

Abstract
Purpose
Indoor tanning usually begins during adolescence, but few strategies exist to discourage adolescent use. We developed and tested a parent–teenager intervention to decrease indoor tanning use.
Methods
Through focus groups, we identified key messages to enhance parent–teenager communication about indoor tanning, and then developed a pamphlet for parents and postcards for adolescents to use in a direct mail experiment with randomly selected households. Two weeks after the mailing, we asked intervention parents (n = 87) and adolescents (n = 69) and nonintervention parents (n = 31) and adolescents (n = 28) about intervention receipt and content recall, parental concern, monitoring, parent–teenager conversations, and indoor tanning intention.
Results
In intervention households, 54% of mothers and 56% of girls recalled receipt and reported reading materials, but few boys and no fathers did. Among mothers, 57% in intervention households indicated concern about daughters’ indoor tanning, and 25% would allow daughters to tan indoors, whereas 43% of nonintervention mothers had concerns and 46% would allow indoor tanning. Fewer girls in intervention households than in nonintervention households thought parents would allow indoor tanning (44% vs. 65%), and fewer intended to tan indoors (36% vs. 60%). Most mothers and daughters who read the intervention materials also reported discussions about indoor tanning. Moreover, the less likely girls were to think that their mothers would allow indoor tanning, the less likely it was that they intended to tan indoors, a relationship mediated by perceptions of maternal monitoring.
Conclusions
A systematic qualitative and quantitative research approach yielded well-received indoor tanning prevention messages for mothers and female adolescents. Enhancing maternal monitoring has potential to decrease adolescent indoor tanning.
Keywords: Indoor tanning, Interventions, Melanoma, Adolescents, Health communication
Melanoma is one of the fastest increasing cancers in the U.S. and accounts for 75% of all skin cancer deaths [1]. Furthermore, melanoma is the second and third most common cancer among women and men under age 40 years, respectively [2]. Solar ultraviolet radiation is an established risk factor for melanoma [3], and recently, artificial ultraviolet radiation obtained from indoor tanning devices was declared to be carcinogenic to human skin [4]. In particular, use of indoor tanning at a young age is widely believed to confer increased risk of melanoma [5]. This is especially concerning because indoor tanning typically starts during adolescence and is more commonly practiced by younger than older adults [6–8]. Recent studies offer evidence to support two different mechanisms by which early onset of indoor tanning affects melanoma risk. Initiation of the behavior at a young age may increase the cumulative exposure, leading to greater likelihood of melanoma [9,10]. For a subset of persons genetically predisposed to melanoma, earlier use of indoor tanning may accelerate melanoma development and cause it to occur at a younger age [10].
Although 16% of high school students overall and 25% of high school girls report indoor tanning [11], and the median age of initiation among girls is 17 years (interquartile range, 16–18 years) [12], the problem of indoor tanning among adolescents has yet to become an active area for intervention. Altogether, just four intervention studies targeting indoor tanning use, all of college-aged females, have been reported: a pilot study of a 30-minute individual counseling session versus a personalized feedback sheet [13], a pilot study that used ultraviolet photography to show skin damage [14], a pilot study that compared narrative with statistical messages [15], and a randomized controlled trial that tested the efficacy of a booklet that encouraged alternatives to enhance appearance other than indoor tanning [16]. Given the dearth of research on interventions in this area for the adolescent population, we conducted a study that incorporated qualitative and quantitative methods for the purpose of developing an intervention to prevent adolescent indoor tanning. Because parents’ indoor tanning has been consistently and strongly predictive of adolescents’ indoor tanning [17–20], and family interaction has been identified as an important influence on the health behavior of children and adolescents, including sun protection [21–24], we included both parents and adolescents in the project with the goal of developing an intervention that enhanced family communication on this topic. Here, we present the findings from our research endeavor.
Methods
Overview
As described in detail below, we conducted focus groups with parents and teenagers to inform the content of our parent–teenager indoor tanning intervention, pretested the intervention with parents and teenagers via a semistructured in-depth telephone interview, and pilot-tested the intervention to determine its reach into the target population. We recruited participants from the membership of HealthPartners, a large integrated health system of more than 800,000 residents in the Minneapolis–St. Paul, Minnesota, metropolitan area with similar characteristics to the state as a whole, and from two area suburban high schools. At each stage, parents provided consent for themselves and their adolescents, whereas we asked adolescents for their assent. Institutional Review Boards at the University of Minnesota and HealthPartners approved the study.
Focus groups
From March through June 2008, we conducted six focus groups with adolescents aged 14–16 years, and two with mothers or fathers of adolescents in the 14- to 16-year age range (one of these included parents related to adolescents who also participated in a focus group). We restricted three focus groups for adolescents to girls who tanned indoors (n = 13), one to girls who had not tanned indoors (n = 6), and two to boys regardless of their indoor tanning experience (n = 13; one indoor tanner). Twenty-five adolescents were non-Hispanic white, four were African-American, two were Hispanic, and one was Native American. Among 10 parents (nine female and one male), eight were non-Hispanic white, one was African-American, and one was Hispanic. Parents ranged in age from 46 to 53 years. Of the 10 parents, seven had at least some college education.
