

Abstract
Background:
Although visual impairment of drivers is a very important risk factor for car accident, a few published papers have explored this issue in Iran. This study aims to evaluate the visual fitness of public vehicle drivers in Kerman province, southeast of Iran.
Methods:
A total of 4,003 public vehicle drivers were examined by one ophthalmologist for visual fitness in Kerman province between January 2009 and June 2010. Data are presented as Mean±SD or percentage, and with 95% confidence intervals (CIs). Pearson Chi-square and McNemmar tests along with crude odds ratio (OR) were used to compare vision deficit between groups.
Results:
Almost 361 drivers (9.0%; 95% CI: 8.1-9.9) had insufficient vision to drive public vehicles before the refractive errors (RE) correction and this number, was reduced to 68 drivers (1.7%; 95% CI: 1.3-2.1) after the correction. A number of them including 200 drivers (5.0%; 95% CI: 4.3-5.7) had insufficient vision to drive personal vehicles before the correction and this was reduced to 30 thereafter (0.8%; 95% CI: 0.5-1.0). We also found out that the vision status got worse with aging, and RE was the most prevalent cause of sight defects.
Conclusion:
It seems that visual fitness of public vehicle drivers is a point of real concerns which might somewhat explain the high rate of car accidents in Iran.
Keywords: Kerman, public vehicle driver, road safety, vision
INTRODUCTION
The number of drivers and vehicles crossing our roads increases every year. Land transportation systems have become an essential part of modern life. Speedy communications and the people and cargo transport have brought about a drastic change in modern economic and social relations.[1,2,3]
Road traffic injuries are a huge problem for public health and development, taking almost 1.2 million lives a year and crippling and injuring about 20 to 50 million more. World health organization (WHO) data show 25% of all deaths resulting from injuries are caused by road traffic injuries and without apt action, these injuries will rise significantly by the year 2020, specially in rapidly-motorizing countries. Low- and middle-income countries not only bear about 90% of the burden, they have also got the greatest casualty rates.[2,3] Comparing deaths from road traffic accidents in Iran with that of the world population, low- and middle-income countries, and the Eastern Mediterranean Region, the magnitude of the problem becomes more evident.[4] Over 30,000 people die annually in Iran from road traffic crashes, amounting to a death rate of 44 per 100,000.[5]
A road traffic crash results from a combination of factors related to the components of the system comprising roads, the environment, vehicles and road users, and the way they interact. Driving a car requires cognitive, psychomotor, and psychological aptitudes that should be assessed when the driving license is being issued. Vision is one human sense that is absolutely essential for safe driving and up to 90% of information received is visual[6,7] and it is well known that visually impaired drivers had significantly more total crashes and convictions than the non-impaired drivers.[8] To see and to be seen is a fundamental requirement for the safety of all road users and insufficient visibility appears to be a major cause of collisions.[2,3,9] Public vehicle drivers have very high levels of driving exposure compared to non-commercial drivers of personal vehicles. Since they are on the road almost continuously during their workday, logging in more miles per day than many drivers of personal vehicles cover in a week. No need to say that, public vehicle drivers need a better vision than others as the risk of having an accident increases with distance driven.[7]
It is argued that, compared with the scale of the problem in developing countries, there has been relatively little study on road traffic accidents and their consequences, and it could be regarded as ‘the neglected epidemic’.[10] We conducted this study to estimate the scale of the problem through testing the vision of the drivers on the road. To the best of our knowledge, this is the first roadside survey of its kind conducted in Iran. Kerman province is located on a high margin of Kavir-e Lut (Lut Desert) in the south-east of Iran. It is on the Tehran, Bandar Abbas and Zahedan route which connects the southern part of the country to its northern. Therefore, the level of traffic on Kerman roads is very noticeable.
METHODS
In this action research, we evaluated visual fitness among 4,003 public vehicle drivers (in commodity and passenger transportation) from January 2009 to June 2010. The drivers were selected sequentially by the transportation organization from a total of around 8,000 public vehicle drivers, in Kerman province and referred for examination. The drivers were examined by one ophthalmologist only and inclusion criteria were driving public vehicles.
