

Abstract
Background:
Prolonged fasting may precipitate or exacerbate gastrointestinal complaints. The aim of this study was to evaluate the relation between Ramadan fasting and acute upper gastrointestinal bleeding (AUGIB), and to assess characteristics of those occurred in the holly month.
Materials and Methods:
Retrospective analysis was conducted for all patients, who underwent endoscopy for AUGIB in Ramadan (R) and the month before Ramadan (BR). Epidemiological, clinical and etiological characteristics and outcome of patients having AUGIB were compared between the two periods from 2001 to 2010.
Results:
Two hundred and ninety-one patients had endoscopy for AUGIB during the two periods study. There was an increasing trend in the overall number of patients in Ramadan period (n = 132, 45.4% versus n = 159, 54.6%), especially with duodenal ulcer (n = 48, 37.2% versus n = 81, 62.8%). The most frequent etiology was peptic ulcer but it was more observed in group R than in group BR (46.2% versus 57.9%, P = 0.04), especially duodenal ulcer (36.4% versus 50.3%, P = 0.01); this finding persisted in multivariable modeling (adjusted odds ratio: 1.67; 95% confidence interval, 1.03-2.69, P = 0.03). In contrast, there was a decreasing trend in rate of variceal bleeding from BR period (26.5%) to R period (18.9%; P = 0.11). Regarding the outcome, there were no significant differences between the two periods of the study: Recurrent bleeding (10.6% versus 7.5%, P = 0.36) and mortality rate (5.3% versus 4.4%, P = 0.7).
Conclusion:
The most frequent etiology of AUGIB was peptic ulcer during Ramadan. However, Ramadan fasting did not influence the outcome of the patients. Prophylactic measures should be taken for people with risk factors for peptic ulcer disease.
Keywords: Acute upper gastrointestinal bleeding, duodenal ulcer, endoscopy, fasting, peptic ulcer, Ramadan, variceal bleeding
INTRODUCTION
Ramadan is the ninth lunar month of Islamic calendar during which adult Muslims fast from sunrise to sunset. Those, whom fasting or any other illness may aggravate their conditions, are exempted. Previous studies have shown that the conditions of feeding imposed by Ramadan are associated with an increase in gastric acidity and pepsin activity mainly in diurnal phase.[1,2,3,4] However, acid is a risk factor that can cause bleeding or rebleeding from peptic ulcer.[5,6,7,8] This means that modifications in gastric acid secretion are likely to increase the risk of upper gastrointestinal bleeding during Ramadan. To our knowledge, there are two published studies in the English language that have evaluated characteristics of AUGIB occurring during Ramadan fasting.[9,10] The two studies have suggested that fasting Ramadan increases the risk of bleeding from the upper gastrointestinal tract. But, there is still a lack of enough evidence, and more studies are necessary to evaluate the effect of Ramadan fasting on AUGIB.
The aim of this study was to evaluate the relation between Ramadan fasting and acute upper gastrointestinal bleeding (AUGIB), especially those related to peptic ulcer.
MATERIALS AND METHODS
We performed a retrospective analysis of a retrospective (2001-2004) and prospective (2005-2010) study on upper gastrointestinal bleeding, including all adult patients over the age of 16 years who presented with hematemesis and/or melena and/or acute anemia, attached to a lesion of the upper gastrointestinal tract, and who underwent endoscopy. The cause of the AUGIB has been attributed to a lesion in the presence of active bleeding, stigmata of recent bleeding, or the absence of other causes of bleeding. If more than one lesion were present, both were considered as causative. Rebleeding was defined as a new bleeding episode during the first 5 days of hospitalization after the initial bleeding has stopped. Mortality rate was defined on the basis of death occurring during hospitalization.
Time periods corresponding to the month of Ramadan in the Gregorian calendar have been established. Since the year in the Islamic calendar is lunar and is approximately 11-12 days shorter than the solar year, therefore the month of Ramadan coincides with different times of the year. To reduce the effects from seasonal changes to a minimum, we have evaluated data from Ramadan period (R) and compared them with the month before Ramadan (BR) by going back the duration of Ramadan (29-30 days) in each (R) and (BR) of the years of the study.
Epidemiological data of patients, clinical information, results of endoscopy, treatment and outcome of patients during their hospitalization were analyzed by the software Epi Info 3.5.1 ™(Clifton Rd. Atlanta, USA). The χ2 test was used to compare categorical parameters where appropriate. The ANOVA was used to compare the differences in the continuous parameters. Level of significance was considered when P < 0.05.