We gathered viewpoints regarding knowledge and attitudes about indoor tanning, preferred media for message delivery, barriers to parent–teenager conversations, and parental roles regarding adolescent indoor tanning. We transcribed and analyzed audio recordings from the focus group discussions using a thematic approach [25]. From these data, we derived a set of themes and worked with a graphic designer and science writer to create the intervention materials.
Pretest
After we created draft versions of intervention materials in fall 2008, we sent them to 10 parents of adolescents ages 14–16 years and 10 adolescents of the same age in December 2008 to January 2009. After giving each participant about a week to review, we then conducted in-depth telephone interviews for a detailed assessment of relevance, appearance, and comprehension of the intervention materials.
Pilot test
The pilot test took place in April to June 2009. From 500 randomly selected households that were HealthPartners members with an adolescent (boy or girl) aged 15 or 16 years, and that had not participated in our focus groups or pretest, we randomized 70% to receive the intervention materials and 30% to serve as a comparison group. Before sending the intervention materials, we sent a letter to all households informing the parents that they and their adolescent could be selected for a telephone interview on skin health and behavior, and that they might receive some mailed information on that topic. We planned to interview approximately 100 parents and 100 adolescents (limited to one parent and one adolescent per household) while maintaining the 7:3 ratio of intervention to comparison households to ensure an adequate number of participants from intervention households likely to recall receiving the materials. Telephone interviews were completed by 87 parent–teen dyads, 31 parents only, and 10 adolescents only. Altogether, we interviewed 87 parents and 69 adolescents in intervention households and we interviewed 31 parents and 28 adolescents in nonintervention households (70.7% of eligible households contacted by telephone). The primary purpose of the interview was to determine whether the interviewee recalled receiving the intervention materials, and if so, whether the materials were read. We asked these questions of both intervention and comparison groups to determine the possibility of biased recall. Among those who indicated having read the materials, we assessed the accuracy with which they recalled the content and inquired about their satisfaction with the materials. From all study participants, we also collected information about indoor tanning-related knowledge, attitudes, and behavior using measures reported in prior studies [17,18,20,26,27].
In descriptive analyses, we compared responses from parents and adolescents who were mailed the intervention materials with the responses of those who were not mailed the materials, testing for differences using chi-square statistics. We also conducted a mediation analysis using structural equation models to understand hypothesized mechanisms by which the intervention could affect adolescents’ intention to tan indoors. We restricted this analysis to dyads in which both the parent and adolescent were female (n = 60). Among these dyads, 43% of mothers and 38% of daughters reported reading the intervention materials. The outcome, daughters’ intention to tan indoors, was a factor score derived from three items similar to a validated measure used to assess intention to smoke [28] (will try indoor tanning soon, will try if offered by friends, or will try in next 12 months). We estimated standardized regression coefficients to represent changes in daughters’ intention to tan indoors (in standard deviation) that correspond to one standard deviation increase in the predictor in each hypothesized path. We conducted the mediation analysis using Mplus, version 5.0 (Los Angeles, CA) [29].
Results
Focus groups
Table 1 lists themes and quotes from the focus groups. Both parents and adolescents expressed interest in the adverse consequences of indoor tanning on health and appearance. Girls who tanned indoors were particularly interested in how likely and how quickly these consequences occurred. Participants also inquired about the benefits of indoor tanning (e.g., getting vitamin D or preventing sunburn), and some wondered whether indoor was safer than outdoor tanning. Participants indicated that they were not aware of state regulations pertaining to indoor tanning by minors.
Table 1.
