

Abstract
Physical exercise is used for the promotion and maintenance of good health and for the improvement of physical fitness. Both endurance and resistance exercises are needed to carry out a complete training program. Because time may be a barrier to physical exercise practice, the aim of this study was to verify whether the order of execution of endurance and resistance exercises, in concurrent training, has different effects on the metabolic responses during recovery. Thirteen healthy women [24.40 (1.67) years, Mean (SD)] were investigated for energy expenditure (EE), oxygen consumption (VO2), ventilation (Ve), respiratory frequency (RF), proportion of oxygen in expired air (FeO2) and ratings of perceived exertion (RPE) both before and after three concurrent endurance and resistance trainings, carried out in different orders: endurance-resistance training (ERT), resistance-endurance training (RET) and alternating endurance-resistance training (AERT). AERT elicited a significantly greater increase of EE, VO2, and Ve and a greater decrease of FeO2. ERT elicited a lower increase of RPE. Acute post-exercise physiological responses to concurrent endurance and resistance physical exercise seem to depend on the order of execution of the two parts: among the selected protocols, AERT seems to elicit the best responses.
Key points.
The concurrent execution of both endurance and resistance exercise, in the same training session, could be a practical solution to conform to guidelines for health in the presence of lack of time.
The order of concurrent execution of both endurance and resistance exercise, in the same training session, influences the amplitude of some post-exercise physiological responses.
Key words: EPOC, FeO2, exercise order, endurance exercise, resistance exercise
Introduction
It is well known that at the end of an exercise session, oxygen consumption remains elevated above resting levels, declining progressively, together with a lower respiratory exchange ratio (RER). These phenomena have been attributed to excess post-exercise oxygen consumption (EPOC) and to a greater use of free fatty acids as energy supply (Gaesser and Brooks, 1984) respectively: physical exercise elicits fat-powered energy expenditure in the post-exercise phase at a higher level than in the pre-exercise phase. The duration and rate of EPOC and RER are related to and influenced by the level of physical fitness and intensity of physical exercise, together with the timing, extent and kind of exercise performed (Braun et al., 2005). The optimization of metabolic responses to physical exercise is obtained through the optimization of the exercise prescription (Braun et al., 2005; Frey et al., 1993; Gillette et al., 1994) taking into account also environmental effects and the sex of the subject (Fukuba et al., 2000; Matsuo et al., 1999).
According to the guidelines for whole-body physical fitness conditioning and exercise prescriptions for health, both endurance and resistance exercises should be included in training programs with a frequency of up to three and two times a week, respectively (Haskell et al., 2007); therefore conforming with these guidelines could be expensive in terms of time. In fact, among the barriers that could influence compliance with a physical exercise program, the lack of time is frequently reported, showing an inverse correlation with age, and was negatively associated with overall physical activity (Moschny et al., 2011). As a consequence, the concurrent execution of both endurance and resistance exercise, in the same training session, should be a practical solution to conform to these guidelines, both in physical fitness training (ACSM, 2006) and athletic program (Drummond et al., 2005; Haddock et al., 2006). As reported by Villaca Alves and colleagues (2011), the use of concurrent endurance and resistance exercise may also serve to improve space and time management procedures in fitness facilities; it also provides an additional way to reduce the monotony of training.
The training sequence of endurance and resistance exercise, at least in theory, could influence acute physiological responses: indeed, while the sequence seems to have no effects on absolute or relative VO2, heart rate and RER during exercise; post-exercise VO2 seems to be affected by the order of concurrent endurance and resistance exercise (Villaca Alves et al., 2011). Post-exercise VO2 was significantly greater when endurance exercise was performed before resistance exercise in several (Drummond et al., 2005; Villaca Alves et al., 2011) but not all studies: Oliveira and Oliveira, 2011 found that the order of execution did not affect the EPOC magnitude and duration. To the best of our knowledge, the literature is lacking in studies conducted on healthy but non-trained women that investigate the acute effects of all of the possible combinations of concurrent endurance and resistance training.
The aim of the study was to investigate whether the sequence of execution of endurance and resistance exercises, during the same session, significantly affected post-exercise resting energy expenditure (REE), oxygen consumption (VO2), ventilation (Ve), respiratory frequency (RF), and proportion of oxygen in the expired air (FeO2) in healthy women who had not previously undertaken such exercise programs (‘non-trained’ women).
