

Abstract
The aim of this study was to determine the prevalence of self- reported versus diagnosed stress fractures in female elite athletes and non-athletic controls. A random sample of Norwegian elite athletes from the national teams, aged 13-39 years (n = 186) and a random sample of non-athletic controls (n = 145) in the same age group participated in the study. The athletes represented a junior- or senior team, or a recruiting squad for one of these teams, in one of 46 different sports/events. A higher percentage of athletes self-reported stress fractures (14.0%) compared to those diagnosed with stress fractures (8.1%) (p < 0.001). Six controls self- reported stress fractures, but none of them were diagnosed with stress fractures. These results indicate that self-reporting of stress fractures has low validity. This finding has important implications for further research on stress fractures in athletes.
Key points.
This study is the first to compare self-reported and diagnosed stress fractures in the total population of elite athletes representing all kinds of sports.
The results indicate that self-reporting of stress fractures has low validity in both athletes and non-athletic controls, and other measurement methods should be considered when evaluating possible stress fractures.
Based on our results, stress fractures seem to be a sport-related injury.
Key words: Imaging, sports, injuries, validity
Introduction
The prevalence of stress fractures among female athletes ranges from 4% to 52% (Barrow and Saha, 1988; Bennell et al., 1995; 1996b, Johnson et al., 1994; Nattiv et al., 1997; Pecina et al., 1990; Torstveit and Sundgot-Borgen, 2005b; Warren et al., 1986). A number of factors can influence the interpretation of these results, such as study design, diagnostic and clinical definitions of stress fracture, sampling methods, sample size, the length of the observation period, and different sports/events (Brukner et al., 1999). The term “stress fracture ”may be unfamiliar to people in general, and even to some athletes and coaches. Athletes experiencing sport related pain may assume that the injury is a stress fracture, and they may even be told the same by others, such as coaches, leaders or health personnel. However, it is important to diagnose the pain or injury properly to avoid mistreatment and further interruptions from training and competition. Differencing the diagnosis of stress fractures from other injuries may be difficult. Differential diagnoses to stress fractures include tendon inflammation, degenerative change, muscle- or tendon injury, and compartment syndrome. Tumours and infections can also mimic stress fractures (Brukner et al., 1999; Pommering and Kluchurosky, 2007). Thus, thorough physical examinations and imaging seems necessary for adequate diagnosis of stress fractures (Moran et al., 2008). Still, many studies on female athletes use self-reported stress fracture data (Barrow and Saha, 1988; Bennell et al., 1995; Brunet et al., 1990; Cameron et al., 1992; Micklesfield et al., 2007; Pecina et al., 1990; Warren et al., 1986; Dubravcic-Simunjak et al., 2008), and to our knowledge, no studies have compared self-reported stress fractures with diagnosed stress fractures in athletes. Furthermore, even if stress fractures are seen upon as a sport-related injury, also physically active non-elite athletes may theoretically experience such injury. A sudden increase in exercise volume, such as changing the lifestyle from inactive to moderately active, may cause injuries often seen in elite athletes (Fahlstrom et al., 1998; Nilsson, 1982). However, there is a lack of information regarding the occurrence of stress fractures in the general population. The aims of this study were therefore to determine the prevalence of self-reported versus diagnosed stress fractures in athletes, and to investigate whether stress fractures are prevalent also in the general population.
Methods
Subjects
All female elite athletes on the Norwegian national teams (aged 13-39 years, n = 938), and non-athletic controls (aged 13-39 years, n = 900) were invited to participate. Permission to conduct the study was provided by the Data Inspectorate and the Regional Committee for Medical Research Ethics, the Norwegian Olympic Committee and the Norwegian Confederation of Sports.
An elite athlete was defined as one who qualified for one of the national teams. Exclusion criteria were pregnancy with a plan to discontinue the athletic career after delivery, participation in two different sport groups, or an injury which had prevented the athlete from training and competing for more than three months. A Norwegian Bureau of Statistics randomly selected a sample of 900 subjects from the entire population of Norwegian female citizens aged 13-39 years. Every county was represented and an identical perceptual age and geographical distribution in relation to the total population was accounted for. Exclusion criteria were severe illness and unfamiliarity with the Norwegian language, and competing in sports at the national team level.