Themes and quotes from focus group discussions: pilot test of intervention to reduce indoor tanning by teenagers, 2009
| Themes | Quotes |
|---|---|
| Topics of Interest | |
| Health effects | “Risk of skin cancer or what kind of diseases—what could they get? What do they get besides the tan?” Female parent “Consequences … like disease, skin cancer or something.” Male teenager “Problems it does to your skin and your health, because some people don’t really understand all that.” Female teenager, tanner |
| Appearance | “An interesting thing would be to give me a ‘this is what someone who’s tanned for 10 years—for 20 years—for 30 years—looks like.’” Female parent “Yeah, like, is that true [that indoor tanning gives you wrinkles]? I don’t know if it’s true or not.” Female teenager, tanner |
| Possible benefits | “It’s a good source of vitamin D …” Female parent “[People] go tanning so that when they get to where they’re going [for vacations in the winter], they don’t burn. Does that work?” Female parent “Like, helps appearance, helps confidence, how it relaxes …” Female teenager, tanner |
| Personal story | “It would be interesting to follow a story of someone … just see if they have a higher incidence of skin cancer or something.” Female parent “Well, like if you really want to, like, go scare somebody, you could tell someone, like, a disaster story.” Female teenager, tanner |
| Safer than the sun | “I guess one of the other topics would be, is tanning worse than the sun? Is tanning better than the sun?” Male parent “Is it health[ier than tanning outdoors] that I should do it?” Male teenager |
| Regulations | “I don’t know about the ” Female parent law. “I was not aware of a law—it’s nothing we’ve ever had to think about.” Female parent |
| Barriers to parent-teenager conversation | |
| Not important/relevant | “They’re not asking to tan to get it, so it must not be that important to them.” Female parent “I don’t know. I never really thought of indoor tanning in my life. Maybe I’m just used to my mom saying pale skin, fair skin is nice. I don’t know.” Female teenager, nontanner “We basically just both agree how stupid it is…” Male teenager |
| Need for conversation triggers | “We have a discussion about it—I mean, for prom, I’m sure you’ve heard that—they all wanna be tan, they all—they can’t be white-looking.” Male parent “I just ask her if I can go [tan indoors], and she’ll say, ‘Yeah.’” Female teenager, tanner “[How we started the conversation was that] we got some things in the mail—this new place opened by our house, and you can get, like, a free—3 tans in a row.” Male teenager |
| Lack of credible information | “I’ve never researched it … I guess I would have to do some research if she expressed interest in it.” Female parent “I didn’t really know [anything about tanning].” Female teenager, tanner |
Indoor tanning appeared to be an infrequent topic of conversation among parents and adolescents. Some parents thought it was not a relevant topic because their teenagers had not expressed interest in tanning indoors. Adolescents, particularly boys, also thought that indoor tanning was not a topic that they would discuss with their parents. Conversations related to indoor tanning were triggered by upcoming school dances or receiving indoor tanning advertisements in the mail. Both parents and adolescents commented that their lack of accurate knowledge about the topic was a barrier to discussion.
The intervention
We created a pamphlet and postcard for delivery via U.S. mail for parents. Content included information about health risks associated with indoor tanning, common misperceptions (e.g., a base tan prevents sunburn), parental influences (e.g., parents’ own use of indoor tanning), industry tactics, and tips for talking to teenagers about indoor tanning. We created three postcards for adolescents to be delivered about 2 weeks apart. Topics included health risks, common misperceptions, and industry tactics, as well as alternatives to indoor tanning (e.g., makeup). Opportunities to encourage parent–teenager conversation about indoor tanning were incorporated into the intervention. The first teenager postcard was embedded in the parent’s pamphlet, which required the parent to then share the information with her child. The second teenager postcard included a quiz that teenagers were encouraged to use to test their parents’ knowledge. In addition, the pamphlet and all postcards included the address of a website where parents and teenagers could together learn more about the topic, view videos, and access additional resources (e.g., material from the American Cancer Society).
Pretesting
Adolescents and parents who participated in pretesting the intervention materials correctly described the key messages and found the materials to be age appropriate and informative. Based on their feedback, we modified the content (e.g., we placed more emphasis on the parenting tips) and images (e.g., we reduced the number of images on some of the postcards). Final versions of the pamphlet and postcards can be accessed as supplemental data here.
Pilot study findings
Characteristics of interviewed parents and teenagers in intervention and nonintervention households were similar. Among parents, 62% reported light or extremely light skin; 60% had a college or advanced degree. About 23% of adolescents and 15% of parents had tanned indoors during the previous year. Nearly all survey respondents among parents and about three quarters of survey respondents among adolescents were female (Table 2). Among those randomly assigned to receive the intervention materials, no fathers and fewer than half of boys recalled receiving the pamphlet or postcards, whereas 71% of mothers and 88% of girls recalled receiving them. A substantial proportion of interviewed mothers and girls in intervention households reported reading the materials, for a total reach into the target population of 54% of mothers and 56% of girls. Whereas a small percentage of mothers, boys, and girls in the comparison group reported receipt of the materials, none reported reading the materials. Because mothers and girls were the primary beneficiaries of the intervention, we restricted subsequent analyses to females.
Table 2.
Percentage of parents and teenagers who recalled receiving or reading pamphlet or postcards: pilot test of intervention to reduce indoor tanning by teenagers, 2009
| Mailed pamphlet or postcards
|
||||||||
|---|---|---|---|---|---|---|---|---|
| Yes
|
No
|
|||||||
| Parents
|
Teenagers
|
Parents
|
Teenagers
|
|||||
| N | % | N | % | N | % | N | % | |
| Total respondents | 87 | 100.0 | 69 | 100.0 | 31 | 100.0 | 28 | 100.0 |
| Female | 83 | 95.4 | 50 | 72.5 | 28 | 90.3 | 20 | 71.4 |
| Male | 4 | 4.6 | 19 | 27.5 | 3 | 9.7 | 8 | 28.6 |
| Recalled receipt | ||||||||
| Female | 59 | 71.1 | 44 | 88.0 | 3 | 10.7 | 1 | 5.0 |
| Male | 0 | 0.0 | 8 | 42.1 | 0 | 0.0 | 2 | 25.0 |
| Read materials (if receipt recalled) | ||||||||
| Female | 45 | 76.3 | 28 | 63.6 | 0 | 0.0 | 0 | 0.0 |
| Male | N/A | 3 | 37.5 | N/A | 0 | 0.0 | ||
| Total reached (if receipt recalled and read) | ||||||||
| Female | 45 | 54.2 | 28 | 56.0 | 0 | 0.0 | 0 | 0.0 |
| Male | 0 | 0.0 | 3 | 15.8 | 0 | 0.0 | 0 | 0.0 |
N/A = Questions were not asked or not applicable.