Methods
Participants
Non-trained, healthy women from the Chieti-Pescara metropolitan area (Abruzzo, central-southern region of Italy), who belonged to a local social and cultural association, were recruited and participated in this study. A screening interview and a clinical visit excluded eleven ineligible persons. Therefore thirteen subjects were enrolled in the study [mean age 24.40 (SD 1.67) years; body mass index, i.e. BMI, 21.28 (1.64) Kg·m-2].
The eligibility criteria for this study were aimed at identifying subjects without endocrine, cardiovascular, pulmonary and orthopedic disorders, with a BMI in the range of normality (18. 5<BMI<25 Kg·m-2), and not participating in any program dealing with physical exercise and/or dietetic restriction. Also a regular menstrual cycle and the absence of stimulating and inhibitory drugs, dietary supplementation and smoking were requested.
Volunteers who satisfied the above inclusion/exclusion criteria gave their informed consent, in accordance with procedures approved by the Helsinki Committee.
Study protocol
The study was designed and conducted by the Laboratory of Medicine and Sports Cardiology of the University Centre of Sports Medicine of the "G. d’Annunzio" University (Chieti-Pescara, Italy).
All subjects underwent a careful clinical examination, anthropometry and body composition assessment, and preliminary endurance and resistance testing before the execution of the experimental training protocols. During all the phases of study, the laboratory conditions were controlled for temperature (21-23 °C) and humidity (50%) (ACSM, 2006). All the preliminary tests and experimental training protocols were executed during the early to mid-follicular phase of the subjects’ menstrual cycle (days 1-7) (Braun et al., 2005).
Anthropometry and body composition
Body weight and stretched stature were measured to the nearest 0.1 kg and 0.1 cm, respectively, with the subjects dressed in light clothing and without shoes (Marfell-Jones et al., 2006), using a stadiometer with a balance-beam scale (Seca 220, Seca, Hamburg, Germany). The body mass index was calculated according to the formula of body weight/stature2 (Kg·m-2).
To exclude that the variation of muscle mass could affect the recorded variables of the continuous indirect calorimetry, body composition was assessed. The body composition was assessed using an electrical bioimpedance technique, on a foot-to-foot 50 kHz frequency bioelectrical impedance scale (BC-420MA, Tanita, Tokyo, Japan). The error margin in impedance measurement of the body composition analyzer is ± 2%, corresponding to a change of approximately ± 0.5% in the body fat measurement of a person of a regular figure. The test was performed three hours after getting up and after voiding; with the subject in an upright position, barefoot and without conductive garments.
Preliminary testing
Preliminary testing for endurance exercises included the assessment of participants’ maximal heart rate through a graded stress test (i.e. Bruce protocol) on a treadmill (770 CE, RAM, Padua, Italy), under continuous electrocardiogram monitoring and step-by-step blood pressure measurements (ACSM, 2006). Maximal heart rate minus basal heart rate, measured after 10 minutes of reclined rest before starting the graded stress test, gave the reserve heart rate of each participant.
Preliminary testing for resistance exercises included the determination of the weight corresponding to the one-repetition maximum (1-RM) of the exercised muscle groups (Kraemer and Fry, 1995). Each participant completed three sessions of light lifting in order to become familiarized with the exercises, prior to the tests, on the following machines of myShape circuit (Teca srl, Ortona, Italy): ABDOMINAL ROM, GLUTEUS PRESS ROM, SP 100 LEG EXTENSION, ABDUCTOR ROM, ADDUCTOR ROM (Teca srl, Ortona, Italy). A flat bench, barbell, and dumbbells were also used.
The endurance and resistance tests were performed in the same week with one resting day in between. Participants presented in the morning, 4 hours after a standardized breakfast, without having performed maximal muscle exertion the day before and abstaining from caffeine and alcohol for the preceding 12 hours. The meal was 400 kcal (Compher et al., 2006) and consisted of 33 cl of water, 35 cl of orange juice and two 30 g energy bars (Power Sport Double Use, Enervit, Milan, Italy).
Experimental training protocols
The participants were scheduled to come to the laboratory soon after waking in the morning, 4 hours after the standardized breakfast and after avoiding vigorous exercise and alcohol consumption during the preceding 24 h. Dietary and physical activity records were collected for the three days preceding the first experimental training protocol and participants were requested to follow the same meal plan over the three days preceding the second and the third experimental training protocols.