Visual acuity (VA) was measured using Snellen chart (with present glasses, if they had any); VA ≥8/10 was assumed as normal. Those drivers who had an acceptable visual fitness, according to traffic rules of Iran, either with or without a pair of glasses were diagnosed healthy. However, those who had visual difficulties were prescribed glasses or new glasses were fitted. Best corrected VA was measured.
Examination of lids, ocular movements and pupils, slit lamp examination, applanation tonometry and fundoscopy was done. For suspected cases, automated visual field testing was carried out by confrontation method.
Statistical analysis
Data are presented as Mean± SD or percentages and corresponding 95% confidence intervals (CIs). We calculated visual impairment prevalence in each stage. The Pearson chi-square test was used to calculate the differences between proportions and McNemmar test to compare proportions before and after correction. We calculated crude odds ratios (ORs) and corresponding 95% CIs to compare vision deficit in middle-aged and elderly drivers compared with young drivers. The data was analyzed using Stata 10 software.
RESULTS
Study participants consisted of 4,003 male public vehicle drivers with mean age of 40.94±10.24 (20-78) years.
Before examination, 492 already (12.3%; 95% CI: 11.3-13.3) had glasses; 21.1% of which (104 drivers) needed their glasses to be changed. After examination, 683 (17.1%; 95% 15.9-18.2) drivers were diagnosed to need glasses for driving public vehicle, according to the traffic rules and regulation of Iran.
Overall, 1,061 (13.3%) eyes of 729 drivers (18.2%; 95% CI: 17.0-19.4) had a vision less than 8/10 and 238 (3.0%) eyes of 164 drivers (4.1%; 95% CI: 3.5-4.7) had a vision less than 5/10. Statistical analysis showed no significant difference of vision impairment between left and right eyes (P>0.05). In 13 drivers (0.3%; 95% CI: 0.15-0.5), the vision was less than 1/10.
Analyzing the association between vision and age revealed that the vision got worse with aging, and the worst condition was in drivers older than 54 years of age compared with <25 year group [odds ratio (OR)=14.37; 95% CI: 6.14-40.90; P value <0.0001] [Table 1].
Table 1.
Age distribution and visual defects association in public health drivers in Kerman province, Iran [2009-2010]

According to results of before and after RE correction, the number was reduced significantly after correction for drivers who had insufficient vision to drive public vehicles (P value <0.0001). Figure 1 shows the number of drivers with insufficient vision before and after refractive errors correction.
Figure 1.
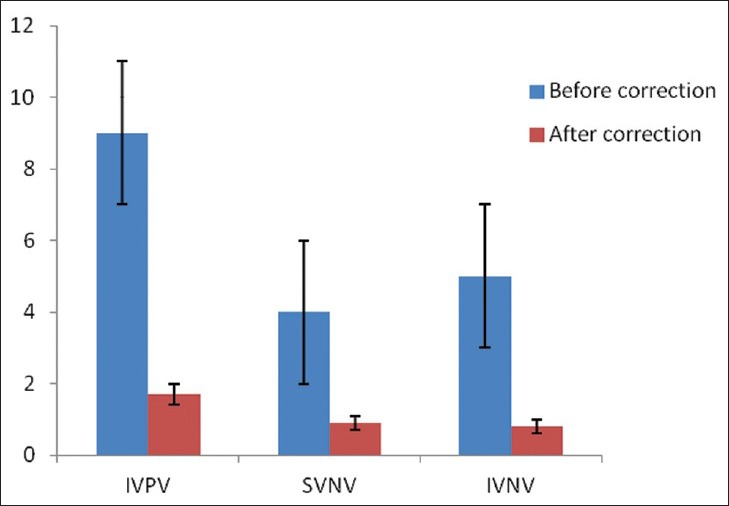
Drivers with insufficient vision, before and after correction [Data presented as percentage and 95% CI]. IVPV: Insufficient vision for public vehicles. SVNV: Sufficient vision for nonpublic vehicles. IVNV: Insufficient vision for nonpublic vehicles
From 1,061 eyes that had visual deficit (<8/10), in 729 drivers, RE, amblyopia, corneal diseases and macular diseases except age related macular degeneration (AMD) were more prevalent in drivers that were younger than 54 years of age. However, RE, AMD, cataract, and diabetic retinopathy were more prevalent in drivers older than 54 years of age (P value <0.001). Figure 2 shows causes of visual deficits in these drivers.
