the patient.
Parameters assessed
Parameters were assessed with UNC-15 periodontal probe. Following parameters were assessed at baseline and 6 months after the surgical procedure.
Clinical recession depth (RD) - distance between cemento-enamel junctions to the most apical point of gingival margin.
Pocket depth (PD) - distance between the gingival margin and the bottom of the gingival sulcus.
Clinical attachment level (CAL) - measured from the cemento enamel junction to the bottom of the pocket.
Surgical procedure
Step 1: Vestibular extension procedure. After proper isolation of the surgical field, the operative sites were anesthetized using 2% xylocaine hydrochloride with adrenaline (1:200000). A horizontal incision was made using a #15 blade at the mucogingival junction retaining all of the attached gingiva. Flap was reflected sharply, dissecting muscle fibers. A rectangular periosteal strip measuring 2-3 mm width was then bluntly dissected at the level of mucogingival junction along the length of operative field, causing a periosteal fenestration [Figure 2]. Periodontal dressing (Coe pak) was placed over the wound. Post-operative instructions were given to the patient. Periodontal dressing was removed after 7 days. Patient was re-evaluated after 3 months [Figure 3].
Figure 2.

Vestibular extension (Fenestration technique)
Figure 3.

Three months after vestibular extension procedure
Step 2: After 3 months, laterally positioned pedicle flap-revised technique along with PRF was done. After proper isolation of the surgical field, the operative sites were anesthetized using 2% xylocaine hydrochloride with adrenaline (1:200000). A collar of tissue was removed around the recession by two vertical incisions, which joined at one point apical to the base of the recession [Figure 4]. Then the donor site (right canine) was prepared by giving a vertical incision extending from gingival margin to the oral mucosa up to the level of the base of central incisor with a #15 blade. After that, thorough scaling and root planning was performed. The sliding flap detached as follows: First, the one-half of the flap away from the recession was reflected as a split thickness flap by giving sharp dissection using #15 blade, and then one half of the flap close to the recession was reflected as full thickness flap by giving blunt dissection using periosteal elevator [Figures 5 and 6]. The entire flap was finally released by performing an undermining incision through the periosteum at its apical base.
Figure 4.

Collar of tissue was removed around the recession site
Figure 5.

Combined partial and full thickness flap elevated
Figure 6.

Flap showing both full and partial thickness zones
Preparation of PRF
The 5 ml of blood was drawn in 10 ml test tube without an anticoagulant and centrifuged immediately. Blood was centrifuged in single step using a Bench top centrifuge (REMY Laboratories, Goregaon, Mumbai, India) for 10 min at 3000 rpm.[9] The resultant product consisted of the following three layers: Top layer consisting of acellular platelet poor plasma, PRF clot in the middle, RBC's at the bottom [Figure 7]. The PRF membrane was obtained by squeezing out the fluids from the fibrin clot.[10] The PRF membrane was placed over the denuded roots and stabilized [Figure 8]. The flap was then slided to completely cover the membrane and secured using sling sutures [Figure 9]. Periodontal dressing (Coe-pak) was used over the surgical site.
Figure 7.
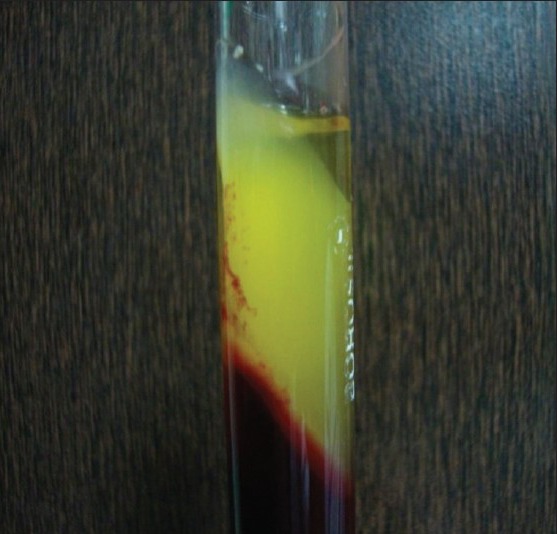
Platelet rich fibrin clot
Figure 8.

