

Abstract
Ellis-van Creveld (EvC) syndrome or chondroectodermal dysplasia is an autosomal recessive disorder with characteristic clinical manifestations. The four principal characteristics are chondrodysplasia, polydactyly, ectodermal dysplasia and congenital heart defects. Its incidence in the general population is low. The oral manifestations of EvC syndrome include both soft tissues and teeth, but the dental literature on the subject is scarce. The present case describes the constant and variable oral findings in these patients, which can be diagnosed at any age, even during pregnancy. The presence of a variety of oral manifestations, such as fusion of upper lip to the gingival margin, presence of multiple frenula, abnormally shaped and microdontic teeth and congenitally missing teeth requires multidisciplinary dental treatment, with consideration for the high incidence of cardiac defects in these patients.
Background
Ellis-van Creveld (EvC) syndrome is an autosomal recessive chondroectodermal dysplasia, described by Richard Ellis and Simon van Creveld in 1940.1 It is a generalised dysplasia of endochondral ossification, caused by mutations in a novel gene on chromosome 4p16, with high prevalence in Amish community of Lancaster.2 There is parental consanguinity in 30% of the cases with 7/1 000 000 prevalence outside Amish community. Today, the syndrome has been described in other populations and it is known to affect all races.3
EvC presents a characteristic tetrad4:
Disproportionate dwarfism due to chondrodysplsia of the long bones and an exceptionally long trunk. The severity of short limbs increases from the proximal to the distal portions.
Bilateral postaxial polydactyly of the hands, with the supernumerary finger usually being on the ulnar side. Occasionally a supernumerary toe may be present.
Ectodermal dysplasia with dystrophic, small nails, thin sparse hair and hypodontic and abnormally formed teeth.
Congenital heart malformations in 50–60% of the cases. The most common being a single atrium and a ventricular septal defect.
Other skeletal anomalies such as genu valgam (knock knees) have been occasionally reported. Patients’ intelligence is usually normal.5 Oral manifestations in EvC syndrome are remarkable and constant. The most common finding is a fusion of the anterior portion of the upper lip to the maxillary gingival margin, so that no mucobuccal fold exists, causing the upper lip to present a slight V-notch in the middle.1 The anterior portion of the lower alveolar ridge is often serrated and multiple small and conical molars have abnormal cusps or accessory grooves,1 and sometimes hypoplastic enamel is seen. Congenitally missing primary and permanent teeth, dysmorphic conical-shaped roots and delay in eruption have also been reported.6 Malocclusions occur secondary to these oral abnormalities as they are of no specific type.7
Cardiac defects present in some patients with EvC and require antibiotic coverage for the prevention of infectious endodcarditis.4 Almost half of these patients die during childhood because of cardiopulmonary complications; for this reason the life expectancy of EvC patients is determined by their congenital cardiac disease.5
Case presentation
A 13-year-old girl reported to our out patient department with missing lower front teeth and abnormally shaped teeth in the mouth. The history as reported by the parents revealed that the teeth had never erupted and presence of natal teeth which were extracted. Family history was positive with her parents being the first cousins suggestive of consanguineous marriage, the child's aunt and brother being affected by the same condition indicated a recessive pattern running in the family. On examination the patient was healthy, with very short stature measuring 4 feet (figure 1), normal facial and trunk development but small distal extremities especially fingers and toes (figure 2). She had bilateral ulnar polydactyly and dystrophic nails (figure 3).
Figure 1.

The general features of the child.
Figure 2.

The small distal extremities.
Figure 3.

The ulnar polydactaly.
On intraoral examination the teeth were small, peg shaped and hypoplastic; the palate was high arched, the sulcus between upper lip and gum was obliterated while the short upper lip was bound down by multiple frenula along with presence of bilateral bony clefts (figure 4). Agenesis of lower incisors was noted with bilateral crossbite with upper first molars (figures 5 and 6). Teeth were microdontic and conical, molars had abnormal cusps and accessory grooves (figure 7). Hair and skin were normal and she had normal sweating. Systemic examination revealed all the systems to be normal. A clinical diagnosis of EvC syndrome was made.
Figure 4.

Multiple frenula along with presence of bilateral bony clefts and malformed teeth.
Figure 5.

Serrated lower anterior region with missing permanent incisors.
Figure 6.

Malocclusion.
Figure 7.