Upon arrival at the laboratory, each participant’s body composition was assessed and baseline resting metabolic data (T0) collected. Resting EE, VO2, Ve, RF, and FeO2 were collected for 30 minutes via continuous indirect calorimetry (FitMate Pro, Cosmed, Roma, Italy) with the subjects in total rest and in a reclined position in a standardized and quiet room (Compher et al., 2006). Data collected during minutes 15 to 30 of the rest period were averaged and used to represent the resting metabolic data. Participants underwent a new metabolic assessment immediately after each training protocol. Each participant performed all three training protocols, while the order of their execution was randomly assigned.
Protocol 1: Concurrent endurance-resistance training (ERT). In the concurrent endurance-resistance training, endurance training preceded resistance training (Figure 1). Thirty minutes of endurance exercise was performed at 60% ± 5 bpm of the subject’s HRR on a treadmill (T1T, Teca srl, Ortona, Italy). If the heart rate went above/below to the established range of training the speed of treadmill was lowered/increased. The endurance session was preceded and followed by five minutes of warm-up and cool-down. Two minutes after the endurance phase, the resistance phase was performed. Participants were engaged in circuit training including eight stations of myShape circuit (Teca) organized as follows: ABDOMINAL ROM, bent over lateral raises, GLUTEUS PRESS ROM, bench press, LEG EXTENSION ROM, barbell curls, ABDUCTOR ROM, ADDUCTOR ROM. The exercises were performed at 55% of 1-RM; the stations were used consecutively and a 30-second transition time was provided between each station. We chose the use of 55% of 1-RM because it allows working for 30-second consecutively: circuit training, composed by stations lasting 30-second, is a widely used modality of resistance training among women. The resistance circuit was repeated three times with a recovery of two minutes between each repetition. An exercise trainer supervised the trainings and recorded the ratings of perceived exertion (RPE), using the RPE scale (Borg, 1998), before the beginning of the training (T0), at the end of the endurance phase (T1), before the beginning of the resistance phase (T2) and at the end of it (T3). Five minutes after the end of the training (T4) RPE was again recorded. The subtraction of RPE recorded at T0 to that recorded at T4 gave the variation of RPE. The participants were familiarised with the RPE scale before the beginning of the study (Borg, 1998). We have chosen to record also the RPE to verify whether the experimental training protocols affected both objective (e.g. VO2) and subjective (i.e. RPE) variables.
Figure 1.
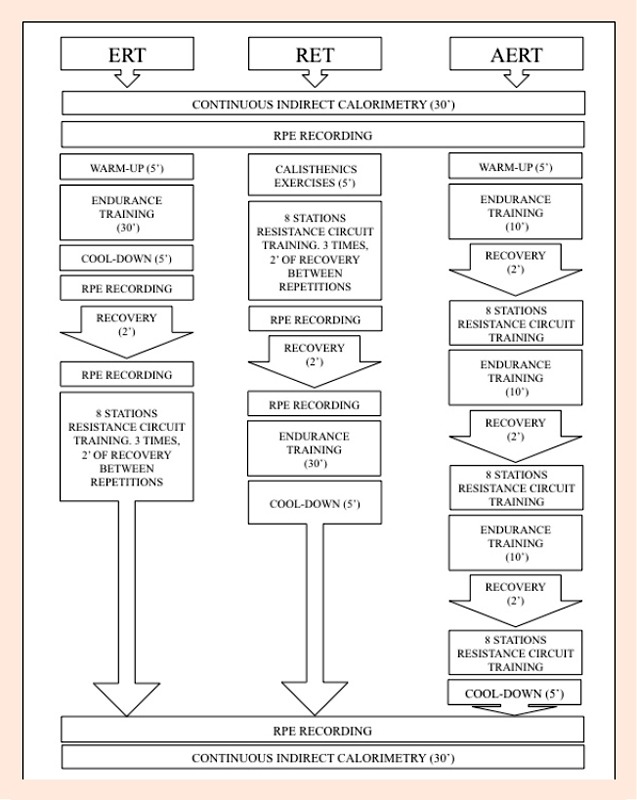
Experimental training protocols. ERT = concurrent endurance-resistance training; RET = concurrent resistance-endurance training; AERT = concurrent alternated endurance-resistance training.
Protocol 2: Concurrent resistance-endurance training (RET). Protocol 2 differed from protocol 1 only in the order of execution and the warm-up: the resistance phase was followed by the endurance phase and the warm-up was executed through five minutes of whole body calisthenics exercises. Ratings of perceived exertion were recorded following the same scheme applied to Protocol 1 (Figure 1).
