

Abstract
The aim of this study was to investigate the difference in the magnitude of muscle damage between maximal eccentric exercises of the elbow flexors (EF) and knee extensors (KE). Twelve sedentary male volunteers participated in the study. Range of motion (ROM), isometric peak torque (IPT), delayed onset of muscle soreness (DOMS), creatine kinase activity (CK), and myoglobin concentration (Mb) were evaluated before, immediately after, and on the 1st , 2nd, 3rd , and 7th days following exercise. Total work (TW) during exercises was recorded and corrected by muscle volume (TWc). TWc was greater (p < 0.01) for EF [24 (2) joule·cm-3] than for KE [7 (0.4) joule·cm-3]. Increases in CK on the 2nd , 3rd , and 7th days (p < 0.01) and increases in Mb on the 1st , 2nd , 3rd , and 7th days were significantly (p<0.01) larger for EF than for KE. The decline in IPT was greater (p < 0.05- 0.01) for EF at all test occasions compared with KE. The results of this study demonstrate that the magnitude of muscle damage is greater and the recovery is slower following maximal eccentric exercise of the EF than of the KE for sedentary males.
Key points.
The magnitude of muscle damage is greater and the recovery is slower following maximal eccentric exercise of the EF than of the KE for sedentary males.
This may be because of the higher total eccentric work per muscle unit in elbow flexors.
Key words: Maximal eccentric exercise, muscle damage, creatine kinase, muscle volume.
Introduction
It is well-known that eccentric muscle actions result in muscle damage (Clarkson et al., 1992; Nosaka et al., 2002). Blood proteins, like creatine kinase and myoglobin (Nosaka and Clarkson, 1992; Sorichter et al., 1997; 1999), muscle force analyses (Nosaka and Clarkson, 1992; Nosaka et al., 2002; Paschalis et al., 2005), subjective muscle soreness (Clarkson et al., 1992; Vickers, 2001), cellular and subcellular changes in muscle ultrastructure (Friden and Lieber, 2001) and decrement in range of motion (Nosaka and Clarkson, 1992; Nosaka et al., 2002), are some of the indices that are used to assess muscle damage (Clarkson and Hubal, 2002).
In order to evaluate eccentric exercise-induced muscle damage, elbow flexors (EF) in the upper extremity and knee extensors (KE) in the lower extremity are the mostly utilized muscle groups (Clarkson and Hubal, 2002). Interestingly, the results of studies that used EF (Clarkson and Tremblay, 1988; Newham et al., 1988, Nosaka et al., 1991; Nosaka and Newton, 2002) showed more marked changes for the indicators of muscle damage than the other studies using KE (Brown et al., 1997; Dolezal et al., 2000; Prou et al., 1999; Sorichter et al., 1997; 2001). Different responses to eccentric exercise between leg and arm muscles based on the previous studies should be interpreted carefully. Probable reasons for these differences may rise from different modes of exercise, different types of muscle contraction, different intensities and number of muscle actions, and different groups of subjects.
Only one study has yet directly compared arm and leg muscles in relation to muscle damage using the same subjects to explain the different results of the previous studies on this topic (Jamurtas et al., 2005). In that study (Jamurtas et al., 2005), the same intensity of submaximal eccentric exercise was used to elicit muscle damage for EF and KE. The results of this study indicated that the magnitude of muscle damage was greater and the recovery of muscle function was slower after eccentric exercise of EF compared to KE. The authors suggested some possible explanations for the different response between arm and leg muscles. The proposed reasons were different degree of daily use, muscle architecture difference, and muscle fiber type difference. These expressions seem to be acceptable.
Differences in muscle architecture were proposed as an important factor that affects muscle damage after eccentric exercise (Friden and Lieber, 2001). This has been attributed to the fact that, in eccentric exercise, the ability to generate tension increases and a higher load is distributed among the same number of fibers, resulting in a higher load per fiber ratio (Clarkson and Hubal, 2002). Beside this, maximal eccentric exercises cause more pronounced muscle damage in contrast to submaximal eccentric exercise (Nosaka and Newton, 2002; Paschalis et al., 2005). This means that the higher the eccentric load, the higher the mechanical stress per muscle unit, and this may cause more prominent muscle damage. Because of the different architecture of arm and leg muscles (Lieber and Friden, 2000), it is probable that mechanical stress per muscle unit differs between these two muscle groups, when doing eccentric exercises of the same intensity. This can be one of the reasons for different muscle damage responses. To verify this notion and confirm the findings of the study by Jamurtas et al., 2005, it would be interesting to investigate this topic again. Because there is a closer relationship between muscle strength and muscle volume than between muscle strength and cross-sectional muscle area, it might be more appropriate to use muscle volume (Gadeberg et al., 1999) to represent the stress per muscle unit.
In the light of this information, the purpose of this study was to investigate the differences in the magnitude of muscle damage between maximal eccentric exercises of the elbow flexors and knee extensors in the same subjects.