Assessment procedures
Screening
A detailed questionnaire was sent to each of the 938 athletes and 900 controls. The questionnaire included questions regarding training, physical activity, menstrual function, eating disorders, stress fractures, and use of oral contraceptives. The question asking for a history of stress fracture was as follows; have you ever had one or more stress fractures? The response rate was 88.3% for the athletes and 70.2% for the controls. Based on data from the questionnaire, a random sample of athletes (n = 300) and controls (n = 300) was selected. This sample was stratified based on age-group and “risk-profile ”for the female athlete triad (Torstveit and Sundgot-Borgen, 2005b). The risk criteria were low BMI (< 18.5 kg·m-2), high score on subtests of the Eating Disorder Inventory, use of pathogenic weight control methods, menstrual dysfunction and stress fractures. A total of 186 athletes (62%) and 145 controls (48%) participated in this study. The athletes (n = 186) represented 46 different sports, which were divided into three groups based upon the degree of mechanical loading: Low-impact (LI), medium- impact (MI), and high-impact (HI) sports (Table 1). These selection processes is explained elsewhere (Torstveit and Sundgot-Borgen, 2005a).
Table 1.
Classification of 46 sports (n = 186) divided into three groups based on the degree of mechanical loading in the sports. Data are given as numbers.
| LI-sports (n = 38) | MI-sports (n = 51) | HI-sports (n = 97) |
|---|---|---|
| Underwater rugby (n = 12) | Field hockey (n = 8) | Rhythmic gymnastics (n = 16) |
| Swimming (n = 6) | Orienteering (n = 8) | Gymnastics (n = 16) |
| Cycling (n = 4) | Middle- and long-distance running (n = 6) | Soccer (n = 17) |
| Bowling (n = 3) | Sports dance (n = 4) | Team Handball (n = 14) |
| Horse riding (dressage) (n = 3) | Sailing (n = 3) | Basketball (n = 6) |
| Climbing (n = 3) | Rowing (n = 3) | Volleyball (n = 6) |
| Shooting (n = 3) | Cross-country skiing (n = 3) | Badminton (n = 3) |
| Dog racing (n = 2) | Ski-orienteering (n = 2) | Track and field (jumping events) (n = 4) |
| Billiard (n = 1) | Table tennis (n = 2) | Track and field (sprint events) (n = 4) |
| Curling (n = 1) | Biathlon (n = 2) | Power lifting (n = 2) |
| Race walking (n = 2) | Speed skaiting (sprint) (n = 2) | |
| Kickboxing (n = 1) | Alpine skiing (n = 1) | |
| Karate (n = 1) | Figure skating (n = 1) | |
| Judo (n = 1) | Telemark skiing (n = 1) | |
| Long-distance speed skating (n = 1) | Freestyle (n = 1) | |
| Paddling (n = 1) | Tennis (n = 1) | |
| Wrestling (n = 1) | Icehockey (n = 1) | |
| Triathlon (n = 1) | ||
| Track and field (throwing events) (n = 1) |
Assessment of the prevalence of stress fractures
The athletes and the controls who reported “yes” (n = 32), “I don't know ”(n = 29), or “no ”(n = 270) to the question regarding experience of a stress fracture in the questionnaire, participated in an interview in order to verify their self-reported answer. The diagnosis of a stress fracture was based on their patient history and physical examination. All these participants were asked to confirm their past stress fracture by plain radiography, nuclear scintigraphy, computed tomography (CT), magnetic resonance imaging (MRI), or a combination of these modalities taken short time after their injury occurred. If the scan was positive, the participants were diagnosed with a stress fracture. If the participants had not taken any x-ray of their injury, they were classified as false positive subjects and not diagnosed with a stress fracture. Thus, all athletes and controls had to verify their answer to the stress fracture question in the questionnaire by positive findings on their x-rays pictures to be diagnosed with a stress fracture.
