

Abstract
We compared erect penile length after inflatable penile prosthesis (IPP) implantation with that induced by in-tracavernosal injection (ICI) before surgery. A total of 11 patients with full erections induced by ICI of 0.25 mL of Trimix (papaverine, phentolamine and prostaglandin E1) at the time of penile color duplex Doppler ultrasonography were enrolled in this study. The patients subsequently underwent IPP implantation as the ultimate treatment for their erectile dysfunction (ED). Erect penile length consequent to IPP implantation was measured at 6 weeks, 6 months and at 1 year after surgery. The Sexual Health Inventory for Men (SHIM) was administered before, and at 6 months and 1 year after IPP implantation. Erect penile length (mean ± s.e.) as induced by ICI was 13.2 ± 0.4 cm, whereas the lengths attained with IPP were 12.4 ± 0.3, 12.5 ± 0.3 and 12.5 ± 0.4 cm at the sixth week, sixth month and 1-year follow-ups, respectively. There were 0.83 ± 0.25, 0.75 ± 0.20 and 0.74 ± 0.15 cm decreases in erect penile length at 6 weeks, 6 months and 1 year, respectively, after IPP implantation when compared with that after ICI (P < 0.05). The SHIM scores for patients reporting shorter penises were the same as those for patients without complaints at the 6-month and 1-year follow-ups (P > 0.05). To our knowledge, this is the first study to objectively show a significant decrease in erect penile length after IPP implantation when compared with that after ICI. However, this decrease did not affect the effectiveness of IPP in treating ED.
Keywords: erectile dysfunction, intracavernosal injection, length, penile prosthesis, radical prostatectomy
Introduction
Erectile dysfunction (ED) is a common disease. The recent population-based, longitudinal study revealed that the prevalence of ED was age dependent; from 2% for men aged 40–49 years to 39% for men aged ≥ 70 years 1. Age-adjusted risk of ED for men with risk factors, such as diabetes mellitus and post-prostatectomy, is even higher 2, 3. Currently, the treatment of ED, in order, includes phosphodiesterase type 5 inhibitors (PDE5-I), vacuum erectile devices, intraurethral pellet, intracavernosal injections (ICI) and penile prosthesis implantation. These have given physicians numerous options for successful treatment of ED in nearly all cases. Penile prosthesis has been shown to have excellent long-term patient satisfaction in those who failed non-surgical therapies 4, 5, 6. Satisfaction rate with inflatable penile prosthesis (IPP) was reported as 93%, much higher than other therapies 7. Despite this overall satisfaction, many patients complain of a reduction in their penile lengths subjectively 8. To date, there has been little data investigating this claim with only one study that compared the stretched flaccid penile length before and after the IPP 9. There is no publication to substantiate the decrease of erect penile length after the IPP implantation. This study was designed to compare erect penile length obtained by preoperative ICI with that provided by IPP implantation postoperatively. The sexual health inventory for men (SHIM) was also used to evaluate effectiveness of IPP in patients complaining of shorter penises to those without complaints.
Patients and methods
A total of 109 patients underwent penile color duplex Doppler studies and subsequently received IPP implantation by a single surgeon (RW) from August 2005 to December 2007. A total of 11 patients with full erections induced by ICI of 0.25 mL of Trimix (150 mg of papaverine, 50 μg of prostaglandin E1 and 5 mg of phentolamine in 5 mL solution) at the time of penile color duplex Doppler study were prospectively enrolled in the study. A full erection was defined by an angle of ≥ 90 degrees from the patient pubis. Once a full erection was achieved, it was measured from the pubic bone to the tip of the glans penis by a single examiner. All 11 patients underwent the insertion of three-piece IPP as the ultimate treatment choice for ED. Patients with Peyronie's disease were excluded from the study.
The three-piece IPP implantation was performed through a penile–scrotal incision under general or regional anesthesia, as previously described 10. The lengths of the implanted cylinders corresponded exactly to intracorporeal measurements. The measurements were repeated twice to avoid downsizing the cylinders.
At 6 weeks after surgery, all patients were instructed to inflate and deflate the IPP. At 6 weeks, 6 months and one year postoperatively, the erect penis was measured from the pubic bone to the tip of the glans penis after full inflation of IPP in the clinic.
The SHIM scores were obtained before surgery, at 6 months and at 1 year after penile prosthesis implantation. The patients were also asked to evaluate their erect penile length after full inflation of IPP by simple questionnaire (Is your erect penile length same, shorter or longer?).
The preoperative and postoperative erect penile lengths were compared using paired Wilcoxon-tests. The Wilcoxon-test was also used to compare the SHIM scores. All statistical analyses were processed through the Statistical Package for the Social Sciences (SPSS), version 13.0 for Windows. A P value < 0.05 was considered statistically significant.
