

Abstract
The present study examined smoking-specific and general parenting predictors of in vivo observed patterns of parent–adolescent discussion concerning adolescents’ cigarette smoking experiences and associations between these observed patterns and 24-month longitudinal trajectories of teen cigarette smoking behavior (nonsmokers, current experimenters, escalators). Parental solicitation, adolescent disclosure, and adolescent information management were coded from direct observations of 528 video-recorded parent–adolescent discussions about cigarette smoking with 344 teens (M age = 15.62 years) with a history of smoking experimentation (321 interactions with mothers, 207 interactions with fathers). Adolescent initiation of discussions concerning their own smoking behavior (21% of interactions) was predicted by lower levels of maternal observed disapproval of cigarette smoking and fewer teen-reported communication problems with mothers. Maternal initiation in discussions (35% of interactions) was associated with higher levels of family rules about illicit substance use. Three categories of adolescent information management (full disclosure, active secrecy, incomplete strategies) were coded by matching adolescents’ confidential self-reported smoking status with their observed spontaneous disclosures and responses to parental solicitations. Fully disclosing teens reported higher quality communication with their mothers (more open, less problematic). Teens engaged in active secrecy with their mothers when families had high levels of parental rules about illicit substance use and when mothers expressed lower levels of expectancies that their teen would smoke in the future. Adolescents were more likely to escalate their smoking over 2 years if their parents initiated the discussion of adolescent smoking behavior (solicited) and if adolescents engaged in active secrecy.
Keywords: adolescent–parent communication, disclosure, secrecy, cigarette smoking, observational research
Parental knowledge of their adolescents’ whereabouts and activities has been consistently linked with reduced adolescent problem behavior (Barber, Stolz, & Olsen, 2005). Recent research suggests that “adolescent-initiated” processes such as teen disclosure better predict parental knowledge than “parent-initiated” processes such as parental solicitation (Kerr, Stattin, & Burk, 2010). However, for personal (developing autonomy) or practical (avoid parental sanctions) reasons, adolescents may desire to keep some information secret from parents, particularly their engagement in problem or health-risk behaviors (Smetana, Villalobos, Tasopoulos-Chan, Gettman, & Campione-Barr, 2009). Thus, adolescents often engage in information management strategies (Marshall, Tilton-Weaver, & Bosdet, 2005). Disclosure and information management strategies are associated with parenting behaviors (Smetana et al., 2009) and have been linked to subsequent delinquent behavior (Frijns, Keijsers, Branje, & Meeus, 2010), but previous research in this area has primarily used self-report measures and collapsed across disparate teen activities. Such general knowledge is indisputably important, but it may be equally critical for parents to learn about adolescents’ delinquent or health-risk behavior. In the present study, we used observed parent–teen conversations to assess in vivo patterns of parent solicitation, adolescent disclosure, and information management concerning teen cigarette smoking. The study had two related goals: (a) examine associations between general and smoking-specific parenting behaviors and observed parent–adolescent communication patterns and (b) explore whether observed communication patterns predicted longitudinal trajectories of adolescent smoking behavior.
Adolescent Cigarette Smoking: Disclosure, Information Management, and Developmental Patterns
A great deal of research has investigated parenting behavior and family processes related to adolescent cigarette smoking. This literature has distinguished “smoking-specific socialization” behaviors, such as smoking communication (e.g., antismoking messages) and smoking rules, from general parenting behaviors, such as those associated with authoritative parenting (Chassin et al., 2005; Harakeh, Scholte, Vermulet, de Vries, & Engels, 2010). Research has consistently found that parents’ smoking-specific behaviors are associated with reduced levels of adolescent cigarette smoking over and above general parenting behaviors. Similarly, parental solicitation and adolescent disclosure (or concealment) about smoking may be more clearly linked with subsequent teen smoking than general disclosure processes.
Cigarette smoking is also a significant behavioral outcome to consider when investigating adolescent disclosure and secrecy from a developmental perspective. Smoking poses both short- and long-term health risks to adolescents, and the majority of adults who smoke began smoking in adolescence (U.S. Department of Health and Human Services, 1994). However, not all adolescents who experiment with cigarettes become regular adult smokers (Chassin, Presson, Sherman, & Edwards, 1990). For many youth, cigarette smoking represents an “adolescent-limited” risk-taking behavior that will not persist into adulthood (Moffitt, 1993). Thus, adolescent smoking experimenters are represented by different developmental trajectories, including teens who will escalate into adult-level smokers and those who will maintain low levels of experimentation. Both general and smoking-specific parenting and family processes have been found to distinguish temporary experimenters from persistent escalators (Darling & Cumsille, 2003). We build on this research in the present study by exploring whether smoking-specific parental solicitation and adolescent disclosure and information management predict longitudinal smoking trajectories.
Observed Parent–Adolescent Communication
Previous research on adolescent disclosure and information management has relied on self-report measures. However, by definition, disclosure occurs within parent–adolescent discussions, and paper-and-pencil measures may be relatively uninformative about the conversational context in which such disclosures are embedded. In contrast, standardized observation methods are designed to generate a nuanced characterization of the bidirectional nature of family communication processes. Questionnaire instruments are invaluable tools for providing historical and subjective reports of behavior, but they are susceptible to social desirability biases and can only tap into constructs identified a priori, which constrains discovery of salient behaviors not yet recognized (Rutter, 1997). Little is known about how adolescents disclose or manage information during actual discussions. Direct observation methods may provide objective, complementary data concerning how these communication processes function within live interactions or what they “look like.” Additionally, adolescent disclosure is conceptualized as spontaneous communication that is not preceded by parental solicitation (Stattin & Kerr, 2000). Thus, the order of parent–adolescent dialogue (whether parents solicit or teens disclose first) is a potentially vital component of communication related to parental knowledge. Observing parent–adolescent dyadic conversations allows for an objective measure of this temporal sequence and permits tests of whether family and individual variables distinguish families in which parents solicit or adolescents spontaneously disclose.
Observational methods may be especially useful for characterizing individual differences in parent–teen discussion of adolescents’ problem or health-risk behavior. On self-report measures, adolescents report on parental solicitation and their own management strategies “on average.” Parents and adolescents may frequently discuss everyday activities such as academic or after-school activities, but discussions about teens’ engagement in specific problem behaviors are likely less common. In addition, adolescents who do not engage in specific health risk behaviors (e.g., cigarette smoking) have nothing to disclose or conceal, so disclosure and behavior are often confounded in self-report measures. Traditional observation methods require parents and adolescents to engage in general discussions (argument tasks, etc.), but a structured interaction task “presses” for discussions on topics of interest such as health risk behavior (Boone & Lefkowitz, 2007). A structured observation paradigm may more directly tap into the ways in which parents try to gain information about their teens’ health risk through solicitation, as well as when (or whether) adolescents disclose information or engage in information management strategies.
Adolescent Information Management Strategies
Teens know parents disapprove of health risk activities such as cigarette smoking, which influences whether or not they choose to disclose their behavior (Darling, Cumsille, Pena-Alamay, & Coatsworth, 2009). Findings regarding adolescents’ active role in facilitating parental knowledge has led to finer distinctions in adolescent disclosure and concealment. Disclosure and secrecy are only moderately inversely correlated, have different antecedents (Smetana, Metzger, Gettman, & Campione-Barr, 2006), and are distinctly associated with adolescent outcomes (Frijns et al., 2010). Disclosure and secrecy have been further disaggregated into information management strategies such as full disclosure, partial disclosure, lying (active secrecy), and avoiding (Cumsille, Darling, & Martinez, 2010). Full disclosure involves telling parents all important details. However, teens may try to keep some information secret by lying or making up a story, or partially disclosing by giving parents some information while leaving out essential details parents would want to know (Smetana et al., 2009). Other teens engage in avoidance by changing the subject or leaving before parents can ask questions (Mazur & Ebesu Hubbard, 2004).
Other research has questioned the incremental utility of distinguishing among types of secrecy. Using confirmatory factor analysis, Laird and Marrero (2010) found that categories of young adolescents’ (ages 11 and 12) information management could be modeled as two higher order latent factors: disclosing and concealing strategies. However, research has found that older adolescents’ choice and motivation for using different strategies varied for prudential behaviors (involving harm to self) (Smetana et al., 2009). Thus, key distinctions between concealment strategies may emerge within conversations about health risk behaviors such as cigarette smoking, which teens may be highly motivated to keep secret from parents.
Predictors of Adolescent Information Management Strategies
Research has examined individual and familial predictors of adolescent disclosure and information management. Girls disclose more and engage in secrecy less than boys (Keijsers, Branje, Frijns, Finkenauer, & Meeus, 2010), and teens disclose more to mothers than to fathers (Smetana et al., 2006). Disclosure also varies by ethnicity, with White youth disclosing more than Mexican or Chinese Americans (Yau, Tasopoulos-Chan, & Smetana, 2009).