Among female participants who had read the intervention materials (45 mothers and 28 girls), a high proportion correctly recalled information about the risk of melanoma associated with indoor tanning use (Table 3). Girls were more likely than mothers to recall information about burns and wrinkles, and alternative ways to enhance appearance or to obtain vitamin D. Although mothers appeared to receive the message related to industry practices targeting teenagers, only a small proportion recalled content regarding state laws against teenager use of indoor tanning. Only a small percentage (2%–7%) of both the mothers and girls recalled information that was not included (e.g., weight loss). Satisfaction with the intervention materials was high among both mothers and girls; 80% of mothers and 68% of girls reported talking with each other about intervention content.
Table 3.
Accuracy of content recall and satisfaction with intervention among mothers and girls who reported reading pamphlet or postcards: pilot test of intervention to reduce indoor tanning by teenagers, 2009
| Mothers (n = 45) | Girls (n = 28) | |
|---|---|---|
| Percentage who correctly recalled content | ||
| Indoor tanning and … | ||
| Melanoma risk | 71.1 | 75.0 |
| Burns and wrinkles | 48.9 | 78.6 |
| Weight loss (bogus item) | 2.2 | 7.1 |
| Other ways to look good | 26.7 | 71.4 |
| Other ways to get vitamin D | 53.3 | 60.7 |
| Beauty queen with melanoma | N/A | 71.4 |
| Base tan not protective | 64.4 | N/A |
| State laws for parental permission | 20.0 | N/A |
| Industry targets teenagers | 80.0 | N/A |
| Tips for talking with teenagers | 66.7 | N/A |
| Agree or strongly agree materials meant for them (%) | 63.6 | 89.3 |
| Learned some or a lot (%) | 77.8 | 85.7 |
| Liked materials some or a lot (%) | 93.3 | 92.9 |
| Talked with each other about intervention content (%) | 80.0 | 67.9 |
| Retained pamphlet (%) | 42.4 | N/A |
| Retained postcards (%) | 71.2 | 50.0 |
N/A = Questions were not asked or not applicable.
We performed an intent-to-treat analysis to compare indoor tanning-related knowledge, attitudes, perceived norms, and behavior between mothers and girls who were or were not mailed the intervention materials (Table 4). Even though only a few differences were statistically significant, mothers who were sent the intervention materials tended to report higher knowledge, less favorable attitudes, and a lower normative perception about indoor tanning than those who were not sent the intervention materials. Among mothers, 57% in intervention households and 43% in nonintervention households indicated concern about their daughters’ indoor tanning; 25% of intervention mothers would allow daughters to tan indoors, but 46% of nonintervention mothers would allow it. Compared with mothers, daughters had fewer differences in knowledge and attitudes between those who were and were not mailed the intervention material, except for perception of peer use of indoor tanning, which was statistically significantly lower among girls in intervention households. In addition, a lower proportion of girls in intervention households than girls in nonintervention households thought their parents would allow indoor tanning (44% vs. 65%) and expressed an intention to tan indoors (36% vs. 60%).
Table 4.