Methods
Subjects
The subjects were comprised of 12 healthy, non-athletic, males who were not involved in a resistance-training program for at least one year before the study. Their mean ± SD (range) age, height, and body mass was 25 ± 3 (22-30) yr, 1.77 ± 0.07 (1.65-1.86) m, and 75 ± 8 (63- 94) kg, respectively. Before involvement in the study, the subjects were informed about the experimental procedures, which were in accordance with the ethical standards of the Medical School of Uludag University and of the Declaration of Helsinki, and required to complete a written informed consent document. Subjects were requested to avoid any vigorous physical activities or unaccustomed exercises, other than the ones required for the study, during the experimental period. All subjects were free from any musculoskeletal disorders and were instructed not to take any medicine or dietary supplements during the experimental period. No restrictions of diet, other than the supplementation, were imposed.
Experimental protocol
Eccentric exercise to induce muscle damage was applied to the non-dominant EF or KE randomly. To determine the non- dominant side, firstly the dominant EF (as determined by writing hand) and the dominant leg were (as determined to be the leg used to kick a soccer ball) asked to the subjects. The time between the two sessions was 2 weeks. At the pre-test, muscle volume estimation, height, weight, and isometric strength determination were done. Before and immediately after the exercise and at 1st, 2nd, 3rd, and 7th days following exercise, assessments of biochemical analysis, ROM, DOMS, and isometric peak torque (IPT) were conducted.
Muscle volume estimation
The non-dominant EF and KE were evaluated using MRI with a 1.5-Tesla superconducting magnet (Siemens, Magnetom Vision Plus, Erlangen, Germany). Scanning was performed with the subject in the supine position on a couch placed inside the gantry. Six-millimeter-thick MRI-sections for the EF and 9 mm for the KE were obtained with a conventional T1-weighted spin-echo technique (echo time, 14 ms; repetition time, 540-720 ms) axially. The gap between sections for both the EF and the KE was 1 mm. Muscular anatomy was defined in accordance with standard anatomy textbooks. Rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius were defined as the KE, and the biceps brachii (long and short head), brachialis and brachioradialis as the EF. For the KE, consecutive slices were obtained beginning from the superior anterior iliac spine and proceeding distally to the upper border of the patella. For the EF, consecutive slices were obtained beginning from the coracoid proces and proceeding distally to the lateral distal end of radius. Regions of interest (ROI) were marked manually for the EF and the KE. Each area of the axial section was multiplied with the distance between slices (10 mm for the KE and 7 mm for the EF), and the sum of the results was accepted as the muscle volume. The software of the MRI (Numaris 3 VB33D) was used to calculate the muscle volumes.
Isometric peak torque
Isometric peak torque (IPT) measurements for the EF and the KE were performed using CYBEX 6000 isokinetic dynamometer (Lumex, Inc., Ronkonkoma, USA). The subjects had two days to familiarize themselves with the exercise apparatus and testing procedures. Since of the ROM, that we use in eccentric exercise protocol (0-90 degree), angles for isometric measurement was chosen in this range as close as possible to the optimal peak torque angle for each joint.
The IPT for the EF was assessed while subjects were lying on their back. Shoulder straps, a lap belt, and a knee strap were used to limit extraneous movements. The centre of the elbow joint was aligned with the centre of the dynamometer’s power shaft. The anatomical zero was set at an elbow angle of 0 degrees (full extension). The mass of the arm was determined for every subject and the force correcting the gravitational effects on the arm mass was computed by the dynamometer’s software. The IPT was determined at an elbow angle of 60 degrees. Following three submaximal trials, four successive maximal voluntary efforts were performed for the IPT. The duration of each contraction was 5 seconds, with a rest interval of 10 seconds.
The IPT for the KE was assessed while the subjects sat on the dynamometer’s seat, with a hip angle of 90 degrees and the arms folded in front of the chest. Shoulder straps, a lap belt, a knee strap, and an ankle cuff were used to limit extraneous movements. The centre of the knee joint was aligned with the centre of the dynamometer’s power shaft. The anatomical zero was set at a knee angle of 0 degrees (full extension). The mass of the leg was determined for every subject and the force correcting the gravitational effects of the leg mass was computed by the dynamometer’s software. The IPT was determined at an angle of 60 degrees at the thigh-shin. Following three submaximal trials, four successive maximal voluntary efforts were performed for the IPT. The duration of each contraction was 5 seconds with a rest interval of 10 seconds.
Eccentric exercise protocol
The setting for each eccentric exercise was the same as the one used to determine the IPT. Both the KE and the EF were performed on the isokinetic dynamometer in the active-assistive mode (with concentric/eccentric actions) and consisted of 3 sets of 15 repetitions of eccentric actions with maximal intensity. The subjects were asked not to do an active contraction at the concentric phase of the active-assistive mode. Due to technical properties of the dynamometer that we use and sitting position of the subjects the range of motion was limited to 90 degrees for the KE (from full extension to 90° flexion). To standardize the time under tension of each muscle groups same ROM was also used for the EF (from 90° flexion to full extension) during the exercise. The angular velocity of the eccentric actions was 30°/sec for both exercises. The time under tension for each eccentric action was the same for the KE and the EF. Resting intervals between the sets were fixed at 1 min for both protocols. Work is defined as torque times angle (work = torque x angular displacement). The eccentric torque that moves the extremity from 0° to 90°, and the angular distance between this ROM was multiplied to obtain the work per repetition. Thereafter, work for each of the 15 repetitions was summed to calculate the work done in each set of the eccentric exercise protocol. These calculations for each set were made via the software of the dynamometer automatically. The total eccentric work (TW) was determined as the sum of work of the three exercise sets.