Adolescent disclosure is positively associated with parenting dimensions, including warmth and responsiveness (Darling, Cumsille, Caldwell, & Dowdy, 2006). In contrast, secrecy is more common in low-quality parent relationships, and this link may be especially strong for adolescent girls (Keijsers et al., 2010) or in adolescents’ relationships with fathers (Smetana et al., 2009). Communication is an important component of high-quality parent–adolescent relationships (Barnes & Olson, 1985). Adolescents who view their communication with parents as open and unproblematic may be more comfortable initiating conversations and disclosing. Adolescent disclosure has also been associated with higher levels of familial rules (Darling et al., 2006). However, excessive or inappropriate forms of parental control may increase the use of concealment or secretive strategies (Tilton-Weaver et al., 2010), especially rules concerning issues adolescents view as personal (Smetana et al., 2009). Family rules vary by activity (Laird & Marrero, 2010), so adolescent discussion of their smoking behavior may be more closely aligned with substance use rules.
Teens may be more likely to discuss their smoking experiences with currently smoking parents, as an environment in which smoking-related communication is normative may increase adolescent disclosure. However, descriptive research indicates that the predominant parental message is that smoking is “bad” (Miller-Day, 2002). Adolescents may be reluctant to disclose to parents with strong negative attitudes toward smoking to avoid parental disapproval or punishment (Smetana et al., 2009). In contrast, teens may discuss their smoking behavior with parents who view smoking experimentation as normative and assume that teens (including their own teen) will try smoking. An observational methodology allows for the examination of in vivo patterns of parental smoking approval and disapproval to complement self-reports.
The Present Study
In the present study, we used a structured interaction task that directly “pressed” for discussion of smoking behavior to assess in vivo patterns of parent solicitation and adolescent information management about adolescents’ current and past smoking behavior. The present sample was enriched for adolescent smoking experimentation (all had smoked at least once in the past year, 1/2 had smoked in the past 30 days), reducing the confound between adolescent disclosure and behavior. Discussions concerning teens’ smoking behavior initiated by parents (parental solicitation) were distinguished from those initiated by teens (spontaneous disclosure or concealment). Teens were grouped into information management strategy categories (full disclosure, lying, etc.) by comparing their observed statements and self-reported smoking status. A majority of adolescents participated with two parents, allowing for an investigation of these processes in interactions with mothers and fathers. The goals of the study were twofold. The first goal was to examine general and smoking-specific parenting correlates of observed parental solicitation, adolescent disclosure, and adolescent information management concerning adolescents’ smoking behavior. It was hypothesized that parental solicitation would be associated with parental illicit substance rules and antismoking messages, whereas teens would initiate such exchanges to warm and open parents. Full disclosure was expected to increase when parents were currently smoking, warm, open, and spoke about smoking experimentation as being normative. Increased substance rules and parental smoking disapproval was hypothesized to increase adolescents’ use of concealment strategies. Disclosure was also hypothesized to be more common among females, Caucasian rather than African American or Hispanic youth, and in interactions with mothers. The second goal was to examine associations between adolescent longitudinal smoking trajectories and observed patterns of parental solicitation, adolescent disclosure, and adolescent information management. It was hypothesized that adolescents who initiated discussions and fully disclosed their own smoking behavior would be less likely to escalate their smoking behavior, whereas adolescents who engaged in concealing strategies would be more likely to escalate.
Method
Participants
Data for the present study come from an observational substudy (Family Talk about Smoking; FTAS; Wakschlag et al., 2011) embedded in a larger investigation of socioemotional influences on adolescent cigarette smoking. Adolescents in the larger study were recruited through a screening survey administered to ninth- and 10th graders at 16 schools, which oversampled for smoking (83% had some smoking experience; for a description of the full cohort and subsample, see Wakschlag et al., 2011). The FTAS subsample was composed of 348 adolescents, who had at least tried smoking at some point prior to their enrollment in the study. Participants were, on average, 15.61 years old (SD = 0.63, range = 13.9–17.5), and 58% were girls. Teens completed questionnaires and participated in structured dyadic communication tasks with their parents (both mothers and fathers when possible). Fifty-five percent of teens participated with two parents (n = 191) and 45% with one parent (n = 157). Three teens participated with two female caregivers (e.g., mother and grandmother), and interactions with mothers were used for these adolescents. Most (81%) of the teens who participated with one parent did so with their mothers (n = 127), 14% (n = 22) participated with their fathers, and the remaining 5% (n = 8) participated with another relative (for simplicity, we refer to female caregivers as mothers and male caregivers as fathers). Due to technical difficulties, four participants did not have usable video data. Thus, the analytic sample is 344 teens and their parents (528 video-recorded conversation segments: 321 with mothers and 207 with fathers).
The sample was demographically diverse. The majority of adolescents were non-Hispanic White (56%), African American (20%), or Hispanic (15%). Most parents were married (76%) and had some post-high school education (77%). Close to half (48%) of parents had a history of regular smoking.
Procedure
Assessment overview
Teens and parents completed baseline questionnaires prior to the Family Talk discussion visit. Teens and parents received $20 for completing the questionnaire assessments and $50 for the home visit (with a $50 family bonus when both available parents participated).
Questionnaire Measures
Teen and parent smoking
Self-described teen smoking status
Adolescents were asked, “Which of the following best describes how you think of yourself?” and instructed to choose from the following categories: smoker, social smoker/occasional smoker, ex-smoker, someone who tried smoking, nonsmoker. Smokers and social/occasional smokers were grouped into a “current experimenters” category (n = 75, 21.8%).
Teen smoking behavior
Teens reported the number of days smoked in the past 30 days; 44% reported smoking on at least one day. Teens smoked an average of 3.69 days (out of the last 30).
Parental smoking status
Parents were asked, “Do you currently smoke cigarettes on a regular basis (at least 1×/week)?” and were classified as current smokers (mothers = 23%, fathers = 26%) versus none and former smokers. Of the 10% of parents missing this data, all but two were available by teen report.
General parenting behaviors
Quality communication
Teens completed the Parent-Adolescent Communication Scale (Barnes & Olson, 1985) for both parents. Ten items assessed open (e.g., “My mom/dad is always a good listener”) and 10 items assessed problematic communication (e.g., “I have trouble believing everything my mom/dad tells me”) on a 5-point scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). Items were summed and higher scores indicated more openness and problems, respectively; alphas, open: mothers = .91, fathers = .91; problematic: mothers = 71, fathers = .70. The open and problematic scales were significantly though moderately negatively correlated (mothers: r = −.37, p < .001; fathers: r = −.38, p < .001).
Parental warmth
Parental warmth was measured with seven items (Ge, Conger, Lorenz, & Simmons, 1994), assessing parents’ expression of interest in and understanding of their teen (e.g., “How often does your Mom/Dad let you know that he/she appreciates you?”). Adolescents rated each parent, separately, on a 4-point scale ranging from 1 (never) to 4 (always); alphas: Mother scale = .93, Father scale = .94.
Smoking-specific parenting behaviors
Family rules about substance use
Adolescents rated the level of familial rules about 10 hypothetical behaviors from the Parental Restrictive Control Questionnaire (Smetana, 1988) on a 5-point scale ranging from 1 (No rules or expectations) to 5 (Firm rules or expectations). Principal axis factor analysis with oblimin rotation established three factors: Personal Behavior, Intimacy/dating, and Substance Use. Mean scores from the Substance Use subscale (three items, e.g., “whether I can smoke cigarettes/alcohol”, α = .75) were used in the present study, with higher scores indicating firmer rules.
Smoking-specific messages
Frequency of parental smoking messages was measured with seven items (Kodl & Mermelstein, 2004). Adolescents rated the frequency of parental antismoking statements (e.g., “smoking can give you cancer”) on a 3-point scale ranging from 1 (never) to 3 (several times). Items were averaged, and higher scores indicated a greater frequency of antismoking messages (α = .83).
Longitudinal smoking trajectories
Time line follow-back interviews were used to develop a continuous calendar of each adolescent’s smoking behavior from 6 months prior to initial assessment through a 24-month follow-up. Every 6 months, adolescents participated in structured interviews in which they comprehensively reported their smoking experiences over the previous 6 months and how much they smoked on each of the days that they smoked. Adolescents were prompted to recall specific life events (e.g., birthdays, school functions, vacations, etc.) to help anchor their recall. Growth mixture models in Mplus 4.21 were run to identify the form and the number of latent trajectory classes based on this information. Participants who reported not smoking over the full assessment period were considered as having a nonsmoking trajectory and were not included in the trajectory analysis. Random intercepts and nonlinear trends across time (linear and quadratic) were examined for all other participants who reported smoking at least once during the study period. A four-class solution resulted, including two classes of infrequent, nonescalating smokers, and two classes of escalating smokers. Intercepts were ordered by class, and Class 4 had the highest intercept. Class 4 escalated more rapidly than Class 3, starting at smoking 13.42 days/month (initial assessment) and increasing rapidly to 22.06 days/month at 24 months. Class 3 displayed slower escalation from Time 1 to 15 months (3.77 days/month to 6.60 days/month) and then rapid escalation from 15 months to 24 months (6.60 days/month to 9.53 days/month). Classes 1 and 2 displayed parallel, nonescalating trends; Class 2 started at smoking 2.01 days/month (initial assessment) and ended at 2.25 days/month (24 months), whereas Class 1 started at .68 days/month (initial assessment) and ended at .54 days/month (24 months).