Comparison of indoor tanning knowledge, attitudes, perceived norms, and behavior between mothers and girls who were and were not mailed pamphlet or postcards: pilot test of intervention to reduce indoor tanning by teenagers, 2009
| Mailed pamphlet or postcards
|
||||
|---|---|---|---|---|
| Mothers
|
Girls
|
|||
| Yes (n = 83) | No (n = 28) | Yes (n = 50) | No (n = 20) | |
| Knowledge | ||||
| Percentage who agreed or were correct that … | ||||
| Skin cancer is common | 98.8 | 89.3a | 98.0 | 95.0 |
| Tanned skin is damaged | 92.8 | 85.7 | 88.0 | 95.0 |
| Melanoma is increasing | 86.8 | 89.3 | 90.0 | 90.0 |
| Indoor tanning is safer than sun | 1.2 | 3.6 | 0 | 4.0 |
| Indoor tanning could cause cancer | 94.0 | 96.4 | 100.0 | 100.0 |
| Base tan protects from sun | 21.7 | 25.0 | 36.0 | 45.0 |
| Alternatives to look good exist | N/A | N/A | 90.0 | 85.0 |
| Laws exist for parental consent | 18.1 | 0a | 28.0 | 5.0 |
| Attitudes | ||||
| Percentage who agreed that … | ||||
| People with tans are more attractive | 77.1 | 88.9 | 49.0 | 70.0 |
| Chances of skin cancer are small | 24.1 | 37.0 | 32.0 | 30.0 |
| Tanned skin looks healthier | 78.6 | 66.3 | 34.0 | 40.0 |
| Industry markets to teenagers | 96.1 | 96.4 | 90.0 | 100.0 |
| Industry targeting teenagers is serious | 92.2 | 85.7 | N/A | N/A |
| One gets compliments on tanned skin | 80.0 | 67.9 | 90.0 | 100.0 |
| Indoor tanning lifts spirits | 59.5 | 84.6a | 57.1 | 50.0 |
| Indoor tanning is relaxing | 46.3 | 61.5 | 59.2 | 83.3 |
| Perceived norms | ||||
| Percentage who believed that … | ||||
| >50% of peers use indoor tanning | 48.8 | 63.0 | 55.1 | 79.0a |
| Behavior | ||||
| Percentage who … | ||||
| Talked to teenager or parent about indoor tanning | 43.4 | N/A | 38.0 | N/A |
| Think parent would allow indoor tanning | N/A | N/A | 44.0 | 65.0 |
| Would use indoor tanning if friend offered free session | N/A | N/A | 56.0 | 65.0 |
| Were concerned if teenager tanned indoors occasionally | 56.6 | 42.7 | N/A | N/A |
| Were concerned if teenager tanned indoors regularly | 96.4 | 96.4 | N/A | N/A |
| Would allow teenager to tan indoors | 25.3 | 46.4a | N/A | N/A |
| Intend to tan indoors soon | N/A | N/A | 36.0 | 60.0 |
| Intend to tan indoors in next 12 months | 14.5 | 25.0 | 44.0 | 55.0 |
N/A = Questions were not asked or not applicable.
Difference between groups was statistically significant at p < .05.
Figure 1 shows results of the mediation analysis. Although mothers’ reading the intervention materials was positively associated with knowledge of state laws, higher knowledge of state laws was statistically significantly correlated with lower likelihood that mothers would disallow daughters to tan indoors. However, a greater likelihood of mothers’ disallowing daughters to tan indoors was associated with a lower intention to tan indoors among daughters, both directly (path A; standardized regression coefficient [SRC] = −.40, p = .01) and indirectly through daughters’ perception that parents would allow indoor tanning (path B*G; SRC = −.18, p = .02). Daughters who read the materials also reported lower intention to tan indoors than did daughters who had not read the materials (sum of paths C, D*G, and E*F; SRC = −.36, p = .02). About 39% of the effect of reading the materials on daughters’ intention to tan indoors was through the daughters’ perception that mothers would allow indoor tanning, and the daughters’ disagreeing with the idea that a tan was attractive (total indirect effect, the sum of paths D*G and E*F; SRC = −.14, p = .04).
Figure 1.
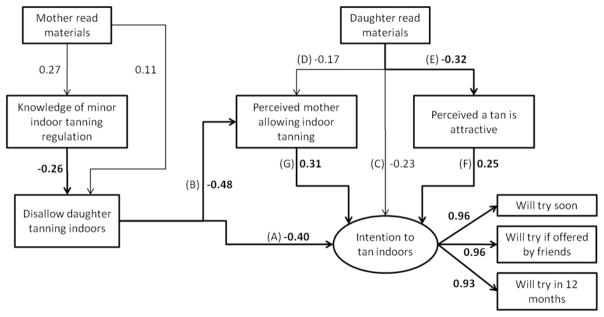
Results of the mediation analysis: pilot test of intervention to reduce indoor tanning by teenagers, 2009. The total effect of mothers’ disallowing daughters to tan indoors on daughters’ susceptibility to indoor tanning is the sum of the direct [Path A] and indirect effects [Path B*G]. The total effect of daughters’ reading the materials on susceptibility to indoor tanning is the sum of the direct effect [Path C] and indirect effects through the perception that mother allows indoor tanning [Path D*G] and that a tan is attractive [Path E*F]. Bolded paths and standardized regression coefficients are statistically significant (p < .05).
Discussion
Through a formal and systematic approach that involved the end user, we created messages about indoor tanning that were salient to parents and adolescents and served as triggers for conversation between them about the topic. Because no interventions for indoor tanning have been reported for adolescents, focus groups were critical to define the messages. Our pretest of the intervention materials with both parents and adolescents led to modifications to improve the relevance of the messages and the visual presentation, and it confirmed our planned mode of delivery. We considered reaching more than half of mothers and girls with our mailed messages to be a success. Given today’s electronic and social media environment, and that print media accounts for only 38 minutes of the total average time (7 hours 38 minutes) that children or adolescents aged 8–18 years spend with media in a day [30], results from our pilot test suggest that a mailed intervention to adolescents may be a novelty that cuts through the myriad of electronic media.