Definitions
Training volume
Total training volume for the athletes was defined as the mean of total hours of training and competition per week during the previous year. Amount of physical activity among the controls was defined as the mean of total hours of physical activity per week including physical education lessons, recreational sports and active daily living such as walking, during the previous year.
Statistical analysis
All analyses were performed using SPSS software for windows, version 15.0 (SPSS Inc, Chicago, Illinois). The descriptive results are expressed as mean values and Standard Deviation (SD). Comparisons between athletes and controls were carried out using independent sample T-tests for continuous data. Chi-square tests (McNemar’s test) were utilized to investigate the difference between the subjects who self-reported stress fractures in the questionnaire, and the same subjects who were diagnosed with stress fractures in the interview. P-values <0.05 were considered statistically significant.
Results
Subject characteristics
The athletes were younger and had a lower Body Mass Index (BMI) compared with the non-athletic controls (Table 2). The total training volume for the athletes was 14.0 (5.6) hours/week, and the total amount of physical activity for the controls was 4.7 (4.4) hours/week.
Table 2.
Anthropometric data for the athletes (n = 186) and the non-athletic controls (n = 145). Data are given as means (SD).
| Athletes | Controls | |
|---|---|---|
| Age (years) | 22.2 (5.8) | 29.6 (7.9) *** |
| Height (m) | 1.68 (.07) | 1.66 (.06) ** |
| Weight (kg) | 61.5 (8.7) | 66.4 (12.3) *** |
| BMI (kg/m²) | 21.7 (2.4) | 24.0 (4.2) *** |
| Fat percentage (%)† | 24.2 (7.2) | 35.4 (7.1) *** |
† Measured by Dual-energy x-ray absorptiometry (DXA).
** and *** denote p < 0.01 and 0.001, respectively.
Prevalence of stress fractures
A higher percentage of athletes (n = 186) self-reported stress fractures (n = 26) (14.0%) compared to those who had stress fractures diagnosed by clinical criteria (n = 15) (8.1%) (p < 0.001). Six controls (n = 145) (4.1%) self- reported stress fractures, but none of them were diagnosed with stress fractures (Figure 1).
Figure 1.
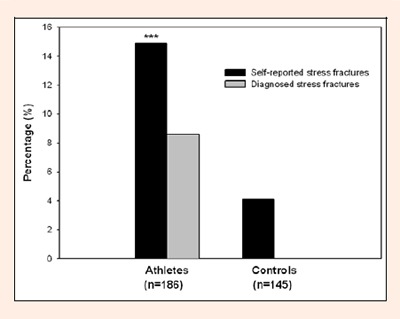
Percentage of athletes and controls with self-reported and diagnosed stress fractures. *** p < 0.001 compared with self-reported stress fractures.
A total of 8.1% of the athletes self-reported stress fractures, and were also diagnosed with stress fractures, while 5.9% of the athletes self- reported stress fractures, but were not diagnosed with stress fractures.
None of the participants who reported “no ”or “I don't know ”to the question regarding experience of a stress fracture in the questionnaire was diagnosed with stress fractures.
The total training volume was higher for the athletes diagnosed with stress fractures (17.0 ± 5.8 hours/week) compared with the athletes without diagnosed stress fractures (13.0 ± 5.5 hours/week) (p < 0.05).
Nine of the 15 athletes diagnosed with stress fractures represented HI sports, while six represented MI sports. None of the athletes diagnosed with stress fractures represented LI sports. Eight of the 15 stress fractures were found in the metatarsals (Table 3). Among the athletes without stress fractures (n = 171), 38 were classified into LI sports, 40 into MI sports and 93 into HI sports.
Table 3.