Results
The patient's age (mean ± standard error [s.e.]) was 62 ± 1.9 years (range 50–73 years). All 11 patients had ED associated with nerve-sparing radical prostatectomy for localized prostate cancer treatment. In our cancer center, all patients were instructed to start penile rehabilitation 6 weeks after radical prostatectomy with patient-directed use of PDE5-I and daily use of a vacuum erectile device. For patients with no response to PDE5-I in 3 months, the ICI was offered. In this study, all patients had failed non-surgical treatment or were unwilling to use ICI therapy. The penile color duplex Doppler studies were performed to evaluate the etiology of ED. The interval between radical prostatectomy and the penile color duplex Doppler evaluation was from 2 to 4 years in this group of patients. The neurogenic etiology, possibly because of poor recovery of cavernosal nerve function after radical prostatectomy, was deemed as the cause of ED, as no vascular abnormality was identified and full erection was observed after ICI in all 11 patients.
The erect penile length (mean ± s.e.) induced by ICI at the time of penile color duplex Doppler studies in this cohort was 13.2 ± 0.4 cm. A total of 54.5% of patients received Mentor/Coloplast Titan prostheses and 45.5% of patients had AMS 700 CX prosthesis implantations. No surgical complications occurred in this cohort.
After IPP implantation, the mean erectile length was 12.4 ± 0.3 cm at the sixth week, 12.5 ± 0.3 cm at the sixth month and 12.5 ± 0.4 cm at the 1-year follow-ups, respectively (Figure 1). There were 0.83 ± 0.25 cm, 0.75 ± 0.20 cm and 0.74 ± 0.15 cm decreases of erect penile length at the sixth week, sixth month and 1-year measurements after IPP implantation when compared with that induced by ICI (P < 0.05). The measurements of penile length at 6 weeks, 6 months and 1 year were not statistically different (P > 0.05). No difference in change of erect penile length was found between patients who received the Mentor/Coloplast Titan prostheses and those who had AMS 700 CX prosthesis implantations. All (100%) patients had an objective (measurable) decrease of erect penile length (from 0.2 to 3.0 cm) after IPP. However, only 45.5% of patients reported subjective penile shortening after IPP. A total of 54.5% patients reported no difference regarding the erect penile length obtained by ICI and IPP. No patients believed that their erect penile lengths were longer after IPP implantation.
Figure 1.
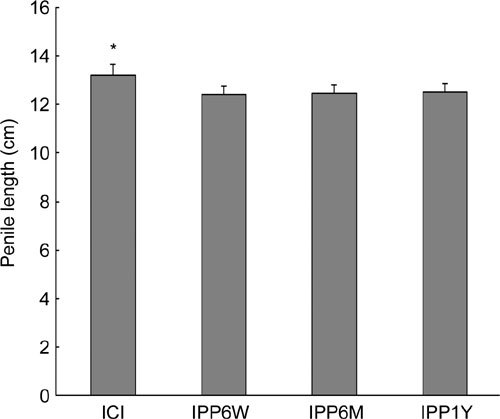
Erect penile length induced by ICI and after IPP. ICI: intracavernosal injection; IPP: inflatable penile prosthesis; W: week ; M: month; Y: year. *P < 0.05 .
The SHIM scores (mean ± s.e.) in patients complaining of shorter penises were the same as that in patients without complaints (23.0 ± 0.7 vs. 23.2 ± 0.8 at the 6-month follow-up and 23.7 ± 0.7 vs. 23.6 ± 0.9 at the 1-year follow-up, P > 0.05, Figure 2).
Figure 2.
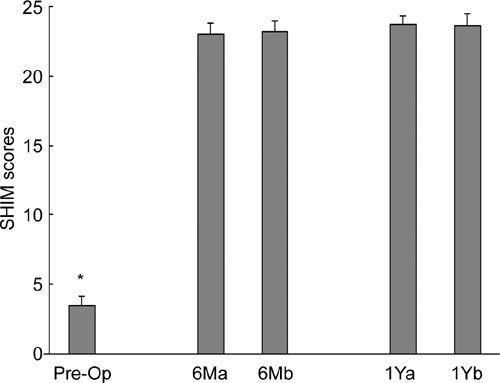
SHIM scores in patients reporting penile shortening vs. no penile shortening. 6Ma: 6 month, reporting penile shortening 6Mb: 6 month, reporting no penile shortening; 1Ya: 1 year, reporting penile shortening; 1Yb: 1 year, reporting no penile shortening. *P < 0.01 before and after IPP
Discussion
Evaluation for patients' claim of the loss of penile length after IPP is difficult because they were unable to obtain an erection for many years before the penile implantation. Wessell et al. 11 reported that, although stretched penile length closely correlated with erect length, there was an average discrepancy of 0.5 cm between the two. Deveci et al. 9 compared the stretched flaccid penile length before and after the IPP and found that penile prosthesis did not have a negative impact on the measurement of stretched flaccid penile length even though 72% of patients reported a decrease of penile length in the study. However, erect penile length (not stretched flaccid length) is the true concern for the patients. We believe that erection induced by ICI while doing the penile Doppler study will give physicians and patients opportunities to objectively and subjectively evaluate the erect penile length before surgery. In our study, we found statistically significant decreases in erect penile length at 6 weeks, 6 months and at 1 year after IPP, and this difference was noticeable in 45% of patients. Loss of erect penile length was not associated with a particular IPP. We did not include the patients with Peyronie's disease in this study because the healing and the ultimate results after IPP implantation in these patients can sometimes be unpredictable owing to the increased risk of fibrosis and scar tissue formation.