Figure 2.
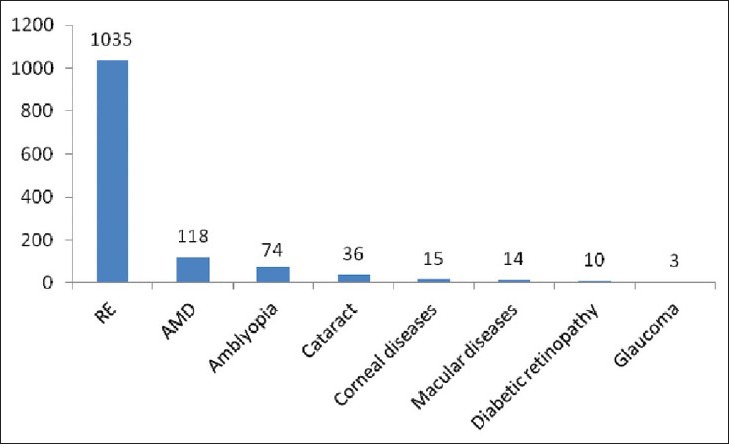
Number of different visual deficits in public vehicle drivers that cause vision less than 8/10
12 drivers (0.3%; 95% CI: 0.13-0.47) had a visual field less than 120° and therefore had insufficient vision to drive public and personal vehicles.
DISCUSSION
In this study, we investigated the visual fitness of public vehicle drivers in Kerman province, Iran. We found out that 9.0% of commercial vehicle drivers had insufficient vision to drive public vehicles and even with the best prescribed corrective glasses (lens), 1.7% of the drivers had to stop driving.
As driving is assumed to be a visually intensive task, there is a legal minimum standards of vision required for all motor vehicle drivers. The legal visual standards required to drive public vehicles in Iran are a total visual acuity of 12/10 in both eyes or 14/10, if the dominant eye's acuity is less than 10/10. Visual field standards recommended are 120° continuous horizontally. In Iran, the vision of the drivers’ license candidates is tested before siting the driving test. Annually, vehicles are subjected to Ministry of Transport testing after the first 3 years of registration, but it is not necessary for the drivers to have a similar test at least every few years.[11]
In a study in Melbourne, Australia, 2.6% of current drivers had a vision less than required to obtain a driver's license.[7] A similar study in the UK, in 2007, found that nearly 10% of the drivers were visually unfit.[12]
We realized that some drivers were monocular and one eye was legally blind. According to some researches, monocular drivers are more exposed to crash and subject of crash involvement.[13,14] Monocular drivers are also less adept than binocular drivers in sign-reading distance in both daytime and nighttime driving, which is consistent with what is known about binocular summation and binocular inhibition.[15,16]
In the current study, the main causes of sight defects were: RE, followed by AMD, amblyopia and cataract. RE and amblyopia were significantly more prevalent in younger drivers; however, AMD and cataract were mostly observed in older drivers. The ratio of drivers with visual difficulties increased with aging and the worst visual problems were in the age group of >54 years.