Biochemical analyses
Blood samples were drawn from the antecubital vein into plain, evacuated test tubes. The blood was allowed to clot at room temperature for 30 min and centrifuged. The serum layer was removed and frozen at -18 °C for further analyses. Serum creatine kinase (CK) activity was determined using a commercially available kit (Abbott Aeroset, USA) Normal reference range for CK is 29-200 IU/L. Myoglobin (Mb) concentration was also measured using a commercially available kit (Abbott Axsym System, USA). Normal reference range for Mb is <116.6 ng/mL.
Delayed onset of muscle soreness (DOMS)
Muscle soreness was determined by deep palpation of the muscle belly on the EF and the KE (at the distal end of the vastus medialis, vastus lateralis, and rectus femoris) and evaluated by a visual analog scale (VAS) that had a 100-mm line with “no pain” on one end and “extremely sore” on the other. During the examination the subjects lying supine on an examination table and both extremities were in a relaxed position.
Range of motion (ROM)
ROM was measured by a goniometer. ROM for the KE was performed while the subjects lay prone. Active flexion was performed slowly from a full extended position. The knee joint angle at which point the subjects reported discomfort was taken as an indication of the end of the pain-free ROM. Similarly, ROM of the EF was assessed while the subjects were lying down on their back and the elbow was moved from a fully extended position towards a fully flexed position. The elbow joint angle at which point the subjects reported discomfort was taken as an indication of the end of the pain-free ROM.
Statistical analysis
Analysis was conducted using the statistical software package, SPSS for Windows, version 9.0.0. The Shapiro-Wilk test was used to test all of the variables for normal distribution. The effectiveness and safety of the intervention is usually assessed by the change from baseline of some primary clinical endpoints. It may provide a more precise statistical inference of the intervention effects because of a reduction of variability. If the distribution of the data from the baseline is not normal, no inference about mean or variance can be made. In this case it is recommended that nonparametric methods be employed to obtain inference of the intervention effect(Chow and Liu, 2004). Due to lack of normal distribution, small number of subjects, and assessment of subjects own EF and KE the non-parametric two related samples tests (Wilcoxon signed rank test) were used. Comparisons were made between baseline and consecutive time points and between EF and KE at each time point. The percent change between pre-exercise (baseline) and consecutive time point values were calculated for the variables isometric peak torque and range of motion. The results are reported as mean and standard error of mean (SEM). P < 0.05 was considered statistically significant.
Results
Muscle volume and eccentric exercise features
Table 1 represents the muscle volume and eccentric exercise features for the EF and the KE. The muscle volume was significantly larger in the KE than in the EF. The sum of the eccentric work of the three damaging exercise sets was also significantly higher for the KE. An inverse and remarkable finding was the significantly higher values for the EF compared with the KE when the TW was corrected for muscle volume.
Table 1.
Muscle volume, total work (TW), and corrected total work (TWc) of elbow flexors (EF) and knee extensors (KE). Data are presented as means (SEM).
| EF | KE | |
|---|---|---|
| Muscle Volume (cm3) | 124 (4) ** | 1119 (47) |
| TW (joule) | 2915 (180) ** | 7341 (460) |
| TWc (joule/ cm3) | 24 (2) ** | 7 (0.4) |
** Significantly (p < 0.01) different from the KE
Plasma CK and Mb
Figure 1 shows the percent changes in CK after the EF and the KE exercises. CK levels for the EF began to increase significantly from the baseline immediately after exercise, reaching peak values on the 3rd day and still not recovering on the 7th day post-exercise. Although increases of CK levels for the KE on the 3rd day were not as high as for the EF, significant changes were observed until the 7th day from baseline. However, the EF showed significantly larger increases on the 2nd, 3rd, and 7th days post-exercise than the KE.
Figure 1.
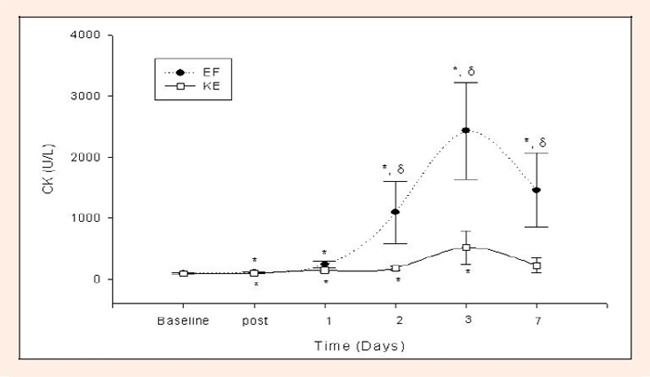
Changes in creatine kinase activity (CK) from the pre-exercise level following eccentric exercise of the knee extensors (KE) and elbow flexors (EF). * Significantly different form the baseline. δ Significantly different form KE. The symbol (•□) and their error bars denote mean and SEM.
Figure 2 shows the percent changes in Mb after the EF and the KE exercises. Mb increased significantly from the pre-exercise value on the 1st, 2nd, 3rd, and 7th days for the EF. The same was observed for the KE on the 1st, 2nd, and 3rd days, except for the 7th day. The EF showed significantly larger increases than the KE on the 1st, 2nd, 3rd, and 7th days.
Figure 2.