Platelet rich fibrin membrane placed
Figure 9.

Sling sutures placed
Post-Operative care
Amoxicillin 500 mg thrice a day was prescribed for 5 days. Ibuprofen 400 mg thrice daily and vitamin-B complex, 1 capsule daily were also prescribed for 5 days. Patient was recommended to follow all the normal oral post-operative hygiene instructions. Patient should rinse the oral cavity with 0.12% chlorhexidine digluconate mouth rinse for two weeks. Patient was advised to avoid pulling on their lips to observe the surgical site. Both dressings and sutures were removed 12 days after surgery [Figure 10]. Post-operative follow-up was done for 6 months [Figure 11]. In this case, there was no post-operative complication and healing was satisfactory. The patients did not have any post-operative morbidity.
Figure 10.

Post-op at 12 Days
Figure 11.

Post-op at 6 months
RESULTS
The treated site showed 5 mm gain in CAL and 4 mm reduction in recession and 1 mm reduction in probing depth at 6 months [Table 1]. Around 80% coverage was achieved 6 months after the procedure with excellent tissue contour and color. The gingival tissue of both donor and recipient site showed satisfactory healing with no signs of inflammation at final evaluation [Figure 11].
Table 1.
Clinical parameters at baseline and 6 months following treatment

DISCUSSION
Root coverage is a successful and predictable procedure in the treatment of gingival recession in periodontics. Various surgical procedures have been described to treat gingival recessions. Laterally positioned pedicle flap-revised technique have been introduced by Ruben, Goldman and Jonson[3] for management of localized gingival recession as a modification of lateral sliding flap technique first described by Harvey (1970).[4] This flap is elevated from donor zone as full thickness in the mesial portion of the flap (near the recession) and a split thickness on the distal portion (away from the recession). The objective of full thickness (mucoperiosteal) flap design in the mesial portion of flap is to place periosteum over the exposed root to utilize its potentially dynamic reparative potential to provide more tenacious connective tissue-cementum fixation of the flap. Periosteum of the mucoperiosteal flap (mesial side of flap design), recipient site periodontal ligament, periosteum, endosteum, and lamina propria surrounding the lesion can provide fibrogenic, osteogenic, cementogenic, vascular proliferative and neural trophic activity, which all play important role in healing of the periodontal surgical wound and partial thickness flap (distal side of flap design) avoid the exposure of the bone at donor site.[5] However, it is important to emphasize that all the root coverage procedures have been demonstrated to heal with a long junctional epithelium, and regeneration has been observed only in the most apical portion of the lesion.[11]
A different approach to periodontal regeneration is the use of polypeptide growth factors.
Platelet-rich plasma (PRP) is a fraction of plasma that provides a source of growth. PRP is prepared with an anticoagulant to avoid platelet activation and degranulation. Thereafter, it must undergo two centrifugation processes. Then PRP is mixed with bovine thrombin and calcium chloride at the time of application.[12] Recently, platelet-rich fibrin (PRF) has been introduced by Choukroun et al., in 2001 and has several advantages over platelet rich plasma. This second generation platelet concentrate eliminated the risk associated with the use of bovine thrombin.[13] PRP and PRF differ in their preparation protocols. PRF is used without the addition of anticoagulant and is centrifuged only once. A physiologic fibrin matrix (PRF) has very different effects than a fibrin glue enriched with cytokines (such as PRP), which has a massive uncontrollable and short-term effect. The intrinsic incorporation of cytokines within the fibrin mesh allows for their progressive release over time (7-11 days), as the network of fibrin disintegrates. The easily applied PRF membrane acts much like a fibrin bandage, serving as a matrix to accelerate the healing of wound edges. It also provides a significant postoperative protection of the surgical site.