RESULTS
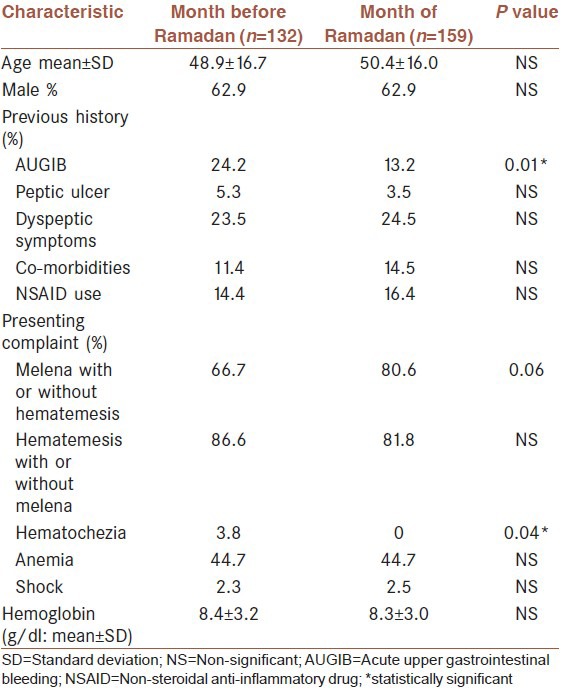
The study included 10 months of Ramadan period (from November 2001 to September 2010) and ten months of before Ramadan period (form October 2001 to August 2010). During the two study periods, 291 patients had endoscopy for AUGIB. There was an increasing trend in the overall number of patients in Ramadan period 132 (45.4%) versus 159 (54.6%). Demographic and clinical characteristics of the patients are shown in Table 1. The mean age was 49.7 ± 16.3 years and median age was 49 years (range, 16-90 years). Most patients were men (62.9%). There were no age or gender differences between the two groups (P = 0.4 and P = 0.9 respectively). There was no difference in NSAID use neither (16.4% versus 14.4%, P = 0.6). Patients in BR group had more previous history of upper gastrointestinal bleeding compared to R group (24.2% versus 13.2%, P = 0.01). In multivariate analysis, previous history of AUGIB was associated to BR group (P = 0.03) and variceal bleeding (P = 0.0007). Both groups, BR and R, were comparable regarding previous history of peptic ulcer, medication use and underlying diseases [Table 1]. Clinical presentation was hematemesis only in 40.9% cases versus 29.6% (P = 0.04) and melena only in 10.6% versus 16.4% (P = 0.15) respectively. Anemia was noted in 132 patients (44.7% in each group, P = 0.9) and shock in 7 patients (2.3% versus 2.5%, P = 0.6) without any statistically significant difference between the two groups [Table 1].
Table 1.
Demographic and clinical characteristics of patients according to the month of admission
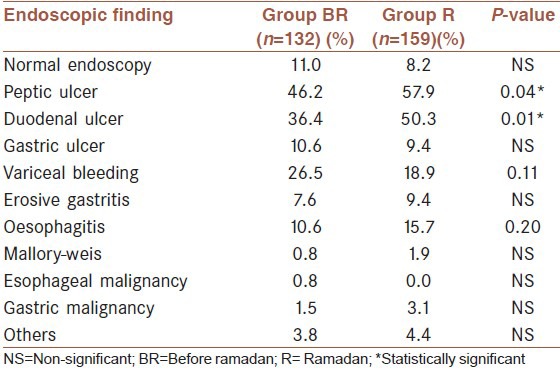
Median time to endoscopy (from the first episode of bleeding) was 22 h in group BR versus 24 h in group R (P = 0.9). The most frequent etiology was peptic ulcer (52.6%) in both groups but it was more observed in group R (n = 92, 57.9%) than in group BR (n = 61, 46.2%; P = 0.04), especially duodenal ulcer (36.4% versus 50.3%, P = 0.01); this finding persisted in multivariable analysis (adjusted odds ratio: 1.67; 95% confidence interval, 1.03-2.69, P = 0.03). In contrast, there was no significant decreasing trend in rate of variceal bleeding in Ramadan (26.5% versus 18.9%, P = 0.11). Other Endoscopic findings are resumed in Table 2.
Table 2.