Detry-Morel realized that different diseases, such as ametropia, age related effects, loss of vision in one eye, cataract, glaucomatous neuropathy, and laser treatments can affect drivers’ ability to drive safely.[6] Harms et al. explained that the main cause of inadequate visual acuity is age.[17] The apparent overrepresentation of older drivers in fatal accidents is due to their greater physical weakness and susceptibility to injury when involved in a collision. Although, age itself is not a predictive factor of an increased risk for dangerous driving, the prevalence of medical states that may impair driving ability increases with age.[18]
Owsly et al. showed that motor vehicle crash risk in older drivers is elevated in those with cataract. In another study, they found out that severe contrast sensitivity impairment due to cataract elevates crash risk among older drivers, even when present in one eye.[19,20]
Besides the visual impairments, older drivers are more susceptible to early driving fatigue and disability glare. Driving fatigue, among older adults particularly, is discussed as a serious threat to the safety of older drivers.[21]
We found out the drivers’ visual impairment was mostly due to RE that could be easily corrected by glasses. This indicates that regular visual examinations not only improves the drivers’ visual fitness, but also reduces voluntary driving cessation rate. Driving cessation regardless of whether it is voluntary or involuntary can have a number of adverse consequences. Cessation of driving has been associated with decreased health-related quality of life, increased chance of depression and social isolation, reduced access to healthcare services, and increased likelihood of placement in long-term-care.[22,23,24,25,26]
There are some limitations to our study. First, we assessed the drivers’ visual acuity and visual field which can not accurately predict the drivers’ visual safety; thus, employing other types of screening approaches such as contrast sensitivity, processing speed, and divided attention tests may be beneficial. Second, drivers suffering from visual impairment will restrict their exposure to driving and this behavioral change leads to an underestimation of visual impairment.[27]
This study has demonstrated that there are many drivers with vision lower than required on the roads. While we found 9.0% of drivers with insufficient vision for driving public vehicles, the number becomes considerable when applied to the country. For example, if Iran has only 500,000 public vehicle drivers there could be approximately 45,000 drivers on the roads are visually unfit for service. This may be one of the most important causes that road traffic accidents are the second important cause of mortality in Iran. It is hard to ignore that current road safety efforts in Iran do not match the severity of the problem and new rules and regulations should be set to ban visually impaired drivers, particularly, those in old ages from driving as they may harm themselves or others.
ACKNOWLEDGMENTS
Preparation of this study was made possible by the help of the police force and the authors are grateful to transportation authorities.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Lorente RE, Fernández GS. Elderly and brain-damaged drivers in Spain. Rev Neurol. 2004;38:785–90. [PubMed] [Google Scholar]
- 2.Mohan D, Tiwari G, Khayesi M, Nafukho F. Geneva: World Health Organization; 2006. Road traffic injury prevention training manual. [Google Scholar]
- 3.Peden M, Scurfield R, Sleet D, Dinesh M, Hyder AA, Jarawan E, et al. Geneva: World Health Organization; 2004. World report on road traffic injury prevention. [Google Scholar]
- 4.Montazeri A. Road-traffic-related mortality in Iran: A descriptive study. Public Health. 2004;118:110–3. doi: 10.1016/S0033-3506(03)00173-2. [DOI] [PubMed] [Google Scholar]
- 5.Naghavi M, Shahraz S, Bhalla K, Jafari N, Pourmalek F, Bartels D, et al. Adverse health outcomes of road traffic injuries in Iran after rapid motorization. Arch Iran Med. 2009;12:284–94. [PubMed] [Google Scholar]
- 6.Detry-Morel M. Visual aptitude for automobile driving. Bull Soc Belge Ophtalmol. 2004;291:5–15. [PubMed] [Google Scholar]