Site specificity, imaging and sports for the athletes diagnosed with stress fractures (n = 15). Data are given as numbers.
| Events | Metatarsal | Tibia/Fibula | Femur | Lumbar spine | Os pubis | Imaging |
|---|---|---|---|---|---|---|
| Soccer (HI) | 1 | 1 | S. P/CT | |||
| Team handball (HI) | 1 | P/S/CT | ||||
| Field hockey (MI) | 1 | P | ||||
| Speed skaiting (sprint) (HI) | 1 | P | ||||
| Cross-country skiing (MI) | 1 | S | ||||
| Track and field (throwing events) (MI) | 1 | P | ||||
| Track and field (sprint events) (HI) | 2 | S | ||||
| Middle- and long-distance running (MI) | 1 | P | ||||
| Orienteering (MI) | 1 | S/MRI | ||||
| Gymnastics (HI) | 1 | P/MRI | ||||
| Rhythmic gymnastics (HI) | 1 | P | ||||
| Sports dance (MI) | 1 | P | ||||
| Figure skating (HI) | 1 | S/MRI | ||||
| Total | 8 | 2 | 2 | 2 | 1 |
HI = High impact sports; MI = Medium impact sports. S = Scintigraphy, P = Plain radiography, CT = Computertomografi, MRI = Magnetic resonance imaging.
Reasons for over-reporting
In terms of reasons for over-reporting a stress fracture, 11 of the athletes and 13 of the controls explained that they were unfamiliar with the term stress fracture, while five of the athletes and two of the controls had other injuries. Among the athletes, four explained that the physiotherapist claimed it was a stress fracture (Table 4).
Table 4.
Reasons for over-reporting among the participants who reported “yes” and “I don’t know” in the questionnaire. Data are given as numbers.
| Athletes (n = 27) | Controls (n = 19) | |||
|---|---|---|---|---|
| Yes | Uncertain* | Yes | Uncertain* | |
| Unfamiliar with the term stress fractures | 4 | 7 | 3 | 10 |
| Other injuries | 4 | 1 | 2 | - |
| Acute fractures | 1 | 2 | 1 | 1 |
| The injury was not diagnosed by imaging | 1 | 3 | - | 2 |
| The physiotherapist claimed it was a stress fracture | 1 | 3 | - | - |
* Answered “I don’t know” to the question regarding experience of a stress fracture in the questionnaire.
Discussion
To our knowledge, this study is the first to compare self-reported stress fractures and diagnosed stress fractures within the same population. Fourteen percent of the athletes self-reported stress fractures, while only 8.1% were diagnosed with stress fractures. This indicates a low validity regarding self-reporting of such injuries. Apart from the study design, a number of factors can influence interpretation of the results, such as diagnostic and clinical definitions of stress fracture, confounding factors, sample size, sampling methods, length of the stress fracture observation period, and different sports/events (Brukner et al., 1999). In most of the studies published on the occurrence of stress fractures, only one or two different sports are investigated (Barrow and Saha, 1988; Bennell et al., 1995; 1996b, Brunet et al., 1990; Frusztajer et al., 1990; Pecina et al., 1990; Warren et al., 1986; Dubravcic-Simunjak et al., 2008). The athletes in our study represented 46 different sports, and it is therefore difficult to directly compare the results. However, our self-reported data are in occurrence with a study by Brunet et al., 1990 where 13.2% of competitive runners self-reported the prevalence of stress fractures. On the other hand, in three other studies on self-reported stress fractures, where the diagnostic methods are not stated, the prevalence was higher (21.0%, 25.0% and 26.6%) (Nattiv et al., 1997, Pecina et al., 1990, Cameron et al., 1992). Even higher numbers has been found in collegiate distance runners 37.0% (Barrow and Saha, 1988) and ballet dancers 45.0% (Warren et al., 1986). Furthermore, Bennell et al., 1995 found the self-reported prevalence rate to be as high as 51.5% among female track and field athletes. These athletes reported that their stress fracture was diagnosed by imaging, but this was not investigated further and are therefore not comparable with our result. The high prevalence found in these retrospective studies (Barrow and Saha, 1988, Bennell et al., 1995, Warren et al., 1986) may be due to the specific sport investigated and/or over-reporting of stress fractures. Two prospective studies show an annual incidence of athletes diagnosed with stress fractures at 6.9% (Johnson et al., 1994) and 21.7% (Bennell et al., 1996b). In the study by Bennell et al., 1996b, track and fields sports were the main events, while Johnson et al., 1994 investigated athletes competing in different kind of sports. In both studies the athletes were followed by observation and the stress fractures were diagnosed by imaging. The latter study is therefore somewhat comparable to our results based on diagnostic method and athletes competing in a variety of sports. Johnson et al., 1994 investigated 321 female athletes participating in 12 different kinds of sports. During a two-year follow-up, 22 stress fractures were found, and the most common site was tibia (n = 9). In contrast, we found that only two of our 15 athletes diagnosed with stress fractures had stress fractures in tibia or fibula, and more than half of the athletes (n = 8) had stress fractures in metatarsals. Only four athletes were diagnosed with metatarsal fractures in the study by Johnson et al., 1994. Furthermore, it should be mentioned that 64% (n = 14) of the athletes with stress fractures in Johnson et al’ s (1994) study competed in track and field events, while only 20% (n = 3) of the athletes with stress fractures in our study competed in track and field events.