Although we randomized households to be mailed the intervention materials, our pilot test was not a true randomized trial. We did not collect baseline information before mailing the intervention materials from experimental or comparison households; thus, we could not assess change in knowledge, attitudes, or intention to tan indoors. Also, because indoor tanning is a seasonal behavior, and we asked only about indoor tanning use in the previous year, the short interval (about 2 weeks) between receipt of the final intervention mailing and the interview eliminated the possibility of assessing whether our intervention had any effect on actual indoor tanning. In addition, our sample size for the pilot test was small. Therefore, we were able to perform only crude data analyses and our results may be subject to selection bias.
Another limitation is that we used the same messages for adolescents whether or not they had tanned indoors. An argument could be made that strategies for prevention of the behavior may differ from those needed to help adolescents refrain from indoor tanning use. However, in a previous study, we found that associations were similar between knowledge and attitudes and the likelihood of intention to initiate or continue indoor tanning among adolescents [26]. Our approach allows for greater dissemination because it does not require knowledge of indoor tanning status. Still, more formative work may be necessary to develop strategies to help adolescents quit tanning indoors.
Although girls and young women are primary users of indoor tanning [8,11], we included boys and fathers at every step of our intervention development, to meet federal guidelines against gender bias in research. Our data provide clear support for focusing future interventions to prevent indoor tanning use by adolescent girls. The fact that no fathers recalled seeing the parent pamphlet is consistent with mothers typically taking responsibility for their family’s health and spending more time with their children, a pattern that has persisted over recent decades in the U.S. despite some changes [31]. Boys clearly showed only limited interest in the information, as indicated by the fact that a small proportion recalled receipt and reported reading the materials. Therefore, targeting girls for intervention is a more efficient use of resources. Furthermore, interventions could incorporate messages and images that would be more appealing to girls than boys, and thus be potentially more effective in changing the behavior in the target population.
We and others have previously shown that maternal influences such as the mother’s use of indoor tanning (role modeling), allowing her adolescent to tan indoors (permissiveness), concern about her adolescent’s indoor tanning use, and knowledge and attitudes are strong predictors of adolescent indoor tanning use [17–20]. Of these possible mechanisms, we were able to examine only parental permissiveness because there was limited variation in our small sample and because of the inability to assess change in indoor tanning just 2 weeks after the intervention mailing. We found that the parental permissiveness pathway explained a considerable proportion of the likelihood of daughters’ intention to tan indoors. Future interventions that persuade parents to be less permissive about adolescent indoor tanning use could be especially effective. As posited by the Protection Motivation Theory [32], individuals are motivated to perform a protective behavior, such as disallowing their teenagers to tan indoors, when they perceive the consequences of not performing the protective behavior to be risky (in terms of severity and susceptibility), that they are capable of performing the protective behavior (self-efficacy), and that performing the protective behavior would prevent the risk (response efficacy). Because our data suggested that parents already recognized indoor tanning as harmful to health, interventions that enhance parental self-efficacy (e.g., coaching parents to discuss indoor tanning with their children) and response efficacy (e.g., emphasizing the importance of parental monitoring of teenagers’ indoor tanning use) may motivate parents to disallow and thereby prevent their adolescents from tanning indoors.
Future directions also include expanding the intervention and testing its efficacy to prevent indoor tanning by the target population. In light of the importance of interpersonal ties and connections as a venue for public health interventions [33,34], fruitful next steps for interventions (such as the one we describe here) could be to provide mothers with the information needed to discuss indoor tanning with their daughters (via pamphlets and postcards), offer mothers resources to enhance parenting skills and promote mother–daughter conversations (e.g., via an interactive website), prime daughters to be receptive to their mothers’ conversations (via mailed postcards), and cue mothers to have a conversation with their daughters (e.g., via text messaging) [35,36]. Whereas this approach addresses intrapersonal and interpersonal influences of the socioecological model [37], reducing indoor tanning by adolescents also lends itself to intervention at organizational and environmental levels. For example, schools could be enlisted to refuse advertising or event sponsorship from indoor tanning salons [38,39], health care providers could be encouraged to advise mothers and daughters against indoor tanning use (consistent with the most recent American Academy of Pediatrics policy statement on protecting children from ultraviolet radiation [40]), and state and federal laws could be strengthened to prohibit indoor tanning by minors (as California has recently done and as is currently under review by the Food and Drug Administration).
In conclusion, we developed and demonstrated the feasibility of a low-cost and technologically simple intervention to encourage parent–teenager conversations about indoor tanning and to discourage indoor tanning by adolescents. Use of both qualitative and quantitative methods ensured a relatively thorough understanding of the strengths and weaknesses of our product. We now need large-scale trials to assess whether engaging both mothers and daughters in conversation about the risks of indoor tanning and enhancing parental influences via permissiveness and role modeling will be effective in preventing, discontinuing, or reducing a behavior that begins during adolescence and puts girls at increased risk of melanoma.
Supplementary Material
IMPLICATIONS AND CONTRIBUTION.
Effective strategies are needed to curb indoor tanning by adolescent girls. This study developed and pilot-tested an intervention to enhance mothers’ influence over daughters’ use of indoor tanning by encouraging informed conversations between mothers and daughters. Preliminary results support this approach, but further evaluation in a randomized controlled trial is needed.