[14] PRF membrane used in this case report has the advantage of the absence of an anticoagulant; blood begins to coagulate as soon as it comes in contact with the glass surface. Therefore, for successful preparation of PRF, speedy blood collection and immediate centrifugation, before the clotting cascade is initiated, is absolutely essential. However, it is important to emphasize that this is a short term report and longitudinal clinical studies with large sample size are needed to provide solid evidence of PRF's impact on soft tissue reconstruction in periodontal therapy along with laterally positioned pedicle flap-revised technique.
CONCLUSION
Within the limits of the study, it may be concluded that laterally positioned pedicle flap-revised technique along with placement of PRF membrane in localized recession defects can be used to restore the functional properties of labial gingiva of teeth by repairing gingival defect and re-establishing the continuity and integrity of zone of keratinized gingiva.
ACKNOWLEDGMENT
The authors report no conflicts of interest related to this case report. The case report was self funded by the first author.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Loe H, Anerud A, Boysen H. The natural history of periodontal disease in man: Prevalence, severity, and extent of gingival recession. J Periodontol. 1992;63:489–95. doi: 10.1902/jop.1992.63.6.489. [DOI] [PubMed] [Google Scholar]
- 2.Carranza S. Clinical Periodontology. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, editors. 10th ed. ST. Louis, Missouri: Saunders Publication; 2006. p. 1016. [Google Scholar]
- 3.Ruben MP, Goldmon HM, Janson W. Biological considerations fundamental to successful employment of laterally repositioned pedicle flaps and free autogenous gingival grafts in periodontal therapy. In: Stahl S, editor. Periodontal Surgery. Springfield: Illinois; 1976. CH.9. [Google Scholar]
- 4.Harvey PM. Surgical reconstruction of the gingiva. Part II. Procedures. N Z Dent J. 1970;66:42–52. [PubMed] [Google Scholar]
- 5.De waal H, Kon S, Ruben MP. The laterally positioned flap. Dent Clin North Am. 1988;32:267–85. [PubMed] [Google Scholar]
- 6.Anilkumar K, Geetha A, Umasudhakar, Ramakrishnan T, Vijayalakshmi R, Pameela E. Platelet rich fibrin: A novel root coverage approach. J Indian Soc Periodontol. 2009;13:50–4. doi: 10.4103/0972-124X.51897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carranza FA, Odont Dr, editors. Clinical Periodontology. 6th ed. Philadelphia: W.B. Saunders Company; 1984. Glickman's; pp. 872–6. [Google Scholar]
- 8.Espinel MC, Caffesse RG. Lateral positioned pedicle sliding flap-revised technique in the treatment of localized gingival recessions. Int J Periodontics Restorative Dent. 1981;1:42–51. [PubMed] [Google Scholar]
- 9.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e51–5. doi: 10.1016/j.tripleo.2005.07.010. [DOI] [PubMed] [Google Scholar]
- 10.Sunitha Raja V, Muniratham Naidu E. Platelet rich fibrin: Evolution of second generation platelet concentrate. Indian J Dent Res. 2008;19:42–6. doi: 10.4103/0970-9290.38931. [DOI] [PubMed] [Google Scholar]
- 11.Grupe HE, Warren RE., JR Repair of gingival defects by a sliding flap operation. J Periodontol. 1956;27:92–5. [Google Scholar]
- 12.Aroca S, Keglevich T, Barbieri B, Gera I, Etienne D. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet–rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6-month study. J Periodontol. 2009;80:244–51. doi: 10.1902/jop.2009.080253. [DOI] [PubMed] [Google Scholar]
- 13.Toffler M, Toscano M, Holtzclaw D, Corso MD, Ehrenfest DD. Introducing Choukroun's Platelet rich fibrin (PRF) to the reconstructive surgery milieu. JIACD. 2009;1:21–32. [Google Scholar]
- 14.Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL, et al. Platelet Rich fibrin (PRF): A second generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg Oral Med Oral Pathol Oral Endod. 2006;101:299–303. doi: 10.1016/j.tripleo.2005.07.012. [DOI] [PubMed] [Google Scholar]