Studies have found that especially track and field athletes have a high prevalence of stress fractures (Bennell and Crossley, 1996; Johnson et al., 1994). We found that our athletes with stress fractures represented a variety of sports. However, when we divided our sports into sport groups based on mechanical loading (Torstveit and Sundgot-Borgen, 2005a), we found that nine athletes diagnosed with stress fractures competed in HI-sports, six in MI-sports, and none in LI-sports. In accordance with our results, Bennell et al., 1995 found that of 22 stress fractures half of the athletes represented HI-sports and the second half represented MI-sports. These findings are also supported by Edwards et al., 2008. Due to the external weight impact on each bone, it is expected that high mechanical loading can be a risk factor for stress fractures (Bennell and Brukner, 1997; Brukner et al., 1999). On the other hand, mechanical loading has a positive effect on BMD (Heinonen et al., 1995, Vuori, 2001), but studies investigating the association between low BMD and stress fractures have contradictory findings (Bennell et al., 1995; 1996a; 2004; Carbon et al., 1990; Frusztajer et al., 1990; Kelsey et al., 2007; Marx et al., 2001; Vinther et al., 2006).
By using a questionnaire to collect data, the results consist of what the subjects report that they have experienced or have not experienced (Sundgot-Borgen, 1994; Sundgot-Borgen and Torstveit, 2004). In our study, 42.3% of the athletes were classified as false positive subjects (b/(a+b) = 11/26). Thus, our results indicate that self-reporting of stress fractures has low validity among female elite athletes. In terms of reasons for the over-reporting of stress fractures, it is important to note that eight of the athletes who falsely self-reported a stress fracture thought their injury (acute fracture or other injuries) was a stress fracture. Additionally, as many as four of the athletes who falsely self-reported stress fracture, were told by their physiotherapist that their injury was a stress fracture. This finding underlines the need for education and information even to health personnel working with athletes in order for them to give the best treatment methods.
Even if many of our controls representing the general population had a low BMD (Torstveit and Sundgot-Borgen, 2005a), and 4.1% of the controls self- reported a stress fracture, none of them were diagnosed with stress fractures. Thus, all of our non- athletic controls were classified as false positives. The association between low BMD and fractures are well known among postmenopausal women with osteoporosis (Melton et al., 1993), but this association has not been confirmed in premenopausal women. Furthermore, a stress fracture is normally seen upon as a sports-related injury (Khan et al., 2001), and to our knowledge studies in this area pertain to athletes (Barrow and Saha, 1988; Bennell et al., 1995; 1996b; Cameron et al., 1992; Dubravcic-Simunjak et al., 2008; Johnson et al., 1994; Kelsey et al., 2007; Mattila et al., 2007; Nattiv et al., 1997; Pecina et al., 1990; Torstveit and Sundgot-Borgen, 2005a; Warren et al., 1986) and military populations (Bijur et al., 1997; Jones et al., 1993; Milgrom et al., 1994; Montgomery et al., 1989; Rutherford, 1993). Our findings support the assumption that stress fractures are a problem related to athletes competing in sports and not to generally physically active females.