The mechanism of penile shortening after IPP is not clearly understood. Decreased penile length can be caused by inaccurate measurement of corporeal length during the surgery. This surgical technique error will generally cause a SST (supersonic transportation)-like deformity. In our implantation surgeries, the measurements were repeated twice to avoid downsizing the cylinders and no SST deformity was observed in the follow-ups. Obviously, decreased penile length cannot be explained by inaccurate measurement. This loss of erect penile length maybe associated with the lack of engorgement of the glans penis after prosthesis placement, which has been a common complaint from the patients after penile prosthesis placement. Several groups have looked at therapeutic options for a soft glans penis after penile prosthesis implantation. Benevides et al. 12 used an intraurethral alprostadil, and found that 10 of 17 men with prosthesis reported better penile engorgement and/or sensation. Other groups have looked at oral sildenafil therapy in patients with inflatable prosthesis. Mulhall et al. 13 studied sildenafil effect in patients with penile prosthesis and found that all had subjective improvement in glans engorgement, and there was improvement in overall sexual satisfaction as measured by the International Index of Erectile Function (IIEF) questionnaire. Lledo et al. 14 found that 12 of 13 patients with inflatable prostheses had improved sexual satisfaction measured by the IIEF questionnaire when given sildenafil orally. We do not know whether our patients will get a longer penile measurement with the use of PDE5-I or intraurethral alprostadil.
To prevent penile shortening, some groups even go as far as advocating concomitant surgical intervention. Borges et al. 15 reported 93% satisfaction with IPP performance and penile length, and a willingness to undergo the surgery again when all patients in their study had their suspensory ligament released at the same time of IPP placement. Miranda et al. 16 performed scrotal plastic surgery to remove the penoscrotal web as a way to enhance patient's subjective penile length. In their study, 84% (36 of 43) of patients reported some degree of increase in their perception of phallic length. However, these studies were not designed to objectively compare the loss and the improvement of erect penile length before and after the surgeries.
Radical prostatectomy is a common etiology for ED, and some patients with ED after radical prostatectomy will eventually need IPP. Several studies have found the stretched penile length to be decreased after radical prostatectomy. Savoie et al. 17 found that 68% of patients had a decrease in their stretched penile length ranging from 0.5 cm to 5.0 cm. Munding et al. 18 found a decreased stretched penile length in 71% of patients. It is believed that a combination of nerve damage (even in the most meticulous nerve-sparing dissection some degree of nerve damage is unavoidable because of the close proximity of the nerves to the prostate gland) with decreased arterial inflow (associated with the ligation of accessory internal pudendal arteries during prostatectomy) may ultimately lead to apoptosis, which has recently been linked to the pathophysiology of post-prostatectomy ED and penile shrinkage 3. With the possible loss of penile length after radical prostatectomy, it is imperative that we discuss with patients the possibility of further reduction in erectile length with the placement of IPP.
Patient satisfaction after penile prosthesis implantation is a complex issue. Penile shortening may affect patients' overall satisfaction 9. Unfortunately, to date there is no validated instrument specific for evaluation of post-implantation satisfaction. Available instruments are either custom made inventories (not validated) or validated questionnaires designed for other reasons (not specific). Our study showed that even though about 45% of patients reported subjective penile shortening with IPP, they had the same satisfaction compared with the patients without subjective penile shortening when a non-specific validated sexual function questionnaire was used to evaluate patient erectile function and satisfaction. Therefore, a non-specific validated sexual function questionnaire may not accurately reflect patient overall satisfaction after IPP. It is necessary to develop an IPP-specific validated satisfaction questionnaire in the future. In addition, a multi-center study is ongoing in the United States to evaluate the penile rehabilitation after IPP to enhance erect penile length and the results will be available in less than a year.
Conclusion
To our knowledge, this is the first study that objectively compared erect penile length with ICI with that of the IPP. We found a significant decrease in erect penile length in our study population. It is important to educate patients and their partners about this possibility before surgery to limit any unrealistic expectations after implantation.