The trajectory analysis was run on the full study cohort (N = 1,263). The proportion of teens in each of the five trajectories was similar for the full cohort (FC) and Family Talk (FT) subsample (nonsmokers: FC = 25.4%, FT = 18.6%; Class 1: FC = 20.7%, FT = 29.4%; Class 2: FC = 17.8%, FT = 24.4%; Class 3: FC = 15.4%, FT = 14.5%; Class 4: FC = 20.7%, FT = 13.1%), indicating Family Talk participants are representative of the longitudinal patterns derived from the full study cohort. In the present study (FT subsample), Classes 1 and 2 were combined into an “Infrequent, nonescalating” group (n = 185), Classes 3 and 4 were combined into an “Escalators” group (n = 95), and the nonsmoking group was labeled “Nonsmokers” (n = 64). These combined groups represent distinct adolescent smoking behavior trajectories. Figure 1 displays the number of days smoked per month at baseline, 6-month, 15-month, and 24-month follow-up (from survey data, smoking behavior scale) by trajectory group for Family Talk teens.
Figure 1.
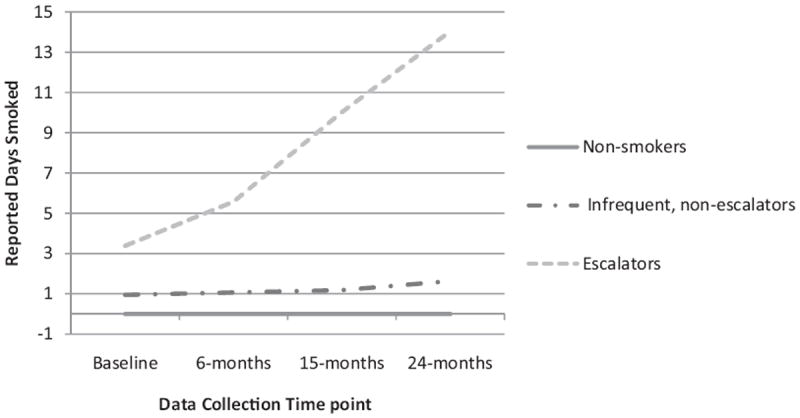
Longitudinal trajectories of adolescent cigarette smoking. Graph represents self-reported smoking at each measurement wave for the combined groups (time line follow-back interviews were used in the trajectory analysis).
Observational Measures
Adolescents and parents participated in a structured dyadic observational task embedded in a broader observational assessment consisting of three 10-min segments (see Wakschlag et al., 2011, for a full description of the Family Talk discussion paradigm). Two of the discussion segments have been used in previous observational research: a discussion of day-to-day family experiences (Cui & Conger, 2008) and a problem-solving task (Wakschlag, Chase-Lansdale, & Brooks-Gunn, 1996). The third segment was a discussion paradigm unique to this study involving a 10-min discussion about cigarette smoking. Parent–teen discussions were conducted separately for each parent, with order of parent discussions randomly determined by a coin flip. Most discussions were conducted in families’ homes (93%).
FTAS discussion task
In order to facilitate a 10-min conversation between parents and teens about salient facets of cigarette smoking, parents and teens took turns reading “conversational triggers,” designed to “press” for variability on smoking-related topics (Cui & Conger, 2008). The three parent triggers were “Let’s talk about…” (a) “My experiences with cigarettes and smoking”; (b) “What parents do if they find out that their teen is smoking”; and (c) “What parents do if they find out that their teen has become a regular smoker.” Teen “triggers” were “Let’s talk about…” (d) “How people in our family feel about cigarette smoking”; and (e) “How today’s teens make decisions about cigarette smoking.”
FTAS global codes (see Wakschlag et al., 2011)
The FTAS is a global, rather than an event-based, coding system. Codes are integrative judgments based on observation of the full discussion segment that include both qualitative (e.g., intensity, pervasiveness) and quantitative (e.g., frequency) aspects of conversational behavior. Behavior is coded along a 9-point scale ranging from 1 (Not at all characteristic) to 9 (Mainly characteristic).
Parents were coded for Level and Consistency of Disapproval about smoking, which was defined as strength, consistency, and pervasiveness of expressed verbal and nonverbal disapproval about smoking. Smoking Expectancies were degree to which parents expressed explicit expectations about the likelihood that teens, in general, and this teen in particular, would smoke now or in the future. On the basis of established guidelines (Cicchetti et al., 2006), the intraclass correlation (ICC) for the disapproval code was in the substantial range (ICC = .76), whereas the ICC for the smoking expectancies code was in the acceptable range (.59).
Observed adolescent solicitation and disclosure about smoking coding system
As part of the consent process, adolescents were told that the research team would not disclose their self-reported smoking behavior to their parents. Teens were also told that they did not have to disclose their smoking history or status. The directions given to dyads prior to the smoking discussion task did not specifically require parents and adolescents to discuss the teens’ own smoking behavior or history. However, in many discussions, parent–teen dyads did have at least one exchange about the teen’s smoking behavior either because parents directly asked their teens or because teens spontaneously discussed their smoking experiences.
Although global coding systems use continuous scales to capture integrative judgments of affective and qualitative aspects of conversational behavior, content coding systems code for the presence or absence of specific types of statements. A coding system was created to capture the content of parent–adolescent exchanges related to teens’ smoking experiences. On the basis of a random selection of 20 parent–teen interactions (3.8%) of the total, the first author along with the two primary coders who were blind to study hypotheses created categories for different types of parental solicitation and teen statements about their smoking experiences. These were further refined through exploratory coding of 40 (7.6%) interactions. The complete dialogue from coded exchanges was transcribed for further verification. Example categories of parental solicitations, adolescent responses, and adolescent disclosure are presented in Table 1. Coders were trained to reliability standards (80% agreement with each other and criterion [first author]). To monitor ongoing interrater reliability, 20% of the interaction segments were randomly selected for double-coding. All disagreements on these double-coded segments were resolved via consensus meetings, and subsequent analyses were conducted on the consensus codes.
Table 1.
Categories and Example Codes From the Content Information Management Coding System
| Coded speaker | Quest/statement category | Example statements from the observed discussions about smoking |
|---|---|---|
| Parental solicitations | Past smoking (tried) | Have you ever smoked? |
| You’ve never smoked, right? (rhetorical) | ||
| You’ve tried smoking, right? (rhetorical) | ||
| Have you had any experiences with smoking? | ||
| Current smoking | Do you smoke? | |
| You don’t smoke, right? (rhetorical) | ||
| Why don’t you smoke? | ||
| Relevant follow-up questions | When did you smoke? | |
| How many times have you smoked? | ||
| Have you smoked since (that experience)? | ||
| Was that the only time you smoked? | ||
| Adolescent responses and spontaneous disclosures | Related to past smoking (tried) | Yes (no elaboration) |
| Nonverbal yes | ||
| Yes, I’ve tried smoking once/a few times. | ||
| Yes, I tried smoking but I didn’t like it. | ||
| No (no elaboration), or nonverbal no | ||
| No. I have never tried smoking. | ||
| I haven’t had any experiences with cigarettes or smoking. | ||
| Current smoking | (Yes) I smoke. | |
| (No) I don’t smoke. | ||
| No, but I have tried smoking. | ||
| Additional information related to smoking | I smoked within the past year. | |
| I smoked more than a year ago, or “a long time ago.” | ||
| I smoked just a puff, not a whole cigarette. | ||
| I smoked one cigarette. | ||
| I smoked more than one cigarette. | ||
| I only smoked once, or that was the only time. | ||
| I smoked more than once/a few more times. |
Observed parental solicitations
Parents were coded when they asked about their teens’ smoking behavior. Codes distinguished between parents asking about current smoking behavior or asking whether the teen had ever smoked at any point in their his or her (tried smoking), and whether parents asked directly, indirectly, or rhetorically. Relevant follow-up questions concerning how recently the teen had smoked and the total number of cigarettes they had ever smoked were also coded (see Table 1). High levels of interrater reliability were achieved both for recognition of parental solicitation (k = .85) and for whether the solicitation concerned past (k = .91) or current smoking behavior (k = .78).
Observed adolescent responses to parental solicitations and spontaneous disclosure
Adolescents’ observed statements were coded for their responses to smoking-related parental solicitations or when teens spontaneously disclosed information about their own smoking behavior without a parental solicitation (see Table 1). Similar to parental solicitation, teens’ statements were coded for whether the teen was discussing current smoking behavior or earlier experiences with smoking (tried smoking). Statements indicating how recently the teen had smoked and the total number of cigarettes the teen had smoked in their lives were also coded. In a few parent–adolescent dyads, adolescents provided ambiguous answers to parental solicitations, and the additional information helped clarify whether adolescents were discussing current or past smoking behavior. Interreliability was adequate for responses to parental solicitations (current smoking behavior: k = .83, past smoking behavior: k = .74), spontaneous disclosure (current: k = .76, past: k = .68), and content of follow-up information (k = .59).