Acknowledgments
Publication of this article was supported by the Centers for Disease Control and Prevention.
Funding for this research was provided by grant number R21CA118222 from the National Cancer Institute.
Footnotes
The authors report no potential conflicts of interest.
Supplementary data related to this article can be found online at http://dx.doi.org/10.1016/j.jadohealth.2012.08.009
References
- 1.Horner MJ, Ries L, Krapcho M, et al., editors. SEER cancer statistics review, 1975–2006. Bethesda (MD): National Cancer Institute; 2009. [Google Scholar]
- 2.Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975–2008. Bethesda (MD): National Cancer Institute; 2011. [Accessed January 13, 2012]. Available at: http://seer.cancer.gov/csr/1975_2008. [Google Scholar]
- 3.Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 2005;41:45–60. doi: 10.1016/j.ejca.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 4.WHO International Agency for Research on Cancer. A review of human carcinogens—Part D: Radiation. Lancet Oncol. 2009;10:751–2. doi: 10.1016/s1470-2045(09)70213-x. [DOI] [PubMed] [Google Scholar]
- 5.WHO International Agency for Research on Cancer Working Group on Artificial Ultraviolet (UV) Light and Skin Cancer. The association of use of sunbeds with cutaneous malignant melanoma and other skin cancers: A systematic review. Int J Cancer. 2006;120:1116–22. doi: 10.1002/ijc.22453. [DOI] [PubMed] [Google Scholar]
- 6.Lazovich D, Sweeney C, Forster J. Prevalence of indoor tanning use in Minnesota, 2002. Arch Dermatol. 2005;141:523–4. doi: 10.1001/archderm.141.4.523. [DOI] [PubMed] [Google Scholar]
- 7.Heckman CJ, Coups EJ, Manne SL. Prevalence and correlates of indoor tanning among US adults. J Am Acad Dermatol. 2008;58:769–80. doi: 10.1016/j.jaad.2008.01.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Choi K, Lazovich D, Southwell B, et al. Prevalence and characteristics of indoor tanning use among men and women in the United States. Arch Dermatol. 2010;146:1356–61. doi: 10.1001/archdermatol.2010.355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lazovich D, Vogel RI, Berwick M, et al. Indoor tanning and risk of melanoma: A case-control study in a highly exposed population. Cancer Epidemiol Biomarkers Prev. 2010;19:1557–68. doi: 10.1158/1055-9965.EPI-09-1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cust AE, Armstrong BK, Goumas C, et al. Sunbed use during adolescence and early adulthood is associated with increased risk of early-onset melanoma. Int J Cancer. 2011;128:2425–35. doi: 10.1002/ijc.25576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Guy GP, Tai E, Richardson LC. Use of indoor tanning devices by high school students in the United States, 2009. [Accessed January 13, 2012];Prev Chronic Dis. 2011 8:A116. Available at: http://www.cdc.gov/pcd/issues/2011/sep/10_0261.htm. [PMC free article] [PubMed] [Google Scholar]
- 12.Lostritto K, Ferrucii LM, Carmel B, et al. Lifetime history of indoor tanning in young people: A retrospective assessment of initiation, persistence, and correlates. BMC Public Health. 2012;12:118. doi: 10.1186/1471-2458-12-118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Turrisi R, Mastroleo NR, Stapleton J, et al. A comparison of 2 brief intervention approaches to reduce indoor tanning behavior in young women who indoor tan very frequently. Arch Dermatol. 2008;144:1521–4. doi: 10.1001/archderm.144.11.1521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gibbons FX, Gerrard M, Lane DJ, et al. Using UV photography to reduce use of tanning booths: A test of cognitive mediation. Health Psychol. 2005;24:358–63. doi: 10.1037/0278-6133.24.4.358. [DOI] [PubMed] [Google Scholar]
- 15.Greene K, Brinn LS. Messages influencing college women’s tanning bed use: Statistical versus narrative evidence format and a self-assessment to increase perceived susceptibility. J Health Commun. 2003;8:443–61. doi: 10.1080/713852118. [DOI] [PubMed] [Google Scholar]
- 16.Hillhouse J, Turrisi R, Stapleton J, Robinson J. A randomized controlled trial of an appearance-focused intervention to prevent skin cancer. Cancer. 2008;113:3257–66. doi: 10.1002/cncr.23922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stryker JE, Lazovich D, Forster JL, et al. Maternal/female caregiver influences on adolescent indoor tanning. J Adolesc Health. 2004;35:528 e1–9. doi: 10.1016/j.jadohealth.2004.02.014. [DOI] [PubMed] [Google Scholar]