Microdontia with abnormal accessory cusps on molars.
Investigations
Panoramic radiograph revealed congenital absence of lower incisors, upper lateral incisors with impacted primary lower incisor (figure 8). Hand wrist radiograph showed short middle and terminal phalanges, ulnar polydactyly (figure 9). These findings supported our clinical diagnosis.
Figure 8.

Panoramic radiograph showing partial anodontia with impacted primary lower incisor.
Figure 9.
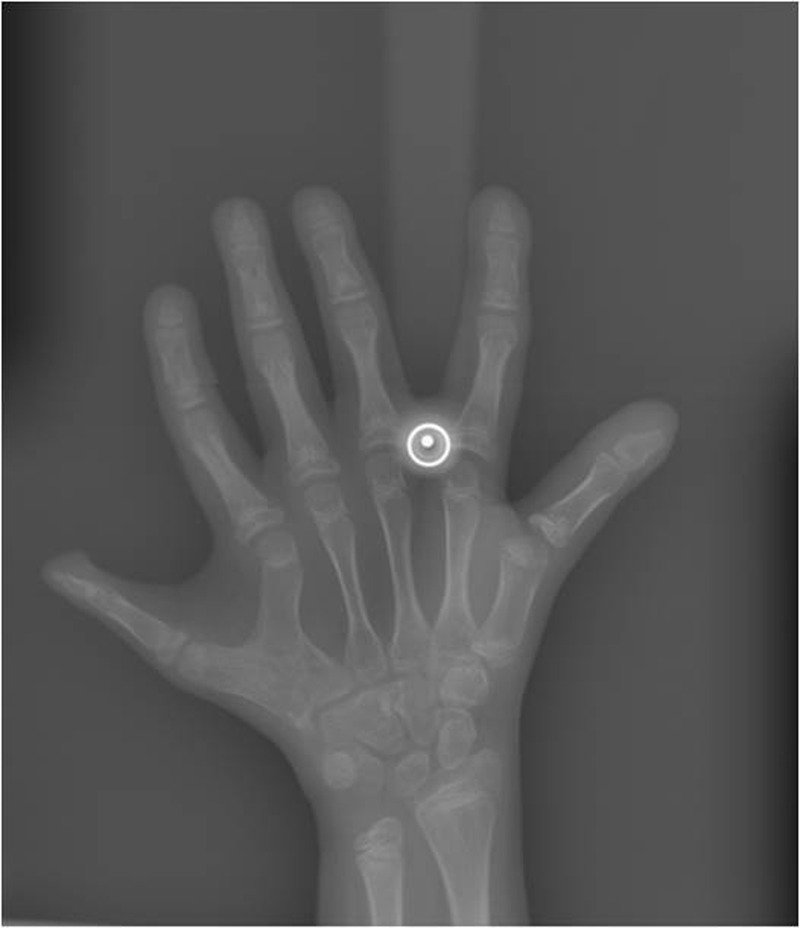
Hand wrist radiograph illustrating postaxial polydactyly.
Thorough review of cardiac, respiratory and reproductive systems was carried out and no abnormality was detected.
Differential diagnosis
Ectodermal dysplasia, Orofaciodigital syndrome, Jeune syndrome.
Discussion
EvC syndrome is a skeletal dysplasia, first described by Richard Ellis and Simon Van Creveld who coined the term ‘Chondroectodermal dysplasia’. It is genetic disorder with autosomal recessive transmission most often described in families with history of consanguinity. The EvC gene has been mapped to short arm of the chromosome 4 with five different mutations. The parents are of normal stature and both are carriers of the mutation. There is 25% chance of further pregnancies resulting in a child with the same condition.8 The syndrome can be diagnosed during the prenatal period, starting from the 18th week of gestation, by ultrasonography, or later by clinical examination after birth.9
The syndrome is a tetrad with chondrodysplasia, polydactyly, ectodermal involvement and congenital heart defects. Chondrodystrophy means disproportionate dwarfism, that is, normal trunk with symmetrical shortening of distal extremities (average adult height being 109–155 cm). Patients also have lumbar lordosis and genu valgum. Polydactyly is a constant finding, usually bilateral and on the ulnar side. It is observed in the hands in most cases but in the feet in only 10% of the cases. Ectodermal dysplasia (observed in up to 93%) includes sausage-shaped fingers hypoplastic dystrophic, friable or even absent nails. The cognitive and motor developments of patients affected by EvC syndrome are normal.8
Oral manifestations are diverse and involve not only soft tissues but also the number, shape and structure of the teeth. The percentage of these manifestations are reflected, the most important being fusion of upper lip to the gingival margin, presence of multiple frenula, conical, microdontic teeth, molars with wide grooves and atypical cusps, congenital missing teeth, malocclusion presence of supernumerary, natal and neonatal teeth.4 6 In this case all the findings were present in agreement with the previous reports. Congenital heart malformations are described in 50–60% of patients affected by this syndrome. Defects of mitral and tricuspid valves, patent ductusarteriosus and ventricular septal defects are some of the malformations described as the principal cause for decreased life expectancy in these patients. Other anomalies which may be present include musculoskeletal anomalies, that is, low set shoulders, a narrow thorax frequently leading to respiratory difficulties.10 In our case the patient had all the tetrad