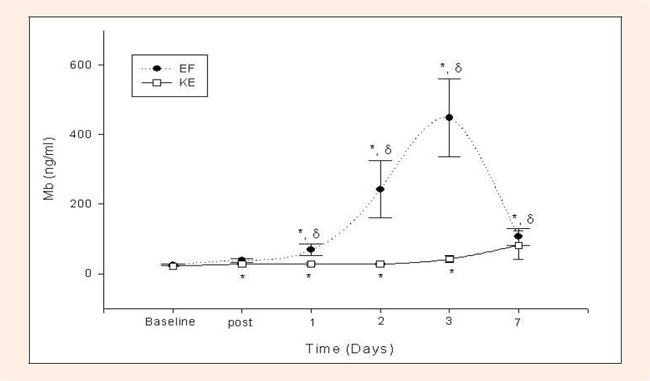
Changes in myoglobin (Mb) from the pre-exercise level following eccentric exercise of the knee extensors (KE) and elbow flexors (EF). * Significantly different form the baseline. δ Significantly different form KE. The symbol (•□) and their error bars denote mean and SEM.
Isometric peak torque
The pre-exercise IPT for the EF and the KE was 63 (4) Nm and 205 (14) Nm, respectively. As seen in Figure 3, the IPT for KE did not show a significant change following maximal eccentric exercise. Despite this, the IPT for the EF decreased and was significantly different from baseline at post-exercise, and the1st, 2nd, and 3rd days. The decrease in the IPT for the EF recovered on the 7th day. The differences in the IPT in the KE and the EF were significant for all measurement days after exercise.
Figure 3.
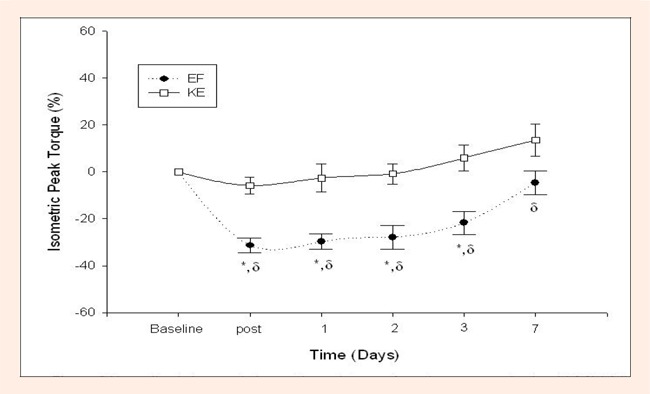
Normalized changes in isometric peak torque from the pre-exercise level (%) following eccentric exercise of the knee extensors (KE) and elbow flexors (EF). δ Significantly different form KE. The symbol (•□) and their error bars denote mean and SEM.
Range of Motion
Figure 4 shows the percent change of decreases in the ROM due to discomfort for the EF and the KE. Only the decrease for the EF was significantly different from the baseline on the 1st, 2nd, and 3rd days. A significant ROM decreased between the EF and the KE was found only on the 2nd and 3rd days.
Figure 4.
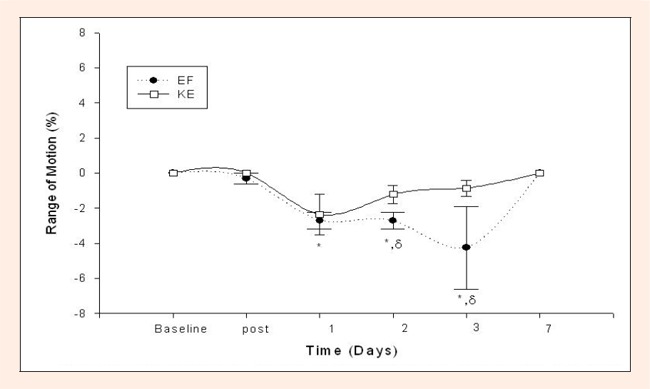
Normalized changes in range of motion from the pre-exercise level (0%) following eccentric exercise of the knee extensors (KE) and elbow flexors (EF). δ Significantly different form KE. The symbol (•□) and their error bars denote mean and SEM.
Delayed onset muscle soreness
As shown in Figure 5, DOMS developed after the 1st day, peaked on the 2nd day post-exercise, began to decrease on the 3rd day, and returned to baseline on the 7th day both for the EF and the KE. Moreover, the DOMS was significantly greater for the EF than the KE on the 2nd and the 3rd days.
Figure 5.
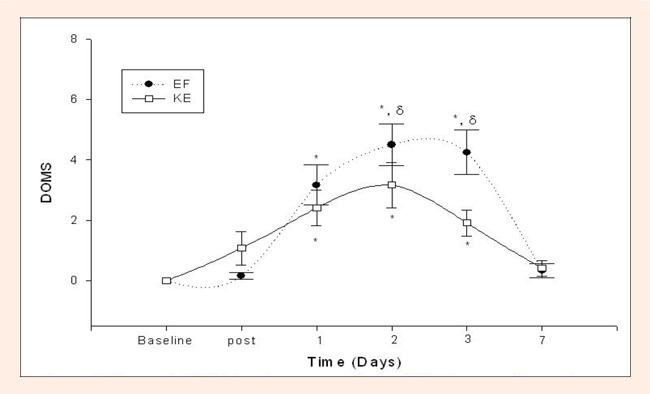
Changes in DOMS from the pre-exercise level following eccentric exercise of the knee extensors (KE) and elbow flexors (EF). δ Significantly different form KE. The symbol (•□) and their error bars denote mean and SEM.