Upper gastrointestinal bleeding diagnosis and frequencies
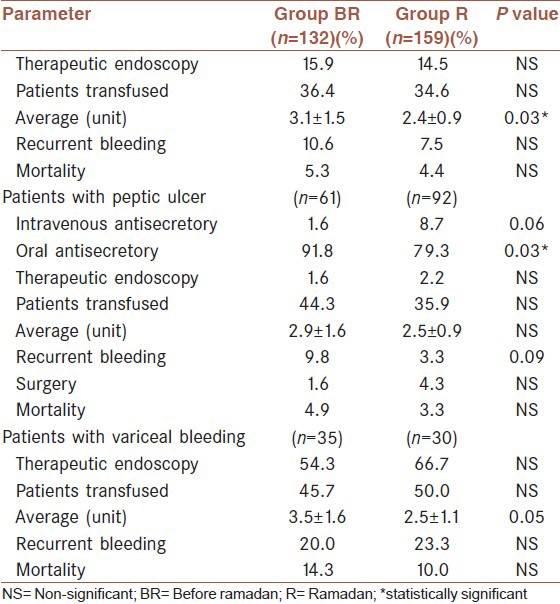
Regarding the outcome of AUGIB in both groups, there were no significant differences between them in rebleeding (P = 0.49), transfusion requirement (P = 0.75), need to therapeutic endoscopy (P = 0.73) or to surgery (P = 0.48), and mortality rate (P = 0.72) [Table 3], except for the blood-unit infused average which was higher in group BR (average 3.1 units versus 2.4 units, P = 0.03), especially for patients who had variceal bleeding (average 3.5 units versus 2.5 units, P = 0.05). However, in patients with peptic ulcer, rebleeding rate was three times more in group BR than in group R, but this difference was not statistically significant (P = 0.09). In multivariate analysis, an age ≥65 years (P = 0.01) and recurrent bleeding (P < 0.0001) were the only factors significantly associated to mortality rate of AUGIB.
Table 3.
Treatment and outcome of patients within the two groups
DISCUSSION
Morocco is a Muslim country; people fast from dawn to sunset during the month of Ramadan. The duration of fasting varies from 12 to 18 h/day depending on geographic location and the time of the year.[9,11] In our study, period covering 2001-2010, it varied between 12 h and 15 h. As already mentioned, previous reports had shown that the time distribution of food intake in Ramadan has a metabolic effect, especially a daily increasing in gastric acidity and peptic activity.[1,3,4] Furthermore, Ramadan fasting led to a decrease in the platelet responses of different aggregating agents in vitro. It also led to an increase in bleeding and coagulation time.[8] There were more patients admitted for AUGIB in the holly month, especially more duodenal ulcer bleeding. A preliminary study conducted in Kashmir, had suggested that Ramadan fasting may prove hazardous in patients with peptic ulcer disease in general and with active chronic ulcers in particular.[12] A Turkish study had shown that partial hunger during Ramadan increased the risk of duodenal ulcer complications including bleeding and perforation.[13] More recent studies followed that Ramadan fasting can increase AUGIB, especially due to duodenal ulcer.[9,10] To prevent peptic ulcer complication, patients with dyspepsia should be evaluated for peptic ulcer disease (PUD), tested for helicobacter pylori (H. pylori) infection and if diagnosed should be treated before Ramadan fasting.[14,15] In addition, higher risk patients with dyspepsia and/or a history of PUD in whom active H. pylori infection has been excluded should be considered for prophylactic acid suppression therapy before embarking on fasting in Ramadan.[15,16] For patients having an active duodenal ulcer, they could also fast without running any risk if they took a prophylactic regimen based on a proton pump inhibitor before and during Ramadan fasting.[17,18] Furthermore, some studies have suggested that the negative effect of the Ramadan fasting on duodenal ulcer may persist even in the period after Ramadan fasting.[1,13] Studies evaluating this probable dose effect of fasting on bleeding from a duodenal ulcer are still needed.
In our study, there was no statistically difference of age between the two groups, even in sub-groups who had duodenal ulcer. This was in contrast with the finding of Emami et al.'s study,[10] as they objectified that patients in fasting group were younger than non-fasting group. In this study, authors compared fasting with non fasting patients during a given period (from the 10th day of Ramadan to one month after), when we compared two periods in our study. The authors explanation for the age difference, was that old patients do not fast because of other concomitant diseases and disabilities that they have and because that duodenal ulcer was more common in fasting group and it occurred in younger patients.[10] However, no age difference was reported in the Turkish work[9] which compared between patients included during two periods: Ramadan month and a non-Ramadan month (two months later).