features. Cardiac anomalies were absent. Hair and sweating are usually normal. However, additional clinical findings affecting other organs lungs, liver, kidneys, pancreas and central nervous system may occasionally be observed, although these were not diagnosed in our case. Genitourinary anomalies such as agenesis and renal dysplasia, uretectasia and nephrocalcinosis usually present in 20% of cases. Other infrequent features include strabismus, epi- and hypospasdias. Exceptionally, haematological anomalies have been reported.9
Learning points.
Ellis-van Creveld syndrome requires multidisciplinary therapeutic planning.
The pedodontist plays a fundamental role in diagnosis and prevention of caries by taking proper preventive care such as dietary counselling, plaque control, oral hygiene instructions and application of fluoride and prescribing daily fluoride mouth rinses.
Aesthetic rehabilitation of abnormally shaped anterior teeth along with replacement of missing teeth with use of anterior acrylic partial dentures to maintain space and improve mastication, aesthetics and speech.
Patient requires orthodontic treatment for correction of malocclusion and surgical treatment for correction of any skeletal deformities.
Dental treatment should be done under antibiotic prophylactic coverage due to high incidence of cardiac pathology in these patients.
Footnotes
Contributors: All authors have made substantive contribution to this manuscript, and all have reviewed the final paper prior to its submission.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Atasu M, Biren S. Ellis-van Creveld syndrome: dental, clinical, genetic and dermatoglyphic findings of a case. J Clin Pediatr Dent 2000;2013:141–5 [PubMed] [Google Scholar]
- 2.Sergi C, Voigtlander T, Zoubaa S, et al. Ellis-van Creveld syndrome: a generalized dysplasia of endochondral ossification. Pediatr Radiol 2001;2013:289–93 [DOI] [PubMed] [Google Scholar]
- 3.Polymeropoulos MH, Ide SE, Wright M, et al. The gene for the Ellis-van Creveld syndrome is located on chromosome 4p16. Genomics 1996;2013:1–5 [DOI] [PubMed] [Google Scholar]
- 4.Hattab FN, Yassin OM, Sasa IS. Oral manifestations of Ellis-van Creveld syndrome: report of 2 siblings with unusual dental anomalies. J Clin Pediatr Dent 1998;2013:159–65 [PubMed] [Google Scholar]
- 5.Ortega J, Ferrer J, Fernandez A, et al. The Ellis-van Creveld syndrome: apropos a clinical case. An Esp Pediatr 1999;2013:74–6 [PubMed] [Google Scholar]
- 6.Himelhoch DA, Mostofi R. Oral abnormalities in the Ellis-van Creveld syndrome: case report. Pediatr Dent 1988;10:309–13 [PubMed] [Google Scholar]
- 7.Varela M, Ramos C. Chondroectodermal dysplasia (Ellis–van Creveld syndrome): a case report. Eur J Orthod 1996;2013:313–18 [DOI] [PubMed] [Google Scholar]
- 8.Khan I, Ahmed SA, Mohsin K. Ellis van Creveld syndrome. A case report. J Pak Assoc Dermatol 2006;2013:239–42 [Google Scholar]
- 9.Baujat G, Le Merrer M. Ellis-van Creveld syndrome. Orphanet J Rare Dis 2007;2013:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Arya L, Mendriratta V, Sharma RC, et al. Ellis-van Creveld syndrome: a report of two cases. Pediatr Dermatol 2001;2013:485–9 [DOI] [PubMed] [Google Scholar]