Conclusion
A higher percentage of athletes self-reported stress fractures compared to those who had stress fractures diagnosed by clinical criteria. Fifteen of the athletes and none of the controls were diagnosed with stress fractures. These results indicate that self-reporting of stress fractures have low validity and that stress fractures are a sport related injury. We recommend that future studies in this field should be carefully using self-reporting as a measurement method.
Acknowledgement
We would like to thank Professor Ingar Holme for statistical advice and Kristine Austgulen for English revision of the manuscript.
Biographies
Jannike Øyen
Employment
Department of Surgical Sciences, Faculty of Medicine and Dentistry, University of Bergen, Bergen, Norway.
Degree
MSc., PhD student.
Research interests
Osteoporosis, Bone health, fractures, physical activity and health.
E-mail: jannike.oyen@kir.uib.no
Monica Klungland Torstveit
Employment
Department of Public Health, Faculty of Health & Sport, University of Agder, Kristiansand, Norway.
Degree
PhD, Assistant Professor.
Research interests
Osteoporosis, bone health, physical activity and health, eating disorders.
E-mail: monica.k.torstveit@uia.no
Jorunn Sundgot-Borgen
Employment
Norwegian School of Sport Sciences, Oslo, Norway.
Degree
PhD, Professor.
Research interests
Eating disorders, physical activity and health, osteoporosis, bone health.
E-mail: jorunn.sundgot-borgen@nih.no
References
- Barrow G.W., Saha S. (1988) Menstrual irregularity and stress fractures in collegiate female distance runners. The American Journal of Sports Medicine, 16, 209-16 [DOI] [PubMed] [Google Scholar]
- Bennell K., Crossley K., Jayarajan J., Walton E., Warden S., Kiss Z. S., Wrigley T. (2004) Ground reaction forces and bone parameters in females with tibial stress fracture. Medicine & Science in Sports & Exercise, 36, 397-404 [DOI] [PubMed] [Google Scholar]
- Bennell K.L., Brukner P.D. (1997) Epidemiology and site specificity of stress fractures. Clinical Journal of Sports Medicine, 16, 179-96 [DOI] [PubMed] [Google Scholar]
- Bennell K. L., Crossley K. (1996) Musculoskeletal injuries in track and field: incidence, distribution and risk factors. Australian Journal of Medical Science, 28, 69-75 [PubMed] [Google Scholar]
- Bennell K. L., Malcolm S. A., Thomas S. A., Ebeling P. R., Mccrory P. R., Wark J. D., Brukner P.D. (1995) Risk factors for stress fractures in female track-and-field athletes: a retrospective analysis. Clinical Journal of Sports Medicine, 5, 229-35 [DOI] [PubMed] [Google Scholar]
- Bennell K. L., Malcolm S. A., Thomas S. A., Reid S. J., Brukner P. D., Ebeling P. R., Wark J. D. (1996a) Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. The American Journal of Sports Medicine, 24, 810-8 [DOI] [PubMed] [Google Scholar]
- Bennell K. L., Malcolm S. A., Thomas S. A., Wark J. D., Brukner P. D. (1996b) The incidence and distribution of stress fractures in competitive track and field athletes. A twelve-month prospective study. The American Journal of Sports Medicine, 24, 211-7 [DOI] [PubMed] [Google Scholar]
- Bijur P. E., Horodyski M., Egerton W., Kurzon M., Lifrak S., Friedman S. (1997) Comparison of injury during cadet basic training by gender. Archives of Pediatrics & Adolescent Medicine, 151, 456-61 [DOI] [PubMed] [Google Scholar]
- Brukner P., Bennell K., Matherson G. (Eds.) (1999) Stress fractures, Australia, Blackwell Science Asia Pty Ltd [Google Scholar]