Moreover, sex ratio was similar between the two periods. In contrast with other studies: Emami et al.,[10] found a no significant increasing of the female rate, from 25% in non-fasting group to 35.5% in fasting group. And in the study of Dönderici et al.,[13] which compared between patients hospitalized for peptic ulcer complication in Ramadan month and before Ramadan month, authors concluded that female patients had a tendency to develop more bleeding and perforations during Ramadan than male patients. And also for a Turkish study, which compared patients operated for perforated duodenal ulcer in Ramadans within a 5-year period with those operated in the remaining periods (other months of the study period), men were predominant but less in Ramadan (90%) than non-Ramadan months (98.6%, P = 0.002).[14] Thus, these studies suggested that female rate tended to increase among patients developing bleeding or ulcer perforation during Ramadan, even though men remain predominant.[10,13,14] The present study had shown no differences of previous use of NSAID, history of peptic ulcer or co-morbidities between the two groups. But, there was less previous history of AUGIB in R group, that may be explained by the fact that patients and physicians paid more attention to contraindication of fasting with the presence of an acute event in the past, and because previous history of AUGIB was more frequent in patients with variceal bleeding than patients with non-variceal bleeding including peptic ulcer bleeding.
Apart from duodenal ulcer, there were no statistically significant differences of endoscopic finding, but a trend to have less variceal bleeding during the month of Ramadan. This finding joined those of other studies[9,10] and could be explained by the increase in frequency of AUGIB because of peptic ulcer. Besides, several studies had shown that regular food intake significantly increases azygos blood flow in cirrhotic patients compared with fasting conditions.[19,20,21] A recent study, which evaluate the effect of Ramadan fasting on Muslim patients with chronic liver diseases, found that bleeding due to esophageal varices was significantly higher in a non-fasting group (9.1%) compared to (1%) in a fasting group (P = 0.004).[22] It seems, therefore, that fasting can decrease episodes of AUGIB due to esophageal varices.[10,22]
Furthermore, we did not find significant differences between the two groups regarding the patients outcome, which suggests that Ramadan fasting may not influence the prognosis of AUGIB.[9,10,15] We should note that patients who died or had surgery before endoscopy were not included, which was a limitation for our study.
This study demonstrated that the most frequent etiology of AUGIB was peptic ulcer during Ramadan. However, Ramadan fasting did not influence the outcome of the patients. Prophylactic measures should be taken for people with risk factors for peptic ulcer disease.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Iraki L, Abkari A, Vallot T, Amrani N, Khlifa RH, Jellouli K, et al. Effect of Ramadan fasting on intragastric pH recorded during 24 hours in healthy subjects. Gastroenterol Clin Biol. 1997;21:813–9. [PubMed] [Google Scholar]
- 2.Hakkou F, Tazi A, Iraqui L, Celice-Pingaud C, Vatier J. The observance of Ramadan and its repercussion on gastric secretion. Gastroenterol Clin Biol. 1994;18:190–4. [PubMed] [Google Scholar]
- 3.Nomani M, Khan A, Shahda M, Nomani A, Sattar S. Predicting serum gastrin levels among men during Ramadan fasting. East Mediterr Health J. 2005;11:119–25. [PubMed] [Google Scholar]
- 4.Iraki L, Bogdan A, Hakkou F, Amrani N, Abkari A, Touitou Y. Ramadan diet restrictions modify the circadian time structure in humans. A study on plasma gastrin, insulin, glucose, and calcium and on gastric pH. J Clin Endocrinol Metab. 1997;82:1261–73. doi: 10.1210/jcem.82.4.3860. [DOI] [PubMed] [Google Scholar]