Observed parental knowledge of teen previous smoking behavior
Some dyads stated that the parent had previous knowledge concerning the teen’s past smoking behavior (mother: n = 55 [16.8%]; father: n = 19 [9.2%]). Parents stated that they gained knowledge of teens’ smoking behavior through a variety of means, including the teen directly telling the parent, actually viewing the teen smoking, or finding cigarettes in the teen’s possession. These types of discussions were not anticipated but were coded to determine whether parents’ prior knowledge was associated with patterns of disclosure and solicitation. Parental knowledge was only coded if both the teen and the parent stated that parents already had knowledge and expressed specific information about what parents knew; vague parental suspicions were not coded (“I bet you have tried [smoking]”). Interrater reliability for parental observed knowledge was moderate (k = .58).
Observed information management coding
On the basis of patterns of observed smoking discussion, adolescents were grouped into categories of discussion initiation and information management. This secondary coding was completed via consensus between the first author and a secondary coder.
Smoking discussion initiation categories
Coded exchanges were first examined for whether discussion of the teens’ own smoking behavior was initiated by the parent (parental solicitation) or by the teen (spontaneous disclosure). When parents and adolescents had multiple separate exchanges about the teens’ smoking behavior, whoever initiated the first exchange was coded as the initiator (parents could be coded as initiators if a solicitation about the teen’s current smoking behavior [“Do you smoke?”] followed a teen disclosure about former smoking experiences). Each dyad received a code for discussions of teens’ own smoking behavior (1 = parent-initiated, 2 = teen-initiated, 0 = teens’ smoking behavior not discussed).
Observed information management groups
On the basis of theory and previous research, adolescents were grouped into categories of information management by combining adolescents’ observed statements about their current and past smoking behavior with their self-reported smoking status. Because of the recruitment and screening procedure used in the present study, all participants had engaged in cigarette smoking at some point in their lives. To categorize adolescents’ current smoking behavior, we used adolescents’ self-label (current experimenter = smoker or social/occasional smoker) because this item captured adolescents’ self-identification with being a casual smoker. Teens varied in how open and honest they were about their previous smoking behavior and current smoking status.
Full disclosure
A full disclosure category included adolescents who communicated information that was consistent with their smoking history and self-described smoking status. When parents solicited currently nonsmoking teens about their previous smoking behavior (e.g., “Have you ever tried smoking?”), fully disclosing teens truthfully admitted trying smoking. Not currently smoking teens were also coded as full disclosers if they spontaneously admitted to previous smoking experiences without being asked by parents. Adolescents who self-identified as currently smoking were included in this group if they admitted current smoking behavior either spontaneously or in response to parental solicitation. In a few dyads in which teens fully disclosed, parents also expressed having previous knowledge (observed parental knowledge). These teens confirmed parents’ knowledge and were retained in the full disclosure group.
Active secrecy
Adolescents in the active secrecy group communicated information about their smoking behavior, which was not consistent with their self-reported smoking status (similar to lying in previous research). Not currently smoking teens were included in this category if they denied ever smoking either spontaneously or when asked. Teens who self-identified as current smokers were categorized as being actively secretive if they denied current smoking behavior either in response to a parental solicitation about current smoking behavior or spontaneously denied currently smoking. In a few dyads, parents had previous knowledge of the teens’ previous smoking behavior (observed parental knowledge), but the teens were actively secretive about their current behavior, either spontaneously or in response to solicitations.
Incomplete strategies
Many adolescents gave parents some information about their past or current smoking behavior while not being completely upfront. Consistent with previous research, some teens were labeled partial disclosers. Partial disclosure has been operationalized as “telling parents, but leaving out important details” (Smetana et al., 2009). In the present study, these important details were defined as “currently experimenting with smoking.” Thus, partial disclosers self-reported a current smoking status and admitted trying cigarette smoking (either in reaction to solicits or spontaneously), but denied current smoking behavior (giving parents some information about their previous behavior but leaving out information about current smoking experimentation). Similarly, some adolescents accurately stated that they were not currently smoking (matched self-label) but did not take the opportunity to discuss their previous smoking experiences. Because these teens did not actually disclose any information about their smoking behavior, they could not be labeled as full disclosers. These teens were labeled nondisclosers.
Avoidance
The avoidance category included adolescents who responded to solicitations by simply refusing to answer or by changing the subject.
Overview of Statistical Analyses
Univariate analyses examined whether the observed smoking discussion variables (parent vs. adolescent initiation and adolescent information management strategies) were associated with aspects of the study design, including parent gender, one- versus two-parent families, across first and second interactions within two-parent families, and observed parental knowledge. Next, multinomial and binary logistic regression models tested associations between parenting variables (general and smoking-specific) and observed smoking discussion variables (initiation and information management strategies). Finally, multinomial models tested associations between observed smoking discussion variables and longitudinal smoking trajectories. Similar to previous family observation research (Wakschlag et al., 2011), interactions involving mothers and fathers were examined separately. Logistic models that included information management were run on subsamples (dyads in which adolescents’ own smoking behavior was discussed), which reduced the n for the models. A common “rule of thumb” is that logistic regression models should include a minimum of 10 outcome events per predictor variable (Peduzzi, Concato, Kemper, Holford, & Feinstein, 1996), but recent research has found that this rule can be relaxed under some circumstances, specifically for smaller sample observational studies hoping to control for confounding variables (Vittinghoff & McCulloch, 2007). However, a series of steps was taken to ensure that findings from the logistic models were stable. Model diagnostics indicated that multicollinearity was not problematic. Post hoc stepwise models verified that significant predictors did not result from spurious or suppression effects in the full model. Coefficients and significance levels were stable across these checks.
Results
Descriptive Statistics
In over half of the observed conversations, adolescents’ own smoking behavior was discussed (mothers: 55.5%; fathers: 57.5%). Although a majority of these discussions were initiated by parents via direct solicitation (mothers: 35.8%; fathers: 34.3%), a sizable percentage of teens spontaneously initiated discussions (with mothers: 19.6%; with fathers: 23.2%). When discussing their smoking behavior, many adolescents fully disclosed (to mothers: 39.9%; to fathers: 32.7%), though a majority admitted to previous and not current smoking (teens fully disclosed their current smoking behavior in only six conversations). A sizable number of teens also engaged in active secrecy (with mothers: 29.8%; with fathers: 26.5%). A smaller though substantial number of teens engaged in partial (with mothers: 13.1%; with fathers: 17.7%) and nondisclosure (with mothers: 17.3%; with fathers: 23.0%). Partial and nondisclosure were combined into an incomplete strategies category for analyses. Teens used avoidance in only 14 total interactions (nine with mothers, and five with fathers), so it was not included in further analyses. Descriptive statistics and correlations among the general and smoking-specific parenting variables are presented in Table 2.
Table 2.
Descriptive Statistics and Correlations for General and Smoking-Specific Parenting Variables (Mothers and Fathers, Separately)
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender: (female) | — | .05 | .04 | .10 | −.17** | .08 | .06 | .05 | −.04 | .03 |
| 2. Parent smoking (current) | −.10 | — | .07 | .12* | −.04 | −.04 | .01 | .41*** | .06 | −.03 |
| 3. Parental warmth | .07 | .11 | — | .63*** | −.14* | .30*** | .10 | .03 | −.04 | .04 |
| 4. Open communication | .12 | −.02 | .72*** | — | .06 | .27*** | .05 | .06 | −.08 | .00 |
| 5. Problem communication | −.19** | .12 | −.23*** | .28*** | — | −.07 | −.01 | −.10 | −.06 | .01 |
| 6. Smoking messages | .02 | −.02 | .30*** | .26*** | −.12 | — | .30*** | .07 | −.02 | −.08 |
| 7. Substance rules | .01 | .12 | .12 | .08 | .00 | .30*** | — | .12* | −.07 | −.13* |
| 8. Observed disapproval | .01 | .26*** | .00 | .01 | .00 | .03 | .21*** | — | −.06 | −.06 |
| 9. Observed expectancies | .07 | .08 | .01 | −.05 | .07 | −.12 | −.12 | −.11 | — | .07 |
| 10. Adolescent smoking behavior (self-report, baseline) | .06 | −.02 | .00 | −.05 | .01 | −.11 | −.09 | −.05 | .07 | — |
| Mothers | ||||||||||
| M/N | 182 | 73 | 3.03 | 34.32 | 31.79 | 2.26 | 4.31 | 6.31 | 4.24 | 1.51 |
| SD/% | 56.7% | 22.7% | 0.80 | 10.46 | 7.30 | 0.53 | 0.87 | 1.81 | 1.83 | 3.49 |
| Range | 1–4 | 10–50 | 10–48 | 1–3 | 1–5 | 1–9 | 1–9 | 1–30 | ||
| Fathers | ||||||||||
| M/N | 111 | 53 | 2.91 | 32.09 | 31.21 | 2.29 | 4.31 | 5.98 | 3.95 | 1.51 |
| SD/% | 53.6% | 25.6% | 0.84 | 10.31 | 7.28 | 0.51 | 0.89 | 2.04 | 1.85 | 3.49 |
| Range | 1–4 | 10–50 | 10–50 | 1–3 | 1–5 | 1–9 | 1–9 | 1–30 |
Note. Correlations for mothers are above and correlations for fathers are below the diagonal.
p < .05.
p < .01.
p < .001.