Discussion
The results of this study showed the following after maximal eccentric exercise: 1) EF represented larger decreases and slower recovery of strength than KE, 2) the magnitude of increase in serum CK and Mb concentrations was higher in EF than in KE, 3) DOMS and discomfort in ROM were greater for EF than for KE, 4) and TWc, which was determined with muscle volume, was greater for EF than for KE,
The results of the present study were consistent with the studies that used either arm or leg muscle exercises. For instance, the amount of increase in CK activity in the blood was greater following eccentric exercise of the EF (Cleak and Eston, 1992; Lee et al., 2002; Newham et al., 1987; Nosaka and Newton, 2002; Nosaka et al., 2002; Rodenburg et al., 1993) than in leg exercises, such as downhill running (Byrnes et al., 1985; Schwane et al., 1983; Sorichter et al., 2001) and isolated KE eccentric exercise (Brown et al., 1997; Byrne and Eston, 2002; Prou et al., 1999; Serrao et al., 2003). DOMS also appeared to be greater following a bout of eccentric exercise performed with EF (Clarkson and Tremblay, 1988; Cleak and Eston, 1992; Lee et al., 2002; Newham et al., 1988; Nosaka et al., 2002; Rodenburg et al., 1993) than for leg exercises (Brown et al., 1996; Byrnes et al., 1985; Dolezal et al., 2000; Gleeson et al., 1998; Prou et al., 1999; Schwane et al., 1983). Furthermore, the recovery of muscular performance seemed to be slower following an exercise bout performed with arm muscles (Kawakami et al., 1995; Nosaka et al., 1991; 2002) than with legs (Brown et al., 1997; Byrne and Eston, 2002; Serrao et al., 2003). However, differences in exercise intensity, time, mode, and contraction type should be taken into account as factors affecting different muscle injury responses in these studies. In order to control the influence of these factors, Jamurtas et al., 2005 tested this observation in the same subject using the same relative intensity eccentric exercise model. Our results were also consistent in some measures with those of the above study; the course of muscle damage indicators, such as blood protein markers and muscle force following eccentric exercise, was greater for EF than for KE. The magnitude and course of blood protein markers of the muscle damage in our study were similar for the KE and the EF as in the study of Jamurtas et al., 2005. Their results for the force loss and recovery after eccentric exercise overlapped with our results. But in our study, the decrease in isometric force for KE after eccentric exercise was not statistically significant. Probably, the ROM that we use during eccentric exercise may be the reason for the different observation. The fibers of the EF muscles were fully stretched during the eccentric exercise, whereas the KE muscles were not stretched equally to same length due to the sitting position of the subjects on the isokinetic dynamometer.
In contrast to the results of Jamurtas et al., 2005, the decrease in ROM and increase in DOMS were significantly different between the KE and the EF following the eccentric exercise bout in our study. Possible explanations for different observations in DOMS and ROM exist. We measured ROM actively from an extended to a flexed position for both joints using a manual goniometer. Jamurtas et al., 2005 measured it passively and on an isokinetic dynamometer from an extended to a flexed position for the KE and vice versa for the EF. The determination of DOMS was different in some points. They measured DOMS by self-palpation in a seated position for the KE and in a relaxed position for the EF. However, we measured it in a relaxed position in each of the muscle groups. This may be the reason why they could not find a significant difference between the KE and the EF. Contraction, stretching, and palpation are factors that can supposedly affect the sensation of pain when evaluating DOMS (Proske and Allen, 2005). Especially, the time under tension during the eccentric contraction is an important factor that can affect the magnitude of muscle damage (Lieber and Friden, 2000; Proske and Allen, 2005). The time under tension during the eccentric contractions for the elbow flexors and knee extensors was 2.2 and 2.0 sec, respectively, in the study of Jamurtas et al., 2005, but we standardized it to 3 seconds for both muscle groups. The inequality of the times during the contractions could be one reason for the different responses. Additionally, we must take into account that subjectively measured DOMS is a variable that is not accurate (Nosaka et al., 2002; Rodenburg et al., 1993) as other objective outcome parameters, like muscle force drop (Clarkson and Hubal, 2002).
Jamurtas et al., 2005 stated that submaximal eccentric loading during daily activities, like downhill walking and going downstairs, is a routine training stimulus for KE , and the same is less valid for EF. It is well-known that after a bout of eccentric exercise the muscles adapt themselves and protect against further damage following repeated bouts of eccentric exercise (Clarkson and Hubal, 2002; Proske and Allen, 2005). From this point of view, the suggestion of Jamurtas et al., 2005 may be acceptable. In contrast, in the study of Brown et al., 1997, the force loss after a maximal eccentric exercise was about 40% and the elevation of serum proteins, like CK, was moderately high (2815 ± 4144 IU/L) for KE and was not small when compared with the study by Jamurtas et al., 2005 and our results. Possible reason for this observation could be that the training effect of daily routine activities is not enough to prevent leg muscles from eccentric exercise-induced muscle damage. Even individuals in excellent athletic condition may experience muscle soreness and damage when performing exercise (Friden and Lieber, 2001), which is new to them. Furthermore, in the study by Vincent and Vincent, 1997, muscle soreness was detected higher in trained athletes than in untrained controls and the force drop was found similar between groups after a strenuous resistance exercise. In respect of these findings, the opinion that the difference in daily utilization of arm and leg muscles as a cause for different magnitude of muscle damage is not sufficient.