- 7.Keeffe J, Jin C, Weih L, McCarty C, Taylor H. Vision impairment and older drivers: who's driving? Br J Ophthalmol. 2002;86:1118–21. doi: 10.1136/bjo.86.10.1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rogers PN, Janke MK. Performance of visually impaired heavy-vehicle operators. J Safety Res. 1992;23:159–70. [Google Scholar]
- 9.North RV. Oxford: Oxford University Press; 1993. Work and the Eye. [Google Scholar]
- 10.Nantulya VM, Reich MR. The neglected epidemic: road traffic injuries in developing countries. BMJ. 2002;324:1139–41. doi: 10.1136/bmj.324.7346.1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.The Iranian official driving rules. 2005 [Google Scholar]
- 12.Anuradha S, Potter C, Fernquest G. Vision and drivers—a South Wales survey. J Public Health. 2007;29:230–5. doi: 10.1093/pubmed/fdm031. [DOI] [PubMed] [Google Scholar]
- 13.McKnight A, Shinar D, Hilburn B. The visual and driving performance of monocular and binocular heavy-duty truck drivers. Accid Anal Prev. 1991;23:225–37. doi: 10.1016/0001-4575(91)90002-m. [DOI] [PubMed] [Google Scholar]
- 14.Rubin GS, Ng ES, Bandeen-Roche K, Keyl PM, Freeman EE, West SK. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: The SEE study. Invest Ophthalmol Vis Sci. 2007;48:1483–91. doi: 10.1167/iovs.06-0474. [DOI] [PubMed] [Google Scholar]
- 15.Blake R, Sloane M, Fox R. Further developments in binocular summation. Percep Psychophys. 1981;30:266–76. doi: 10.3758/bf03214282. [DOI] [PubMed] [Google Scholar]
- 16.Pardhan S, Gilchrist J, Douthwaite W. The effect of spatial frequency on binocular contrast inhibition. Ophthalmic Physiol Opt. 1989;9:46–9. doi: 10.1111/j.1475-1313.1989.tb00804.x. [DOI] [PubMed] [Google Scholar]
- 17.Harms H, Kröner B, Dannheim R. Ophthalmological experiences with automobile drivers with inadequate vision. Klin Monbl Augenheilkd. 1984;185:77–85. doi: 10.1055/s-2008-1054574. [DOI] [PubMed] [Google Scholar]
- 18.Beck LF, Dellinger AM, O’Neil ME. Motor vehicle crash injury rates by mode of travel, United States: using exposure-based methods to quantify differences. Am J Epidemiol. 2007;166:212–8. doi: 10.1093/aje/kwm064. [DOI] [PubMed] [Google Scholar]
- 19.Owsley C, McGwin G, Sloane M, Wells J, Stalvey BT, Gauthreaux S. Impact of cataract surgery on motor vehicle crash involvement by older adults. JAMA. 2002;288:841–9. doi: 10.1001/jama.288.7.841. [DOI] [PubMed] [Google Scholar]
- 20.Owsley C, Stalvey BT, Wells J, Sloane ME, McGwin G., Jr Visual risk factors for crash involvement in older drivers with cataract. Arch Ophthalmol. 2001;119:881–7. doi: 10.1001/archopht.119.6.881. [DOI] [PubMed] [Google Scholar]
- 21.Brown ID. Driver fatigue. Human Factors. Hum Factors. 1994;36:298–314. doi: 10.1177/001872089403600210. [DOI] [PubMed] [Google Scholar]
- 22.Decarlo DK, Scilley K, Wells J, Owsley C. Driving habits and health-related quality of life in patients with age-related maculopathy. Optom Vis Sci. 2003;80:207–13. doi: 10.1097/00006324-200303000-00010. [DOI] [PubMed] [Google Scholar]
- 23.Fonda SJ, Wallace RB, Herzog A. Changes in driving patterns and worsening depressive symptoms among older adults. J Gerontol B Psychol Sci Soc Sci. 2001;56:S343–51. doi: 10.1093/geronb/56.6.s343. [DOI] [PubMed] [Google Scholar]
- 24.Owsley C, McGwin G, Scilley K, Girkin CA, Phillips JM, Searcey K. Perceived barriers to care and attitudes about vision and eye care: focus groups with older African Americans and eye care providers. Invest Ophthalmol Vis Sci. 2006;47:2797–802. doi: 10.1167/iovs.06-0107. [DOI] [PubMed] [Google Scholar]
- 25.Owsley C, McGwin G, Jr, Stalvey BT, Weston J, Searcey K, Girkin CA. Educating older African Americans about the preventive importance of routine comprehensive eye care. J Natl Med Assoc. 2008;100:1089–95. doi: 10.1016/s0027-9684(15)31450-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ragland DR, Satariano WA, MacLeod KE. Driving cessation and increased depressive symptoms. J Gerontol A Biol Sci Med Sci. 2005;60:399–403. doi: 10.1093/gerona/60.3.399. [DOI] [PubMed] [Google Scholar]
- 27.Owsley C, McGwin Jr., G Vision and driving. Vision Res. 2010;50:2348–61. doi: 10.1016/j.visres.2010.05.021. [DOI] [PMC free article] [PubMed] [Google Scholar]