Associations Between Coded Observation Variables and Design Characteristics
Parent gender
Neither initiation (parent-initiated, teen-initiated, smoking not discussed) nor adolescents’ use of different information management strategies varied by parent gender. However, compared with fathers (9.2%), proportionally more mothers (16.8%) communicated prior knowledge of their teens’ smoking during the dyadic interactions, χ2(2, 528) = 6.17, p = .013.
One- versus two-parent families
Neither initiation nor use of information management strategy significantly varied as a function of whether adolescents participated with one or two parents.
Conversation order effects in two-parent families
Within families where two parents participated, percentages of dyads in which the parents initiated (first: 31%, second: 37%), teens initiated (first: 24.4%, second: 21.7%), and the teens’ smoking was not discussed (first: 44.6%, second: 41.3%) were nearly identical across the two interactions. A significant chi-square, χ2(4, 184) = 23.33, p < .001, indicated that teens were more likely to initiate in the second discussion when they had initiated in the first. Parents and teens were also less likely to discuss the teens’ smoking behavior in the second parent discussion when smoking was also not discussed in the first conversation. A similar pattern emerged during comparisons of adolescent information management use (full disclosure, active secrecy, partial strategies), χ2(9, 184) = 59.48, p < .001. Adolescents who fully disclosed to the first parent were significantly more likely to fully disclose to the second parent. There was no stability or consistent pattern across the two interactions when adolescents engaged in active secrecy or incomplete strategies.
Observed parent knowledge
Observed parental knowledge was associated with smoking discussion initiation: mothers, χ2(2, 321) = 17.87, p < .000; fathers, χ2(2, 207) = 8.83, p = .012, and information management: mothers only, χ2(2, 321) = 10.42, p < .005. Teens were more likely to initiate conversations about their own smoking with mothers (35.2% vs. 16.5%) and fathers (47% vs. 20.7%) when parents had previous knowledge. Adolescents were more likely to fully disclose (59.5% vs. 33.3%) and less likely to engage in incomplete strategies (14.3% vs. 35.7%) when mothers had previous knowledge.
Predicting Smoking Discussion Initiation and Teen Information Management Strategies
Analyses examined demographic (teen gender and ethnicity, parental smoking status), general parenting (open and problematic communication, and warmth), and smoking-specific parenting (smoking messages, substance rules, observed smoking disapproval, and observed smoking expectancies) as predictors of smoking discussion variables (mothers and fathers, separately). First, we examined predictors of parent versus teen initiation. Next and consistent with Frijns et al. (2010), we modeled predictors of full disclosure versus concealment (combined active secrecy and incomplete strategies). Finally, differences between types of concealing strategies were explored (active secrecy vs. incomplete strategies).
Parent and teen initiation
Multinomial logistic regressions examined predictors of teen and parent discussion initiation with dyads in which teens’ own smoking behavior was not discussed as the comparison group. Results for mothers are displayed in Table 3. African American mothers were more likely to solicit. All mothers were more likely to solicit when teens reported more illicit substance use rules, which were also associated with increased adolescent initiation. Teens were less likely to initiate when they reported more communication problems with mothers and when mothers displayed higher levels of disapproval for smoking within the observed conversation. Only one significant finding emerged in father models. Compared with boys, girls were more likely to initiate conversations concerning their own smoking behavior in conversations with fathers (B = 1.42, SE = .42, OR = 4.12, 95% CI [1.81, 9.35], p = .001).
Table 3.
Multinomial Logistic Regression Model Examining Predictors of Mother and Teen Initiation With Dyads in Which Teen Smoking Is Not Discussed as the Comparison Group (n = 321)
| Variable | Mother initiation (solicitation)
|
Teen initiation with their mothers
|
||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | OR | 95% CI | B | SE | OR | 95% CI | |
| Gender (female) | .16 | .27 | 1.18 | [.69, 2.01] | .40 | .33 | 1.49 | [.78, 2.85] |
| Ethnicity | ||||||||
| African American | .74 | .34 | 2.09* | [1.07, 4.06] | .36 | .44 | 1.43 | [.61, 3.36] |
| Hispanic | .53 | .40 | 1.70 | [.77, 3.74] | .53 | .49 | 1.69 | [.65, 4.37] |
| Parent: current smoker | −.47 | .35 | .62 | [.31, 1.24] | ||||
| General parenting | ||||||||
| Warmth | −.09 | .22 | .91 | [.59, 1.41] | .08 | .28 | 1.08 | [.63, 1.86] |
| Open communication | −.01 | .009 | .99 | [.97, 1.01] | .004 | .01 | 1.00 | [.98, 1.03] |
| Problem communication | −.01 | .01 | .99 | [.97, 1.01] | −.03 | .01 | .97** | [.95, .99] |
| Smoking-specific parenting | ||||||||
| Smoking messages | .16 | .27 | 1.17 | [.69, 1.99] | .31 | .34 | 1.36 | [.71, 2.27] |
| Substance rules | .53 | .17 | 1.70** | [1.21, 2.39] | .42 | .21 | 1.51* | [1.01, 2.27] |
| Observed disapproval | −.11 | .08 | .90 | [.76, 1.06] | −.27 | .10 | .76** | [.63, .92] |
| Observed expectancies | .08 | .07 | 1.03 | [.93, 1.25] | .14 | .09 | 1.15 | [.97, 1.37] |
Note. OR = odds ratio; CI = confidence interval.
p < .05.
p < .01.
Full disclosure versus concealing strategies
Using the sub-sample of conversations in which teens’ smoking behavior was discussed (n with mothers = 168, n with fathers = 113), logistic regressions (mother and father separately) examined predictors of adolescent use of full disclosure compared with concealing strategies. Results for mothers are presented in Table 4. Teens were more likely to fully disclose to mothers when they reported more open communication with mothers and less likely to disclose with higher levels of problematic communication. No significant findings emerged in the father model.
Table 4.
Logistic Regression Models Predicting Adolescent Information Management Strategies in Discussions With Mothers: Full Disclosure Versus All Concealment Strategies and Active Secrecy Versus Partial and Nondisclosure Combined
| Variable | Full disclosure vs. all concealment strategies
|
Active secrecy vs. incomplete strategies
|
||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | OR | 95% CI | B | SE | OR | 95% CI | |
| Gender (female) | .56 | .39 | 1.74 | [.81, 3.73] | 1.14 | .55 | 3.14* | [1.07, 9.18] |
| Ethnicity | ||||||||
| African American | −.70 | .48 | .50 | [.20, 1.26] | −.78 | .54 | .46 | [.16, 1.33] |
| Hispanic | −.07 | .51 | .93 | [.34, 2.53] | 1.37 | .74 | 3.93† | [.92, 16.72] |
| Parent: current smoker | −.03 | .48 | .97 | [.38, 2.49] | .63 | .67 | 1.87 | [.50, 6.94] |
| General parenting | ||||||||
| Warmth | −.41 | .29 | .66 | [.37, 1.17] | .13 | .38 | 1.14 | [.54, 2.42] |
| Open communication | .03 | .01 | 1.03** | [1.01, 1.05] | −.02 | .01 | .98 | [.95, 1.01] |
| Problem communication | −.03 | .01 | .97** | [.94, .99] | −.02 | .02 | .98 | [.95, 1.01] |
| Smoking-specific parenting | ||||||||
| Smoking messages | .48 | .38 | 1.62 | [.77, 3.43] | .40 | .47 | 1.49 | [.59, 3.77] |
| Substance rules | −.02 | .28 | .98 | [.56, 1.70] | .91 | .40 | 2.48* | [1.13, 5.45] |
| Observed disapproval | .05 | .11 | 1.05 | [.85, 1.29] | .08 | .14 | 1.08 | [.83, 1.41] |
| Observed expectancies | .17 | .10 | 1.18† | [.97, 1.44] | −.33 | .14 | .72* | [.55, .94] |
Note. OR = odds ratio; CI = confidence interval.
p < .10.
p < .05.
p < .01.
Active secrecy versus incomplete strategies
Using the sub-sample of conversations in which the teens engaged in concealing strategies (n with mothers = 101, n with fathers = 76), logistic regressions (mother and father separately) examined predictors of teens’ use of active secrecy versus incomplete strategies. Results for mothers are presented in Table 4. Girls were more likely to engage in active secrecy over incomplete strategies. Teens were more likely to engage in active secrecy with their mothers when they reported higher levels of illicit substance rules. Teens were less likely to use active secrecy when mothers engaged in high levels of observed smoking expectancy (i.e., stated that they expected their teens would experiment with smoking). Compared with Whites, African American teens were less likely to engage in active secrecy with their fathers (B = −2.57, SE = 1.24, OR = .08, 95% CI [.01, .86], p = .037).