Another explanatory reason for the different muscle damage response between the arm and leg muscles may be the muscle fiber distribution. It has been generally accepted that type II muscles fibers are more susceptible to eccentric exercise-induced muscle damage compared to type I fibers (Friden and Lieber, 2001). The muscle fiber composition of the biceps brachii mainly consists of type II muscle fibers (Klein et al., 2003), whereas the KE consist of type I muscle fibers (Travnik et al., 1995). In respect of these studies, the opinion, that muscle fiber distribution may be a factor affecting the magnitude of muscle damage could be acceptable. Since these two studies investigated only one muscle area or group in the subjects, the results of these studies should be carefully interpreted. Studies have shown that people with a predominance of slow twitch fibers in their leg muscles will likely have a higher percentage of slow-twitch fibers in their arm muscles as well. A similar relationship exists for fast-twitch fibers (Clarkson et al., 1982; Flynn et al., 1987; Tesch and Karlsson, 1985; Wilmore and Costill, 2004). Therefore, the opinion that the difference in muscle fiber distribution between the arm and leg muscles has an effect on the muscle damage response is somewhat under debate. Moreover, neither in the study of Jamurtas et al., 2005 nor in our study muscle biopsies was obtained. This argument, however, is no more than speculation.
A valid explanation for the difference in the magnitude of muscle damage between the arm and leg muscles after an eccentric exercise could be the difference in the muscle architecture of these two muscle groups. EF (i.e., biceps) is mostly composed of fibers that extend parallel to the muscle’s force-generating axis and are described as fusiform architecture. On the other hand, KE muscles have fibers with an angular orientation relative to the force generating axis and are described as having a pennate architecture (Lieber and Frieden, 2000). Pennate muscles, like KE, with large physiological cross-sectional areas have probably lower specific tension (or mechanical strain) per muscle unit as compared to fusiform muscles, like EF, during a maximal voluntary contraction. According to this theory, an eccentric exercise with maximal intensity probably causes more prominent muscle damage in the EF than in the KE. In our study, the specific tension per muscle unit (which was determined by total eccentric work/muscle volume) was approximately 3.7 times greater for the EF than for the KE. Our opinion for the difference in eccentric load per muscle volume may be the result of the muscle architectural difference between elbow flexors and knee extensors. Because of closer relationship between maximal muscle strength and muscle volume (Gadeberg et al., 1999), the muscle volume was used as a determinant to represent the specific tension per muscle unit in this study .Since it provides data about the entire range of motion during eccentric contractions, total eccentric work was also used in this study to reflect the specific tension to which the whole muscle is exposed to.
This study has some minor limitations. Firstly, the number of subjects was small. Secondly, it has been shown that the muscle length is one of the factors to determine the magnitude of muscle damage (Nosaka and Sakamoto, 2001). In the present study, the fibers of the EF muscles were fully stretched during the eccentric exercise. Whereas the KE muscles were not stretched equally to same length due to the sitting position of the subjects on the isokinetic dynamometer.
Conclusion
In conclusion, the results of this study demonstrate that the magnitude of muscle damage is greater and the recovery is slower following maximal eccentric exercise of the EF than of the KE for sedentary males. This may be because of the higher total eccentric work per muscle unit in elbow flexors. To clarify the differences in course and magnitude of muscle damage response after eccentric exercises more precisely, further studies are needed that are designed to include various muscle groups, exercise forms, and intensity in the same subjects.
Acknowledgments
This study was supported by the Department of the Scientific Research Projects of Uludag University (Project# T- 2004/11).
Biographies
Tolga Saka
Employment
Ass. Prof., Department of Sports Medicince, Erciyes University, Kayseri
Degree
MD
Research interests
Muscle damage.
E-mail: tolgasakamd@gmail.com

Bedrettin Akova
Employment
Associate Professor, Department of Sports Medicine, Medical Faculty of Uludag University, Bursa, Turkey.
Degree
MD
E-mail: bakova@uludag.edu.tr
Zeynep Yazici
Employment
Prof., Department of Radiology Medical Faculty of Uludag University, Bursa, Turkey.
Degree
MD
Ufuk Sekir
Employment
Associate Professor, Department of Sports Medicine, Medical Faculty of Uludag University, Bursa, Turkey.
Degree
MD
E-mail: sekir@gmail.com

Hakan Gür
Employment
Prof., Department of Sports Medicine, Medical Faculty of Uludag University, Bursa, Turkey.
Degree
MD, PhD
Research interests
Isokinetic and exercise, muscle damage and exercise.