- 18.Hoerster KD, Mayer JA, Woodruff SI, et al. The influence of parents and peers on adolescent indoor tanning behavior: Findings from a multi-city sample. J Am Acad Dermatol. 2007;57:990–7. doi: 10.1016/j.jaad.2007.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cokkinides VE, Weinstock MA, O’Connell MC, et al. Use of indoor tanning sunlamps by US youth, ages 11–18 years, and by their parent or guardian caregivers: Prevalence and correlates. Pediatrics. 2002;109:1124–30. doi: 10.1542/peds.109.6.1124. [DOI] [PubMed] [Google Scholar]
- 20.Mayer J, Woodruff S, Slymen D, et al. Adolescents’ use of indoor tanning: A large-scale evaluation of psychosocial, environmental, and policy-level correlates. Am J Public Health. 2011;101:930–8. doi: 10.2105/AJPH.2010.300079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Devore ER, Ginsburg KR. The protective effects of good parenting on adolescents. Curr Opin Pediatr. 2005;17:460–5. doi: 10.1097/01.mop.0000170514.27649.c9. [DOI] [PubMed] [Google Scholar]
- 22.Riesch SK, Anderson LS, Krueger HA. Parent-child communication processes: Preventing children’s health-risk behavior. J Spec Pediatr Nurse. 2006;11:41–52. doi: 10.1111/j.1744-6155.2006.00042.x. [DOI] [PubMed] [Google Scholar]
- 23.Jackson C, Dickinson DM. Developing parenting programs to prevent child health risk behaviors: A practice model. Health Educ Res. 2009;24:1029–42. doi: 10.1093/her/cyp039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Turrissi R, HIllhouse J, Heavin S, et al. Examination of the short-term efficacy of a parent-based intervention to prevent skin cancer. J Behav Med. 2004;27:393–412. doi: 10.1023/b:jobm.0000042412.53765.06. [DOI] [PubMed] [Google Scholar]
- 25.Boyatzis R. Transforming qualitative information: thematic analysis and code development. Thousand Oaks (CA): Sage; 1998. [Google Scholar]
- 26.Lazovich D, Forster J, Sorensen G, et al. Characteristics associated with use or intention to use indoor tanning among adolescents. Arch Pediatr Adolesc Med. 2004;158:918–24. doi: 10.1001/archpedi.158.9.918. [DOI] [PubMed] [Google Scholar]
- 27.Cokkinides V, Weinstock M, Lazovich D, et al. Indoor tanning use among adolescents in the US, 1998 to 2004. Cancer. 2009;115:190–8. doi: 10.1002/cncr.24010. [DOI] [PubMed] [Google Scholar]
- 28.Pierce JP, Choi WS, Gilpin EA, et al. Validation of susceptibility as a predictor of which adolescents take up smoking in the United States. Health Psychol. 1996;15:355–61. doi: 10.1037//0278-6133.15.5.355. [DOI] [PubMed] [Google Scholar]
- 29.Muthen LK, Muthen BO. Mplus user’s guide. 5. Los Angeles: Muthen & Muthen; 2007. [Google Scholar]
- 30.Rideout VJ, Foehr UG, Roberts DF. Generation M2: Media in the lives of 8-to 18-year olds. Menlo Park (CA): Henry J. Kaiser Family Foundation; 2010. [Google Scholar]
- 31.Sayer LC, Bianchi SM, Robinson JP. Are parents investing less in children? Trends in mothers’ and fathers’ time with children. Am J Sociol. 2004;110:1–43. [Google Scholar]
- 32.Rogers RW, Prentice-Dunn S. Protection Motivation Theory. New York: Plenum Press; 1997. [Google Scholar]
- 33.Southwell BG, Yzer MC. When (and why) interpersonal talk matters for campaigns. Commun Theory. 2009;19:1–8. [Google Scholar]
- 34.Southwell BG, Slater JS, Rothman AJ, et al. The availability of community ties predicts likelihood of peer referral for mammography: Geographic constraints on viral marketing. Soc Sci Med. 2010;71:1627–35. doi: 10.1016/j.socscimed.2010.08.009. [DOI] [PubMed] [Google Scholar]
- 35.Krishna S, Boren SA, Balas EA. Healthcare via cell phones: A systematic review. Telemed J E Health. 2009;15:231–40. doi: 10.1089/tmj.2008.0099. [DOI] [PubMed] [Google Scholar]
- 36.Kharbanda EO, Stockwell MS, Fox HW, Rickert VI. Text4Health: A qualitative evaluation of parental readiness for text message immunization reminders. Am J Public Health. 2009;99:2176–8. doi: 10.2105/AJPH.2009.161364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211. [Google Scholar]
- 38.Freeman S, Francis S, Lundahl K, et al. UV tanning advertisements in high school newspapers. Arch Dermatol. 2006;142:460–2. doi: 10.1001/archderm.142.4.460. [DOI] [PubMed] [Google Scholar]
- 39.Lazovich D, Forster J. Indoor tanning by adolescents: Prevalence, practices and policies. Eur J Cancer. 2005;41:20–7. doi: 10.1016/j.ejca.2004.09.015. [DOI] [PubMed] [Google Scholar]
- 40.Balk SJ. Ultraviolet radiation: A hazard to children and adolescents. Pediatrics. 2011;127:e791–817. doi: 10.1542/peds.2010-3502. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.