Controlling for adolescent smoking and observed parental knowledge
Significant findings remained unchanged with adolescent baseline smoking behavior and observed parental knowledge added to the models. Teen baseline smoking was not associated with initiation or information management.
Predicting Longitudinal Smoking Trajectories
Multinomial regression analyses (mothers and fathers, separately) examined smoking discussion initiation and information management strategies as predictors of adolescent smoking trajectories with infrequent, nonescalating adolescents as the comparison group. The models included the demographic, general parenting, and smoking-specific parenting variables as the models above (observed parental knowledge was not significantly associated with smoking trajectories). To account for the initial difference in smoking behavior between the trajectories (intercepts), the models also controlled for adolescent self-reported smoking at baseline (days smoked in the past 30 days). Not surprisingly, self-reported smoking behavior was positively associated with escalation and negatively associated with nonsmoking group membership in all models. In addition, in all models African American adolescents were more likely to be nonsmokers (ORs = 4.67–10.66, ps < .01) and less likely to be escalators (ORs = .05–.23, ps < .01).
Parent and teen initiation
Increased problem communication with mothers reduced the likelihood that adolescents were in the nonsmoker group (B = −.03, SE = .01, OR = .98, 95% CI [.95, .99], p = .033), and maternal solicitation of teens’ smoking behavior increased the likelihood of being in the escalator group (B = .98, SE = .35, OR = 2.67, 95% CI [1.36, 5.26], p = .005). Neither parent nor teen initiation was associated with adolescent smoking trajectories. No significant findings emerged in the father model.
Full disclosure versus concealment strategies
Within the subsample of dyads in which adolescents’ smoking behavior was discussed (mothers = 168, fathers = 113), observed maternal smoking disapproval reduced the likelihood that adolescents were in the nonsmoker group (B = −.33, SE = .16, OR = .72, 95% CI [.52, .99], p = .047). Adolescent information management strategies were not associated with adolescent smoking trajectories. No significant findings emerged for fathers.
Active secrecy versus incomplete strategies
Within the sub-sample of adolescents who engaged in concealing strategies (mothers = 101, fathers = 76), mothers’ increased use of smoking disapproval also reduced adolescent membership in the nonsmoker group (B = − .33, SE = .16, OR = .72, 95% CI [.52, .99], p = .047). More problem communication with mothers increased the likelihood (B = .09, SE = .03, OR = 1.09, 95% CI [1.03, 1.16], p = .005) and less open communication decreased the likelihood (B = −.06, SE = .03, OR = .95, 95% CI [.90, .99], p = .029) of escalator status. Adolescents who engaged in active secrecy rather than incomplete strategies with their mothers were more likely to be in the escalator group (B = 2.53, SE = .92, OR = 12.60, 95% CI [2.07, 76.64], p = .006). No significant father findings emerged.
Discussion
The present study provides nuanced insights into parent–teen discussions about teens’ engagement in a specific health risk behavior by merging the literature on smoking- specific parenting (Kodl & Mermelstein, 2004) with the burgeoning literature on adolescent disclosure. Smoking-specific parenting behaviors predicted smoking-specific parental solicitation, and both general and smoking-specific parenting behaviors predicted adolescent information management strategies. Additionally, maternal solicitation and adolescent active secrecy were associated with longitudinal escalation of teens’ smoking behavior. Research examining links between teen disclosure/secrecy and subsequent delinquency has primarily assessed discussion of broader aspects of teens’ activities (e.g., teens’ use of free time). Such parental knowledge is certainly important, but the mechanism through which such general knowledge is longitudinally protective against specific forms of teen delinquency is not clear (Kerr et al., 2010). The present study provides evidence for the incremental utility of considering what an adolescent is disclosing or keeping secret, as behavior-specific strategies may be more strongly related to teens’ subsequent engagement in that specific behavior. To our knowledge, this is the first study to derive patterns of solicitation and information management from directly observed conversations. Observed parental communication about smoking influenced teens’ willingness to initiate conversations about and honestly discuss their smoking behavior in live discussions. The ability to directly assess parents’ in vivo framing of health-risk behavior is an additional benefit of an observational methodology.
Predictors of Conversation Initiation and Adolescent Information Management
Compared with other mothers, African American mothers were more likely to solicit about their teens’ smoking experiences. African American families have been described as more hierarchical and controlling than European American families (Bulcroft, Carmody, & Bulcroft, 1996), and such engagement in direct solicitation may be a component of such authoritarian parenting. Increased family rules about illicit substance also increased the likelihood that mothers would solicit their teens about their smoking experiences and behavior. The association between stricter rules and active attempts to gain information indicates overlap in types of maternal behavioral control across teen-reported and observed conversations.
Consistent with previous research, teens were more likely to initiate conversations about their smoking experiences to mothers when they self-reported less maternal problem communication (Soenens, Vansteekiste, Luyckx, & Goossens, 2006). When parents are viewed as unsupportive and untrustworthy, adolescents may feel less secure initiating discussions about difficult issues such as their engagement in problem behavior. Teen initiation was also less likely when mothers engaged in high levels of observed smoking disapproval. Parental antismoking messages predict reduced cigarette use in adolescence (Chassin et al., 2005), but teens may eschew discussing their own smoking experiences to avoid punishment from fervently antismoking parents or avoid disappointing parents who adamantly vocalize their denunciations. Self-reported smoking messages were not associated with initiation, indicating that in vivo reactions to mothers’ spoken smoking beliefs may more strongly impact teens’ conversation strategies.
In terms of information management, adolescents were more likely to fully disclose to mothers whom they rated high on open and low on problematic communication (Tilton-Weaver et al., 2010). Adolescents may view parents who have a history of engaging in receptive communication as more trustworthy (Tasopoulos-Chan, Smetana, & Yau, 2009), leading them to feel safer openly discussing past and current smoking behavior. We also examined in the present study potential heterogeneity among teens who used different concealing strategies. Girls were more likely to engage in active secrecy than use concealing strategies. Girls have been found to disclose general information at higher levels than boys (Keijsers et al., 2010), but girls could be more strongly motivated to keep their engagement in health risk behaviors secret from their mothers. Adolescents were more likely to engage in incomplete strategies rather than active secrecy if their mothers expressed higher levels of observed smoking expectancies (as coded globally with the FTAS). Adolescents may feel more comfortable discussing at least some aspects of their smoking experiences when parents discuss the allure of smoking, recognize the temptation to experiment, and expect that most teens will try smoking at some point. In contrast, adolescents were more likely to engage in active secrecy if they self-reported higher levels of family substance use rules. An understanding of parents’ implicit negative attitudes toward smoking may heighten teens’ awareness of undesirable parental reactions, including punishment (Sherman, Chassin, Seo, & Macy, 2009). Adolescents may be highly motivated to keep all information about their cigarette use secret from such parents, and such dishonest reactions to punitive environments may be rooted in early childhood (Talwar & Kang, 2011).
Predictors of Longitudinal Smoking Trajectories
Over and above demographic variables, initial smoking behavior, and parenting variables, maternal solicitation and active secrecy were associated with longitudinal adolescent smoking trajectories. Locating characteristics and experiences distinguishing “adolescence limited” smokers from “life course” smokers, who will increase their level of smoking, is critical for public health practitioners and intervention designers seeking to reduce smoking in adulthood. The present study’s longitudinal smoking trajectories extended only to late adolescence and not into adulthood, but findings suggest that patterns of parent–adolescent discussion related to teens’ own smoking behavior may usefully differentiate distinct smoking trajectories.
Surprisingly, maternal solicitation increased the likelihood of teen smoking escalation. Previous research found that parental solicitation frequency is negatively associated with baseline (Keijsers, Frijns, Branje, & Meeus, 2009) but not subsequent delinquent behavior (Eaton, Krueger, Johnson, McGue, & Iacono, 2009). The large trajectory intercept differences indicated that escalators were already smoking more average days per month at initial assessment than infrequent, nonescalators (see Figure 1). Adolescents who smoke also engage in other behaviors such as socializing with deviant or smoking peer groups (Kobus, 2003), which may have subtly aroused mothers’ suspicions and encouraged them to ask about their teens’ smoking experiences. However, maternal solicitation significantly predicted smoking escalation over and above teen smoking behavior at initial assessment, and teen self-reported smoking behavior was not associated with maternal solicitation. Thus, an alternative explanation is that maternal solicitation was associated with increased smoking, though not deliberately. Recent research has found that forms of parental behavioral control may have inadvertent negative outcomes, such as prohibitions against problem peer associations leading to increases in delinquent peer associations (Keijsers et al., 2011). Mothers who solicited also had higher levels of substance use rules. Heightened control over a specific issue may have the unintended consequence of subtly increasing the appeal of “age-graded behaviors” such as cigarette smoking, which is illegal for teenagers but legal for adults and could be viewed by teens as a behavior signaling adult-level maturity. Adolescents experimenting with cigarette use may also have more “rebellious” personalities, and such recalcitrant teens may be more likely to engage in reactance against parental behavioral control (de Leeuw, Scholte, Sargent, Vermulst, & Engels, 2010).