- Brunet M. E., Cook S. D., Brinker M. R., Dickinson J. A. (1990) A survey of running injuries in 1505 competitive and recreational runners. Journal of Sports Medicine and Physical Fitness, 30, 307-15 [PubMed] [Google Scholar]
- Cameron K., Telford R., Wark J. (1992) Stress fractures in Australian competitive runners. Australian Sports Medicine Federation Annual Scientific Confererence in Sports Medicine. Perth, Australia. [Google Scholar]
- Carbon R., Sambrook P. N., Deakin V., Fricker P., Eisman J. A., Kelly P., Maguire K., Yeates M. G. (1990) Bone density of elite female athletes with stress fractures. The Medical Journal of Australia, 153, 373-6 [DOI] [PubMed] [Google Scholar]
- Dubravcic-Simunjak S., Moran H., Pecina M., Šimunjak B., Ambartsumov R., Sakai H., Mitchel D., Shobe J. (2008) Stress fracture prevalence in elite figure skaters. Journal of Sports Science and Medicine, 7, 2. [PMC free article] [PubMed] [Google Scholar]
- Edwards W. B., Gillette J. C., Thomas J. M., Derrick T. R. (2008) Internal femoral forces and moments during running: Implications for stress fracture development. Clinical Biomechanics, 23, 1269-78 [DOI] [PubMed] [Google Scholar]
- Fahlstrom M., Bjornstig U., Lorentzon R. (1998) Acute badminton injuries. Scandinavian Journal of Medicine and Science in Sports, 8, 145-8 [PubMed] [Google Scholar]
- Frusztajer N. T., Dhuper S., Warren M. P., Brooks-Gunn J., Fox R. P. (1990) Nutrition and the incidence of stress fractures in ballet dancers. The American Journal of Clinical Nutrition, 51, 779-83 [DOI] [PubMed] [Google Scholar]
- Heinonen A., Oja P., Kannus P., Sievanen H., Haapasalo H., Manttari A., Vuori I. (1995) Bone mineral density in female athletes representing sports with different loading characteristics of the skeleton. Bone, 17, 197-203 [DOI] [PubMed] [Google Scholar]
- Johnson A. W., Weiss C. B., JR. & Wheeler D. L. (1994) Stress fractures of the femoral shaft in athletes--more common than expected. A new clinical test. The American Journal of Sports Medicine, 22, 248-56 [DOI] [PubMed] [Google Scholar]
- Jones B. H., Bovee M. W., Harris J. M., 3RD, Cowan D. N. (1993) Intrinsic risk factors for exercise-related injuries among male and female army trainees. The American Journal of Sports Medicine, 21, 705-10 [DOI] [PubMed] [Google Scholar]
- Kelsey J. L., Bachrach L. K., Procter-Gray E., Nieves J., Greendale G. A., Sowers M., Brown B. W., JR. Matheson, K. A. Crawford, S. L., Cobb K. L. (2007) Risk factors for stress fracture among young female cross-country runners. Medicine & Science in Sports & Exercise, 39, 1457-63 [DOI] [PubMed] [Google Scholar]
- Khan K., Mckay H., Kannus P. (Eds.) (2001) Physical activity and bone health, USA, Human Kinetics [Google Scholar]
- Marx R. G., Saint-Phard D., Callahan L. R., Chu J., Hannafin J. A. (2001) Stress fracture sites related to underlying bone health in athletic females. Clinical Journal of Sports Medicine, 111, 73-6 [DOI] [PubMed] [Google Scholar]
- Mattila V. M., Niva M., Kiuru M., Pihlajamaki H. (2007) Risk factors for bone stress injuries: a follow-up study of 102,515 person-years. Medicine & Science in Sports & Exercise, 39, 1061-6 [DOI] [PubMed] [Google Scholar]
- Melton L. J., 3RD, Atkinson E. J., O'Fallon W. M., Wahner H. W., Riggs B. L. (1993) Long-term fracture prediction by bone mineral assessed at different skeletal sites. Journal of Bone and Mineral Research, 88, 1227-33 [DOI] [PubMed] [Google Scholar]