- 5.Li Y, Sha W, Nie Y, Wu H, She Q, Dai S, et al. Effect of intragastric pH on control of peptic ulcer bleeding. J Gastroenterol Hepatol. 2000;15:148–54. doi: 10.1046/j.1440-1746.2000.02055.x. [DOI] [PubMed] [Google Scholar]
- 6.Low J, Dodds AJ, Biggs JC. Fibrinolytic activity of gastroduodenal secretions-a possible role in upper gastrointestinal haemorrhage. Thromb Res. 1980;17:819–30. doi: 10.1016/0049-3848(80)90247-9. [DOI] [PubMed] [Google Scholar]
- 7.Patchett SE, Enright H, Afdhal N, O’Connell W, O’Donoghue DP. Clot lysis by gastric juice: An in vitro study. Gut. 1989;30:1704–7. doi: 10.1136/gut.30.12.1704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aybak M, Türkoğlu A, Şermet A, Denli O. Effect of Ramadan fasting on platelet aggregation in healthy male subjects. Eur J Appl Physiol Occup Physiol. 1996;73:552–6. doi: 10.1007/BF00357678. [DOI] [PubMed] [Google Scholar]
- 9.Ozkan S, Durukan P, Akdur O, Vardar A, Torun E, Ikizceli I. Does Ramadan fasting increase acute upper gastrointestinal haemorrhage? J Int Med Res. 2009;37:1988–93. doi: 10.1177/147323000903700637. [DOI] [PubMed] [Google Scholar]
- 10.Emami M, Rahimi H. Effects of Ramadan fasting on acute upper gastrointestinal bleeding due to peptic ulcer. J Res Med Sci. 2006;11:170–5. [Google Scholar]
- 11.Azizi F. Islamic Fasting and Health. Ann Nutr Metab. 2010;56:273–82. doi: 10.1159/000295848. [DOI] [PubMed] [Google Scholar]
- 12.Malik G, Mubarik M, Jeelani G, Tajamul H, Kadla S, Lone B, et al. Endoscopic evaluation of peptic ulcer disease during Ramadan fasting: A preliminary study. Diagn Ther Endosc. 1996;2:219–21. doi: 10.1155/DTE.2.219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dönderici O, Temizhan A, Küçükbas T, Eskioglu E. Effect of Ramadan on peptic ulcer complications. Scand J Gastroenterol. 1994;29:603–6. doi: 10.3109/00365529409092479. [DOI] [PubMed] [Google Scholar]
- 14.Kucuk H, Censur Z, Kurt N, Ozkan Z, Kement M, Kaptanoglu L, et al. The effect of Ramadan fasting on duodenal ulcer perforation: A retrospective analysis. Indian J Surg. 2005;67:195–8. [Google Scholar]
- 15.Torab FC, Amer M, Abu-Zidan FM, Branicki FJ. Perforated peptic ulcer: Different ethnic, climatic and fasting risk factors for morbidity in Al-ain medical district, United Arab Emirates. Asian J Surg. 2009;32:95–101. doi: 10.1016/S1015-9584(09)60018-X. [DOI] [PubMed] [Google Scholar]
- 16.Bdioui F, Melki W, Ben Mansour W, Loghmari H, Hellara O, Ben Chaabane N, et al. Duodenal ulcer disease and Ramadan. Presse Med. 2012;41:807–12. doi: 10.1016/j.lpm.2012.05.007. [DOI] [PubMed] [Google Scholar]
- 17.Hosseini-Asl K, Rafieian-Kopaei M. Can patients with active duodenal ulcer fast Ramadan? Am J Gastroenterol. 2002;97:2471–2. doi: 10.1111/j.1572-0241.2002.06011.x. [DOI] [PubMed] [Google Scholar]
- 18.Mehdi A, Ajmi S. Effect of the observance of diurnal fast of Ramadan on duodenal ulcer healing with lansoprazole. Results of a prospective controlled study. Gastroenterol Clin Biol. 1997;21:820–2. [PubMed] [Google Scholar]
- 19.Sugano S, Yamamoto K, Takamura N, Momiyama K, Watanabe M, Ishii K. Azygos venous blood flow while fasting, postprandially, and after endoscopic variceal ligation, measured by magnetic resonance imaging. J Gastroenterol. 1999;34:310–4. doi: 10.1007/s005350050266. [DOI] [PubMed] [Google Scholar]
- 20.Betal D, Hughes ML, Whitehouse GH, Roberts N. Postprandial decrease in splenic volume demonstrated by magnetic resonance imaging and stereology. Clin Anat. 2000;13:404–9. doi: 10.1002/1098-2353(2000)13:6<404::AID-CA2>3.0.CO;2-S. [DOI] [PubMed] [Google Scholar]
- 21.Tochio H, Kudo M, Nishiuma S, Okabe Y. Intrahepatic spontaneous retrograde portal flow in patients with cirrhosis of the liver: Reversal by food intake. Am J Roentgenol. 2001;177:1109–12. doi: 10.2214/ajr.177.5.1771109. [DOI] [PubMed] [Google Scholar]
- 22.Elnadry MH, Nigm IA, Abdel Aziz IM, Elshafee AM, Elazhary SS, Abdel Hafeez MA, et al. Effect of Ramadan fasting on Muslim patients with chronic liver diseases. J Egypt Soc Parasitol. 2011;41:337–46. [PubMed] [Google Scholar]