E-mail: hakan@uludag.edu.tr

Yesim Ozarda
Employment
Associate Professor, Department of Biochemistry, Medical Faculty of Uludag University, Bursa, Turkey
Degree
MD
Research interests
Reference values, choline metabolism and free fatty acids
E-mail: yesim@uludag.edu.tr
References
- 1.Brown S.J., Child R.B., Donnelly A.E., Saxton J.M., Day S.H. (1996) Changes in human skeletal muscle contractile function following stimulated eccentric exercise. European Journal of Applied Physiology and Occupational Physiology, 72, 515-521 [DOI] [PubMed] [Google Scholar]
- 2.Brown S.J., Child R.B., Day S.H., Donnelly A.E. (1997) Indices of skeletal muscle damage and connective tissue breakdown following eccentric muscle contractions. European Journal of Applied Physiology and Occupational Physiology, 75, 369-374 [DOI] [PubMed] [Google Scholar]
- 3.Byrnes W.C., Clarkson P.M., White J.S., Hsieh S.S., Frykman P.N., Maughan R.J. (1985) Delayed onset muscle soreness following repeated bouts of downhill running. Journal of Applied Physiology, 59, 710-715 [DOI] [PubMed] [Google Scholar]
- 4.Byrne C., Eston R. (2002) Maximal-intensity isometric and dynamic exercise performance after eccentric muscle actions. Journal of Sports Sciences, 20, 951-959 [DOI] [PubMed] [Google Scholar]
- 5.Chow S.C., Liu J.P. (2004) Baseline comparisons. : Design and analysis of clinical trials. 2nd edition Wiley-Interscience; 512-516 [Google Scholar]
- 6.Clarkson P.M., Kroll W., Melchionda A.M. (1982) Isokinetic strength, endurance, and fiber type composition in elite American paddlers. European Journal of Applied Physiology and Occupational Physiology 48, 67-76 [DOI] [PubMed] [Google Scholar]
- 7.Clarkson P.M., Tremblay I. (1988) Exercise-induced muscle damage, repair and adaptation in humans. Journal of Applied Physiology, 65, 1-6 [DOI] [PubMed] [Google Scholar]
- 8.Clarkson P.M., Nosaka K., Braun B. (1992) Muscle function after exercise-induced muscle damage and rapid adaptation. Medicine and Science in Sports and Exercise, 24, 512-520 [PubMed] [Google Scholar]
- 9.Clarkson P.M., Hubal M.J. (2002) Exercise-induced muscle damage in humans. American Journal of Physical Medicine & Rehabilitation 81, 52-69 [DOI] [PubMed] [Google Scholar]
- 10.Cleak M.J., Eston R.G. (1992) Muscle soreness, swelling, stiffness and strength loss after intense eccentric exercise. British Journal of Sports Medicine, 26, 267-272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dolezal B.A., Potteiger J.A., Jacobsen D.J., Benedict S.H. (2000) Muscle damage and resting metabolic rate after acute resistance exercise with an eccentric overload. Medicine and Science in Sports and Exercise, 32, 1202-1207 [DOI] [PubMed] [Google Scholar]
- 12.Flynn M.G., Costill D.L., Kirwan J.P., Fink W.J., Dengel D.R. (1987) Muscle fiber composition and respiratory capacity in triathletes. International Journal of Sports Medicine, 8, 383-386 [DOI] [PubMed] [Google Scholar]
- 13.Friden J., Lieber R.L. (2001) Eccentric exercise-induced injuries to contractile and cytoskeletal muscle fibre components. Acta Physiologica Scandinavica, 171, 321-326 [DOI] [PubMed] [Google Scholar]
- 14.Gadeberg P., Andersen H., Jakobsen J. (1999) Volume of ankle dorsiflexors and plantar flexors determined with stereological techniques. Journal of Applied Physiology 86, 1670-1675 [DOI] [PubMed] [Google Scholar]
- 15.Gleeson M., Blannin A.K., Walsh N.P., Field C.N., Pritchard J.C. (1998) Effect of exercise-induced muscle damage on the blood lactate response to incremental exercise in humans. European Journal of Applied Physiology and Occupational Physiology, 77, 292-295 [DOI] [PubMed] [Google Scholar]
- 16.Jamurtas A.Z., Theocharis V., Tofas T., Tsiokanos A., Yfanti C., Paschalis V., Koutedakis Y., Nosaka K. (2005) Comparison between leg and arm eccentric exercises of the same relative intensity on indices of muscle damage. European Journal of Applied Physiology, 95, 179-185 [DOI] [PubMed] [Google Scholar]
- 17.Kawakami Y., Abe T., Kuno S.Y., Fukunaga T. (1995) Training-induced changes in muscle architecture and specific tension. European Journal of Applied Physiology and Occupational Physiology 72, 37-43 [DOI] [PubMed] [Google Scholar]
- 18.Klein C.S., Marsh G.D., Petrella R.J., Rice C.L. (2003) Muscle fiber number in the biceps brachii muscle of young and old men. Muscle & Nerve, 28, 62-68 [DOI] [PubMed] [Google Scholar]
- 19.Lee J., Goldfarb A.H., Rescino M.H., Hegde S., Patrick S., Apperson K. (2002) Eccentric exercise effect on blood oxidative-stress markers and delayed onset of muscle soreness. Medicine and Science in Sports and Exercise, 34, 443-448 [DOI] [PubMed] [Google Scholar]
- 20.Lieber R.L., Friden J. (2000) Functional and clinical significance of skeletal muscle architecture. Muscle & Nerve, 23, 1647-1666 [DOI] [PubMed] [Google Scholar]