Protocol 3: Concurrent alternated endurance-resistance training (AERT). Protocol 3 was characterized by five minutes of warm-up on the treadmill followed by ten minutes of endurance exercise alternated with one repetition of the resistance circuit. This combination was repeated three times in order to reach 30 minutes of endurance exercise and three circuits of the eight stations of resistance exercise (Figure 1). Each endurance phase was separated from each resistance phase by two minutes of recovery. The last repetition of the resistance circuit was followed by five minutes of cool-down on the treadmill. Ratings of perceived exertion were recorded only at T0 and T4.
Statistical analysis
Data were analyzed using STATA 10 software (StataCorp LP, College Station, USA) and their normal distribution was verified before statistical analysis. One-way analysis of variance (ANOVA) was used to assess systematic differences in body composition and basal metabolic parameters among the three training protocols. One-way analysis of variance was also used to compare the variation (∆) of each variable according to sub-group membership. Bonferroni post-hoc analysis was also performed. The ∆ of each variable was calculated subtracting the pre-training value from that recorded post-training. Data are presented as mean (standard deviation) and statistical significance was set at p ≤ 0.05.
Results
The mean age of the study group was 24.40 (1.67) years, while the BMI was 21.28 (1.64) Kg·m-2; as could be expected, the percentage of fat mass and total body water were in the range of normality for age and sex [respectively: 22.60 (0.54); 56.64 (0.61)]. The body composition of the participants did not change during the three months of study. The participants’ basal values of EE, VO2, Ve, RF and Fe O2 were not different according to the training protocols (Table 1). Training protocols elicited significantly different effects on the following variables: EE (p = 0.006), VO2 (p = 0. 005), Ve (p = 0.013), and FeO2 (p = 0.05) (Figure 2). Post-hoc analysis showed that AERT elicited a significantly greater increase of EE, VO2 and Ve, but there was no difference between ERT and RET (Figure 2). The concentration of Fe O2 was higher in ERT and lower in RET and AERT; the responses elicited by RET and AERT were not different, although they differed with respect to ERT (Figure 2). Concurrent endurance-resistance training (i.e. ERT) elicited a significantly lower increase of RPE with respect to the other protocols, which did not differ between themselves (p < 0.001) (Figure 3).
Table 1.
Comparison of investigated variables recorded before each protocol. Data are means (±SD).
| ERT* | RET† | AERT§ | P | |
|---|---|---|---|---|
| EE|| (kcal) | 1495.23 (86.77) | 1433.69 (72) | 1438.07 (65.75) | .60 |
| VO2¶ (ml·min-1) | 198.76 (39.33) | 195.07 (37.53) | 195.69 (37.49) | .90 |
| Ve** (l·min-1) | 6.5 (.63) | 6.07 (1.08) | 6.24 (.86) | .40 |
| RF †† | 18.18 (1.23) | 17.25 (1.91) | 17.22 (1.96) | .20 |
| FeO2§§ (%) | 17.04 (.50) | 16.94 (.60) | 17.04 (.50) | .80 |
| RPE ¶¶ | 6 (0) | 6 (0) | 6 (0) | 1 |
*concurrent endurance-resistance training
†concurrent resistance-endurance training
§concurrent alternated endurance-resistance training
||energy expenditure
¶oxygen consumption
**ventilation
††respiratory frequency
§§proportion of oxygen in the expired air
¶¶ratings of perceived exertion
Figure 2.
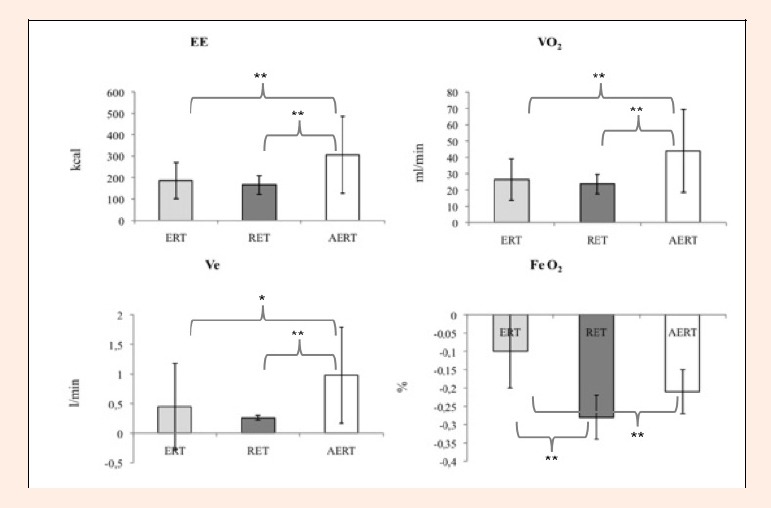
Effects of protocols of training on the variations of the physiological investigated variables. ERT = concurrent endurance-resistance training; RET = concurrent resistance-endurance training; AERT = concurrent alternated endurance-resistance training; EE= energy expenditure; VO2 = oxygen consumption; Ve = ventilation; FeO2 = oxygen fraction in the expired air; * 0.01< p ≤ 0.05; ** p ≤ 0.01.