Such reactance was also potentially evident among teens who engaged in active secrecy, which predicted smoking escalation. This association could also not be fully explained by intercept differences in the smoking trajectories. Models controlled for baseline smoking, and self-described current smokers were equally likely to be in the incomplete (51.9%) and active secrecy groups (48.1%). Adolescent secrecy erodes parent–adolescent relationships (Keijsers et al., 2010) and longitudinally predicts internalizing and externalizing problems (Frijns, Finkenauer, Vermulst, & Engels, 2005). The fact that active secrecy and not full disclosure predicted increased smoking is also consistent with previous research, which found secrecy-maladjustment but not disclosure-maladjustment associations (Frijns et al., 2010). The present study builds on this work by locating potential heterogeneity among types of secretive strategies. Adolescents who are progressively increasing their smoking behavior may be more acutely anxious about parental interference with their cigarette use. This anxiety may motivate them to shield all information about their smoking behavior and history from parents. Teens who are sporadic, recreational smokers may see less potential hazard in disclosing at least some information about their smoking experiences. Alternatively, even the partial information gained from teens’ incomplete strategies may alert parents to increase smoking-related monitoring behaviors, which could limit teens’ opportunities to escalate their smoking behavior.
This finding contrasts with previous research in which concealment strategies robustly loaded onto a single factor (Laird & Marrero, 2010). Previous research used self-report scales assessing strategies for a range of activities, including items that do not specify an activity such as “spending free time.” Everyday exchanges about nonspecific aspects of an adolescent’s life differ dramatically from discussion of teen’s health risk behavior. In such conversations, teens may risk punishment, disruption of the parent–adolescent relationship, or more vigilant parental monitoring (an especially undesirable outcome for teens wishing to engage in further health risk behavior). Awareness of the potential “high stakes” involved in such conversations may make adolescents extremely attentive to slight discrepancies in the information they share, enhancing the appeal of specific concealment strategies. The present study indicates that subtle distinctions in teens’ discussion of health risk activities may help predict subsequent behavior.
Parent Characteristics: Gender and Parental Smoking Status
In contrast to previous research, most parent–adolescent discussion variables did not differ by parent gender. Also unexpectedly, analyses located no paternal predictors of initiation or information management, and the smoking discussion variables did not predict the smoking trajectories in father models. Follow-up analyses indicated that a lack of significant findings most likely did not result from the smaller n of the father models; no paternal variables even trended toward significance. Fathers undoubtedly impact adolescent engagement in problem behavior, so future research examining smoking-related discussion should consider additional father behaviors. We had also hypothesized that teens would feel more comfortable discussing their smoking behavior with smoking parents, but this hypothesis was not supported. There is a great deal of heterogeneity in smoking and nonsmoking parents’ smoking attitudes, rules, and reactions to teens’ smoking behavior. Such variability may better predict teen smoking-related disclosure than whether parents smoke. Parental smoking status may also moderate associations between parenting behaviors and adolescent smoking trajectories (Wakschlag et al., 2011). The present study lacked the power necessary to test such interactions, but future research should explore this possibility.
Limitations and Future Directions
Findings from the present study need to be interpreted in light of its limitations. Focusing on cigarette smoking and including only adolescents with a history of smoking may limit generalizability of these findings to discussions about other problem behaviors and nondeviant activities or to populations where smoking is more normally distributed. This study assessed multiple parental behaviors, but other aspects of parenting may contribute to adolescents’ smoking-specific information management and subsequent smoking behavior. The smoking trajectories intercepts were significantly different and strongly associated with trajectory slopes, which may explain why many parenting variables did not distinguish the trajectories. Parenting behaviors such as smoking messages may distinguish other patterns of teen smoking (e.g., initiators vs. noninitiators). Only 55% of parent–adolescent dyads discussed teens’ smoking experiences, which could point to a lack of generalizability, though this may more closely approximate the rate at which teens actually discuss their own problem behavior with parents. Parent order was randomized for two-parent families, but it is possible the second discussion was influenced by unaccounted-for processes in the first. Certain patterns (teen initiation and full disclosure) were consistent across both interactions, so unmeasured individual variables may account for some of the variance in adolescent discussion variables. Parental prior knowledge of teens’ smoking behavior did not affect any outcome, but future research should test whether communication processes differ when parents have previous knowledge. Finally, race was included as a control but was not tested as a moderator. Solicitation predicted smoking escalation, African American mothers engaged in higher levels of solicitation, but African American teens were less likely to be escalators. Future research should explore the intriguing possibility that links between teen smoking and parental solicitation may vary for different racial groups.
The smoking-specific parenting literature provides evidence for the incremental utility of predicting specific outcomes from “behavior-specific” aspects of parenting. The present study indicates adolescent disclosure and information management research may benefit from such increased measurement precision. Direct observations of solicitation and disclosure patterns may provide an important window on individual differences in family communication about health risk behavior. Patterns of teen disclosure and secrecy are embedded in complex and nuanced transactions and communications, and observed differences have important implications for youth development, including subsequent risk behaviors.
Acknowledgments
This research was supported by National Cancer Institute Grant P01CA98262 (principal investigator: Robin Mermelstein). We gratefully acknowledge the contributions of P01 collaborators Kathi Diviak, John O’Keefe, Paul Rathouz, Dick Campbell, Don Hedeker, and Bennett Leventhal to broader aspects of the study. We are also most grateful to Joyce Ho’s careful oversight of the Family Talk Study in her role as project director. We thank Judith Smetana for invaluable consultation.
Contributor Information
Aaron Metzger, Department of Psychology, West Virginia University.
Lauren S. Wakschlag, Department of Medical Social Sciences, Northwestern University Feinberg School of Medicine
Ryan Anderson, Department of Psychology, West Virginia University.
Anne Darfler, Institute for Health Research and Policy, University of Illinois at Chicago.
Juliette Price, Institute for Health Research and Policy, University of Illinois at Chicago.
Zujeil Flores, Institute for Health Research and Policy, University of Illinois at Chicago.
Robin Mermelstein, Institute for Health Research and Policy, University of Illinois at Chicago.
References
- Barber BK, Stolz HE, Olsen JA. Parental support, psychological control, and behavioral control: Assessing relevance, across time, culture, and method. Monographs of the Society for Research in Child Development. 2005;70:1–137. doi: 10.1111/j.1540-5834.2005.00365.x. [DOI] [PubMed] [Google Scholar]
- Barnes HL, Olson DH. Parent-adolescent communication and the circumplex model. Child Development. 1985;56:438–447. doi: 10.2307/1129732. [DOI] [Google Scholar]
- Boone TL, Lefkowitz ES. Mother-adolescent health communication: Are all conversations created equally? Journal of Youth and Adolescence. 2007;36:1038–1047. doi: 10.1007/s10964-006-9138-2. [DOI] [Google Scholar]
- Bulcroft RA, Carmody DC, Bulcroft KA. Patterns of independence giving to adolescents: Variations by race, age, and gender of child. Journal of Marriage and the Family. 1996;58:866–883. doi: 10.2307/353976. [DOI] [Google Scholar]
- Chassin L, Presson C, Rose J, Sherman S, Davis M, Gonzalez J. Parenting style and smoking-specific parenting practices as predictors of adolescent smoking onset. Journal of Pediatric Psychology. 2005;30:333–344. doi: 10.1093/jpepsy/jsi028. [DOI] [PubMed] [Google Scholar]
- Chassin L, Presson CC, Sherman SJ, Edwards PA. The natural history of cigarette smoking: Predicting young adult smoking outcomes from adolescent smoking patterns. Health Psychology. 1990;9:701–716. doi: 10.1037/0278-6133.9.6.701. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Bronen R, Spencer S, Haut S, Berg A, Oliver P, Tyrer P. Rating scales, scales of measurement, issues of reliability: Resolving some critical issues for clinicians and researchers. Journal of Nervous & Mental Disease. 2006;194:557–564. doi: 10.1097/01.nmd.0000230392.83607.c5. [DOI] [PubMed] [Google Scholar]