- Micklesfield L. K., Hugo J., Johnson C., Noakes T. D., Lambert E. V. (2007) Factors associated with menstrual dysfunction and self-reported bone stress injuries in female runners in the ultra- and half-marathons of the Two Oceans. British Journal of Sports Medicine, 41, 679-83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milgrom C., Finestone A., Shlamkovitch N., Rand N., Lev B., Simkin A., Wiener M. (1994) Youth is a risk factor for stress fracture. A study of 783 infantry recruits. The Journal of Bone & Joint Surgery (Br), 776, 20-2 [PubMed] [Google Scholar]
- Montgomery L. C., Nelson F. R., Norton J. P., Deuster P. A. (1989) Orthopedic history and examination in the etiology of overuse injuries. Medicine & Science in Sports & Exercise, 21, 237-43 [PubMed] [Google Scholar]
- Moran D. S., Evans R. K., Hadad E. (2008) Imaging of lower extremity stress fracture injuries. Sports Medicine, 38, 345-56 [DOI] [PubMed] [Google Scholar]
- Nattiv A., Puffer J. C., Green G. A. (1997) Lifestyles and health risks of collegiate athletes: a multi-center study. Clinical Journal of Sports Medicine, 7, 262-72 [DOI] [PubMed] [Google Scholar]
- Nilsson S. (1982) Jogging injuries: an overview. Scandinavian Journal of Social Medicine, 29, 171-8 [PubMed] [Google Scholar]
- Pecina M., Bojanic I., Dubravcic S. (1990) Stress fractures in figure skaters. The American Journal of Sports Medicine, 18, 277-9 [DOI] [PubMed] [Google Scholar]
- Pommering T. L., Kluchurosky L. (2007) Overuse injuries in adolescents. Adolescent Medicine: State of the Art Reviews, 118, 95-120 [PubMed] [Google Scholar]
- Rutherford O. M. (1993) Spine and total body bone mineral density in amenorrheic endurance athletes. Journal of Applied Physiology, 74, 2904-8 [DOI] [PubMed] [Google Scholar]
- Sundgot-Borgen J. (1994) Risk and trigger factors for the development of eating disorders in female elite athletes. Medicine & Science in Sports & Exercise, 226, 414-419 [PubMed] [Google Scholar]
- Sundgot-Borgen J., Torstveit M. K. (2004) Prevalence of eating disorders in elite athletes is higher than in the general population. Clinical Journal of Sports Medicine, 14, 25-32 [DOI] [PubMed] [Google Scholar]
- Torstveit M. K., Sundgot-Borgen J. (2005a) The female athlete triad exists in both elite athletes and controls. Medicine & Science in Sports & Exercise, 337, 1449-59 [DOI] [PubMed] [Google Scholar]
- Torstveit M. K., Sundgot-Borgen J. (2005b) The female athlete triad: are elite athletes at increased risk? Medicine & Science in Sports & Exercise, 337, 184-93 [DOI] [PubMed] [Google Scholar]
- Vinther A., Kanstrup I. L., Christiansen E., Alkjaer T., Larsson B., Magnusson S. P., Ekdahl C., Aagaard P. (2006) Exercise-induced rib stress fractures: potential risk factors related to thoracic muscle co-contraction and movement pattern. Scandinavian Journal of Medicine and Science in Sports, 16, 188-96 [DOI] [PubMed] [Google Scholar]
- Vuori I. M. (2001) Dose-response of physical activity and low back pain, osteoarthritis, and osteoporosis. Medicine & Science in Sports & Exercise, 333, 551-86 [DOI] [PubMed] [Google Scholar]
- Warren M. P., Brooks-Gunn J., Hamilton L. H., Warren L. F., Hamilton W. G. (1986) Scoliosis and fractures in young ballet dancers. Relation to delayed menarche and secondary amenorrhea. The New England Journal of Medicine, 314, 1348-53 [DOI] [PubMed] [Google Scholar]