- 21.Newham D.J., Jones D.A., Ghosh G., Aurora P. (1988) Muscle fatigue and pain after eccentric contractions at long and short length. Clinical Science (London, England: 1979) 774, 553-557 [DOI] [PubMed] [Google Scholar]
- 22.Newham D.J., Jones D.A., Clarkson P.M. (1987) Repeated high-force eccentric exercise: effects on muscle pain and damage. Journal of Applied Physiology, 63, 1381-1386 [DOI] [PubMed] [Google Scholar]
- 23.Nosaka K., Clarkson P.M., McGuiggin M.E., Byrne J.M. (1991) Time course of muscle adaptation after high force eccentric exercise. European Journal of Applied Physiology, 63, 70-76 [DOI] [PubMed] [Google Scholar]
- 24.Nosaka K., Clarkson P.M. (1992) Relationship between post-exercise plasma CK elevation and muscle mass involved in the exercise. International Journal of Sports Medicine, 13, 471-475 [DOI] [PubMed] [Google Scholar]
- 25.Nosaka K., Sakamoto K. (2001) Effect of elbow joint angle on the magnitude of muscle damage to the elbow flexors. Medicine and Science in Sports and Exercise, 33, 22-29 [DOI] [PubMed] [Google Scholar]
- 26.Nosaka K., Newton M., Sacco P. (2002) Muscle damage and soreness after endurance exercise of the elbow flexors. Medicine and Science in Sports and Exercise, 34, 920-927 [DOI] [PubMed] [Google Scholar]
- 27.Nosaka K., Newton M. (2002) Difference in the magnitude of muscle damage between maximal and submaximal eccentric loading. Journal of Strength and Conditioning Research 16, 202-208 [PubMed] [Google Scholar]
- 28.Paschalis V., Koutedakis Y., Jamurtas A.Z., Mougios V., Baltzopoulos V. (2005) Equal volumes of high and low intensity of eccentric exercise in relation to muscle damage and performance. Journal of Strength and Conditioning Research, 19, 184-188 [DOI] [PubMed] [Google Scholar]
- 29.Proske U., Allen T.J. (2005) Damage to skeletal muscle from eccentric exercise. Exercise and Sport Sciences Reviews, 33, 98-104 [DOI] [PubMed] [Google Scholar]
- 30.Prou E., Guevel A., Benezet P., Marini J.F. (1999) Exercise-induced muscle damage: absence of adaptive effect after a single session of eccentric isokinetic heavy resistance exercise. The Journal of Sports Medicine and Physical Fitness, 39, 226-232 [PubMed] [Google Scholar]
- 31.Rodenburg J.B., Bar P.R., De Boer R.W. (1993) Relations between muscle soreness and biochemical and functional outcomes of eccentric exercise. Journal of Applied Physiology 74, 2976-2983 [DOI] [PubMed] [Google Scholar]
- 32.Schwane J.A., Johnson S.R., Vandenakker C.B., Armstrong R.B. (1983) Delayed-onset muscular soreness and plasma CPK and LDH activities after downhill running. Medicine and Science in Sports and Exercise, 15, 51-56 [PubMed] [Google Scholar]
- 33.Serrao F.V., Foerster B., Spada S., Morales M.M., Monteiro-Pedro V., Tannus A., Salvini T.F. (2003) Functional changes of human quadriceps muscle injured by eccentric exercise. Brazilian Journal of Medical and Biological Research 36, 781-786 [DOI] [PubMed] [Google Scholar]
- 34.Sorichter S., Mair J., Koller A., Gebert W., Rama D., Calzolari C., Dworzak E.A., Puschendorf B. (1997) Skeletal troponin I as a marker of exercise-induced muscle damage. Journal of Applied Physiology 83, 1076-1082 [DOI] [PubMed] [Google Scholar]
- 35.Sorichter S., Puschendorf B., Mair J. (1999) Skeletal muscle injury induced by eccentric muscle action: muscle proteins as markers of muscle fiber injury. Exercise Immunology Review, 5, 5-21 [PubMed] [Google Scholar]
- 36.Sorichter S., Mair J., Koller A., Calzolari C., Huonker M., Pau B., Puschendorf B. (2001). Release of muscle proteins after downhill running in male and female subjects. Scandinavian Journal of Medicine & Science in Sports 11, 28-32 [DOI] [PubMed] [Google Scholar]
- 37.Tesch P.A., Karlsson J. (1985) Muscle fiber types and size in trained and untrained muscles of elite athletes. Journal of Applied Physiology 59, 1716-1720 [DOI] [PubMed] [Google Scholar]
- 38.Travnik L., Pernus F., Erzen I. (1995) Histochemical and morphometric characteristics of the normal human vastus medialis longus and vastus medialis obliquus muscles. Journal of Anatomy, 187, 403-411 [PMC free article] [PubMed] [Google Scholar]
- 39.Vickers A.J. (2001) Time course of muscle soreness following different types of exercise. BMC Musculoskeletal Disorders 2, 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Vincent H.K., Vincent K.R. (1997) The effect of training status on the serum creatine kinase response, soreness and muscle function following resistance exercise. International Journal of Sports Medicine, 18, 431-437 [DOI] [PubMed] [Google Scholar]
- 41.Wilmore J.H., Costill D.L. (2004) Muscles and have they move. : Physiology of sport and exercise.: Wilmore J.H., Costill D.L.3rd edition Hong Kong: Human Kinetics; 31-57 [Google Scholar]