- Cui M, Conger R. Parenting behavior as mediator and moderator of the association between marital problems and adolescent adjustment. Journal of Research on Adolescence. 2008;18:261–284. doi: 10.1111/j.1532-7795.2008.00560.x. [DOI] [Google Scholar]
- Cumsille P, Darling N, Martinez ML. Shading the truth: The patterning of adolescents’ decisions to avoid issues, disclose, or lie to parents. Journal of Adolescence. 2010;33:285–296. doi: 10.1016/j.adolescence.2009.10.008. [DOI] [PubMed] [Google Scholar]
- Darling N, Cumsille P. Theory, measurement, and methods in study of family influences on adolescent smoking. Addiction. 2003;98(Suppl. 1):21–36. doi: 10.1046/j.1360-0443.98.s1.3.x. [DOI] [PubMed] [Google Scholar]
- Darling N, Cumsille P, Caldwell LL, Dowdy B. Predictors of adolescents’ disclosure to parents and perceived knowledge: Between- and within-person differences. Journal of Youth and Adolescence. 2006;35:659–670. doi: 10.1007/s10964-006-9058-1. [DOI] [Google Scholar]
- Darling N, Cumsille P, Pena-Alamay L, Coatsworth D. Individual and issue-specific differences in parental knowledge and adolescent disclosure in Chile, the Philippines, and the United States. Journal of Research on Adolescence. 2009;19:715–740. doi: 10.1111/j.1532-7795.2009.00608.x. [DOI] [Google Scholar]
- de Leeuw RN, Scholte RH, Sargent JD, Vermulst AA, Engels RC. Do interactions between personality and social-environmental factors explain smoking development in adolescence? Journal of Family Psychology. 2010;24:68–77. doi: 10.1037/a0018182. [DOI] [PubMed] [Google Scholar]
- Eaton NR, Krueger RF, Johnson W, McGue M, Iacono WG. Parental monitoring, personality, and delinquency: Further support for a reconceptualization of monitoring. Journal of Research in Personality. 2009;43:49–59. doi: 10.1016/j.jrp.2008.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frijns T, Finkenauer C, Vermulst AA, Engels RCME. Keeping secrets from parents: Longitudinal associations of secrecy in adolescence. Journal of Youth and Adolescence. 2005;34:137–148. doi: 10.1007/s10964-005-3212-z. [DOI] [Google Scholar]
- Frijns T, Keijsers L, Branje S, Meeus W. What parents don’t know and how it may affect their children: Qualifying the disclosure-adjustment link. Journal of Adolescence. 2010;33:261–270. doi: 10.1016/j.adolescence.2009.05.010. [DOI] [PubMed] [Google Scholar]
- Ge X, Conger RD, Lorenz FO, Simmons RL. Parent’s stressful life events and adolescent depressed mood. Journal of Health and Social Behavior. 1994;35:28–44. doi: 10.2307/2137333. [DOI] [PubMed] [Google Scholar]
- Harakeh Z, Scholte RHJ, Vermulet AA, de Vries H, Engels RCME. The relations between parents’ smoking, general parenting, parental smoking communication, and adolescents’ smoking. Journal of Research on Adolescence. 2010;20:140–165. doi: 10.1111/j.1532-7795.2009.00626.x. [DOI] [Google Scholar]
- Keijsers L, Branje SJT, Frijns T, Finkenauer C, Meeus W. Gender differences in keeping secrets from parents in adolescence. Developmental Psychology. 2010;46:293–298. doi: 10.1037/a0018115. [DOI] [PubMed] [Google Scholar]
- Keijsers L, Branje SJ, Hawk ST, Schwartz SJ, Frijns T, Koot HM, Meeus W, et al. Forbidden friends as forbidden fruit: Parental supervision of friendships, contact with deviant peers, and adolescent delinquency. Child Development. 2011;83:651–666. doi: 10.1111/j.1467-8624.2011.01701.x. [DOI] [PubMed] [Google Scholar]
- Keijsers L, Frijns T, Branje SJT, Meeus W. Developmental links of adolescent disclosure, parental solicitation, and control with delinquency: Moderation by parental support. Developmental Psychology. 2009;45:1314–1327. doi: 10.1037/a0016693. [DOI] [PubMed] [Google Scholar]
- Kerr M, Stattin H, Burk WJ. A reinterpretation of parental monitoring in longitudinal perspective. Journal of Research on Adolescence. 2010;20:39–64. doi: 10.1111/j.1532-7795.2009.00623.x. [DOI] [Google Scholar]
- Kobus K. Peers and adolescent smoking. Addiction. 2003;98:37–55. doi: 10.1046/j.1360-0443.98.s1.4.x. [DOI] [PubMed] [Google Scholar]
- Kodl MM, Mermelstein R. Beyond modeling: Parenting practices, parental smoking history, and adolescent cigarette smoking. Addictive Behaviors. 2004;29:17–32. doi: 10.1016/S0306-4603(03)00087-X. [DOI] [PubMed] [Google Scholar]
- Laird RD, Marrero MD. Information management and behavior problems: Is concealing misbehavior necessarily a sign of trouble? Journal of Adolescence. 2010;33:297–308. doi: 10.1016/j.adolescence.2009.05.018. [DOI] [PubMed] [Google Scholar]
- Marshall SK, Tilton-Weaver LC, Bosdet L. Information management: Considering adolescents’ regulation of parental knowledge. Journal of Adolescence. 2005;28:633–647. doi: 10.1016/j.adolescence.2005.08.008. [DOI] [PubMed] [Google Scholar]
- Mazur MA, Ebesu Hubbard AS. “Is there something I should know?”: Topic avoidant responses in parent-adolescent communication. Communication Reports. 2004;17:27–37. doi: 10.1080/08934210409389371. [DOI] [Google Scholar]
- Miller-Day MA. Parent-adolescent communication about alcohol, tobacco and other drug use. Journal of Adolescent Research. 2002;17:604–616. doi: 10.1177/074355802237466. [DOI] [Google Scholar]
- Moffitt TE. Adolescent-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review. 1993;100:674–701. doi: 10.1037/0033-295X.100.4.674. [DOI] [PubMed] [Google Scholar]
- Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology. 1996;49:1373–1379. doi: 10.1016/S0895-4356(96)00236-3. [DOI] [PubMed] [Google Scholar]
- Rutter M. Comorbidity: Concepts, claims, and choices. Behaviour and Mental Health. 1997;7:265–285. doi: 10.1002/cbm.190. [DOI] [Google Scholar]
- Sherman SJ, Chassin L, Presson C, Seo DC, Macy JT. The intergenerational transmission of implicit and explicit attitudes toward smoking: Predicting adolescent smoking initiation. Journal of Experimental Social Psychology. 2009;45:313–319. doi: 10.1016/j.jesp.2008.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smetana JG. Adolescents’ and parents’ conceptions of parental authority. Child Development. 1988;59:321–335. doi: 10.2307/1130313. [DOI] [PubMed] [Google Scholar]
- Smetana JG, Metzger A, Gettman D, Campione-Barr N. Disclosure and secrecy in adolescent–parent relationships. Child Development. 2006;77:201–217. doi: 10.1111/j.1467-8624.2006.00865.x. [DOI] [PubMed] [Google Scholar]
- Smetana JG, Villalobos M, Tasopoulos-Chan M, Gettman DC, Campione-Barr N. Early and middle adolescents’ disclosure to parents about activities in different domains. Journal of Adolescence. 2009;32:693–713. doi: 10.1016/j.adolescence.2008.06.010. [DOI] [PubMed] [Google Scholar]
- Soenens B, Vansteenkiste M, Luyckx K, Goossens L. Parenting and adolescent problem behavior: An integrated model with adolescent self-disclosure and perceived parental knowledge as intervening variables. Developmental Psychology. 2006;42:305–318. doi: 10.1037/0012-1649.42.2.305. [DOI] [PubMed] [Google Scholar]
- Stattin H, Kerr M. Parental monitoring: A reinterpretation. Child Development. 2000;71:1072–1085. doi: 10.1111/1467-8624.00210. [DOI] [PubMed] [Google Scholar]
- Talwar V, Kang L. A punitive environment fosters children’s dishonesty: A natural experiment. Child Development. 2011;82:1751–1758. doi: 10.1111/j.1467-8624.2011.01663.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tasopoulos-Chan M, Smetana JG, Yau JP. How much do I tell thee? Strategies for managing information to parents among American adolescents from Chinese, Mexican, and European backgrounds. Journal of Family Psychology. 2009;23:364–374. doi: 10.1037/a0015816. [DOI] [PubMed] [Google Scholar]
- Tilton-Weaver L, Kerr M, Pakalniskeine V, Tokic A, Salihovic S, Stattin H. Open up or close down: How do parental reactions affect youth information management? Journal of Adolescence. 2010;33:333–346. doi: 10.1016/j.adolescence.2009.07.011. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. Preventing tobacco use among young people: A report of the surgeon general. Atlanta, GA: U. S. Department of Health and Human Service, Public Health Service, Centers for Disease Control and Prevention and Health Promotion, Office on Smoking and Health; 1994. [Google Scholar]
- Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. American Journal of Epidemiology. 2007;165:710–718. doi: 10.1093/aje/kwk052. [DOI] [PubMed] [Google Scholar]
- Wakschlag LS, Chase-Lansdale PL, Brooks-Gunn J. Not just “ghosts in the nursery”: Contemporaneous intergenerational relationships and parenting in young African-American families. Child Development. 1996;67:2131–2147. doi: 10.1111/j.1467-8624.1996.tb01848.x. [DOI] [PubMed] [Google Scholar]
- Wakschlag LS, Metzger A, Darfler A, Ho J, Mermelstein R, Rathouz PJ. The Family Talk About Smoking (FTAS) paradigm: New directions for assessing parent–teen communications about smoking. Nicotine & Tobacco Research. 2011;13:103–112. doi: 10.1093/ntr/ntq217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yau JP, Tasopoulos-Chan M, Smetana JG. Disclosure to parents about everyday activities among American adolescents from Mexican, Chinese, and European backgrounds. Child Development. 2009;80:1481–1498. doi: 10.1111/j.1467-8624.2009.01346.x. [DOI] [PubMed] [Google Scholar]