References
- Inman BA, Sauver JL, Jacobson DJ, McGree ME, Nehra A, et al. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009;84:108–13. doi: 10.4065/84.2.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore CR, Wang R. Pathophysiology and treatment of diabetic erectile dysfunction. Asian J Androl. 2006;8:675–84. doi: 10.1111/j.1745-7262.2006.00223.x. [DOI] [PubMed] [Google Scholar]
- Wang R. Penile rehabilitation after radical prostatectomy: where do we stand and where are we going. J Sex Med. 2007;4:1085–97. doi: 10.1111/j.1743-6109.2007.00482.x. [DOI] [PubMed] [Google Scholar]
- Mulhall JP, Ahmed A, Branch J, Parker M. Serial assessment of efficacy and satisfaction profiles following penile prosthesis surgery. J Urol. 2003;169:1429–33. doi: 10.1097/01.ju.0000056047.74268.9c. [DOI] [PubMed] [Google Scholar]
- Brinkman MJ, Henry GD, Wilson SK, Delk JR II, Denny GA, et al. A survey of patients with inflatable penile prosthesis for satisfaction. J Urol. 2005;174:253–7. doi: 10.1097/01.ju.0000161608.21337.8d. [DOI] [PubMed] [Google Scholar]
- Lewis RW. Long-term results of penile prosthetic implants. Urol Clin North Am. 1995;22:847–56. [PubMed] [Google Scholar]
- Rajpurkar A, Dhabuwala CB. Comparison of satisfaction rates and erectile function in patients treated with sildenafil, intracavernous prostaglandin E1 and penile implant surgery for erectile dysfunction in urology practice. J Urol. 2003;170:159–63. doi: 10.1097/01.ju.0000072524.82345.6d. [DOI] [PubMed] [Google Scholar]
- Olugbade OA, Parker M, Guhring P, Mulhall J. Determinants of patients satisfaction following penile prosthesis surgery. J Sex Med. 2006;3:743–8. doi: 10.1111/j.1743-6109.2006.00278.x. [DOI] [PubMed] [Google Scholar]
- Deveci S, Martin D, Parker M, Mulhall JP. Penile length alterations following penile prosthesis surgery. Eur Urol. 2007;51:1128–31. doi: 10.1016/j.eururo.2006.10.026. [DOI] [PubMed] [Google Scholar]
- Wang R, Lewis RW.Penile implants—types and current indicationsIn: Mulcahy JJ, editor. Current clinical urology: male sexual function: A guide to clinical management. Totowa, New Jersey: Humana Press Inc; 2000. p263–77.
- Wessells H, Lue TF, McAnnich JW. Penile length in the flaccid and erect states: guidelines for penile augmentation. J Urol. 1996;156:995–7. [PubMed] [Google Scholar]
- Benevides MD, Carson CC. Intraurethral application of alprostadil in patients with failed inflatable prosthesis. J Urol. 2000;163:785–7. [PubMed] [Google Scholar]
- Mulhall JP, Jahoda A, Aviv N, Valenzuela R, Parker M. The impact of sildenafil citrate on sexual satisfaction profiles in men with a penile prosthesis in situ. BJU Int. 2004;93:97–9. doi: 10.1111/j.1464-410x.2004.04564.x. [DOI] [PubMed] [Google Scholar]
- Lledo GE, Moncada II, Jara RJ, Carrera PC, Gonzales-Chamorro F, et al. Treatment with sildenafil of cold glans syndrome after inflatable penile prosthesis. Actas Urol Esp. 2004;28:443–6. doi: 10.1016/s0210-4806(04)73107-1. [DOI] [PubMed] [Google Scholar]
- Borges F, Hakim L, Kline C. Surgical technique to maintain penile length after insertion of an inflatable prosthesis via infrapubic approach. J Sex Med. 2006;3:550–3. doi: 10.1111/j.1743-6109.2006.00232.x. [DOI] [PubMed] [Google Scholar]
- Miranda-Sousa A, Keating M, Moreira S, Baker M, Carrion R. Concomitant ventral phalloplasty during penile implant surgery: a novel procedure that optimize patient satisfaction and their perception of phallic length after penile implant surgery. J Sex Med. 2007;4:1494–9. doi: 10.1111/j.1743-6109.2007.00551.x. [DOI] [PubMed] [Google Scholar]
- Savoie M, Kim SS, Soloway MS. A prospective study measuring penile length in men treated with radical prostatectomy for prostate cancer. J Urol. 2003;169:1462–4. doi: 10.1097/01.ju.0000053720.93303.33. [DOI] [PubMed] [Google Scholar]
- Munding MD, Wessells HB, Dalkin BL. Pilot study of changes in stretched penile length 3 months after radical retropubic prostatectomy. Urology. 2001;58:567–9. doi: 10.1016/s0090-4295(01)01270-5. [DOI] [PubMed] [Google Scholar]