Figure 3.
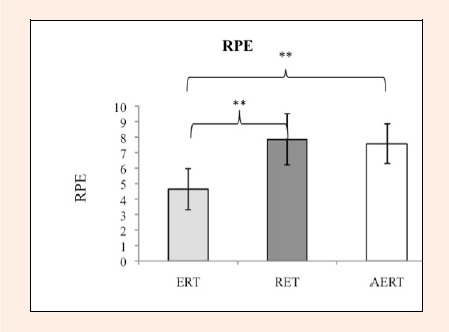
Effects of protocols of training on the variations of ratings of perceived exertion.
ERT = concurrent endurance-resistance training; RET = concurrent resistance-endurance training; AERT = concurrent alternated endurance-resistance training; RPE = ratings of perceived exertion; ** p ≤ 0.01.
Discussion
The major finding of the study was that the organization of a concurrent endurance and resistance training affects the metabolic responses of non-trained women. An important starting point was the standardization of the research. In this study the confounding effects of participants’ lifestyle, as well as the paraphysiological changes due to the estroprogestinic cycle could be deemed to be minimized due to the standardization of both caloric intake, and scheduling of the exercise tests with respect to the menstrual cycle of each participant (Fukuba et al., 2000; Matsuo et al., 1999; Oosthuyse and Bosch, 2010). Indeed, it is well known that dietary habits can influence indirect calorimetry (Compher et al., 2006) and physical performance (American Dietetic Association et al., 2009) through both quality and quantity of nutrients consumed. As literature does not report univocal opinion about the role of the menstrual cycle phase on EPOC (Fukuba et al., 2000; Matsuo et al., 1999) and as a significant variation in metabolic rate, during menstrual cycle, has been reported (i.e. increasing during the luteal phase) (Henry et al., 2003; Solomon et al., 1982), we have chosen to standardize protocols executions, with respect to the menstrual cycle phase, to reduce the possible confounding factors of our results. Adding that, exercise protocols, not differing for total volume, duration and intensity, centered the attention on the effects of the organization of endurance and resistance sessions during post-exercise recovery.
This study found that AERT, compared with the other protocols, induced a higher metabolic rate by increasing EE, VO2, Ve and RPE during recovery from training, and independently of their pre-test values. Literature explains post-exercise higher values of EE, VO2 and Ve, with respect to their pre-exercise values, as physiological responses, to physical engagement, to support the adenosine triphosphate/creatine phosphate resynthesis, the replenishment of glycogen and oxygen stores, lactate removal, and increased body temperature and circulation (Borsheim and Bahr, 2003). In the same time, also post-exercise sustained Ve is cause of EE and VO2 because of the mechanical action of ventilation must be supported energetically.
The proportion of oxygen in the expired air was also been found to be affected by the organization of concurrent training. The concentration of exhaled oxygen reflects the amount of oxygen used in metabolic processes and it is comparable to RER. The greater reduction of FeO2 elicited by AERT and RET, compared with ERT, reflects what is represented by RER because the reduction of FeO2 indirectly represents the increase of carbon dioxide, the dividend of the RER. The reduction of the RER, or the reduction of the FeO2, may represent the increase in fat oxidation. Indeed, Bahr and colleagues (1990) estimated that TG/FA cycling might account for as much as half of the energy cost during the delayed component of EPOC and earlier investigations has also shown RER to fall below baseline measures during recovery from exercise. They concluded that the lower RER values during recovery from high-intensity exercise versus moderate-intensity exercise could be attributable to a higher rate of fat oxidation rather than to replenishment of bicarbonate stores and that one of the other events potentially explain the fall of the RER.
In addition, the trend of the measured objective variables has been shown to be coordinated with that of RPE: the lowest increases of EE and VO2 and the lowest decrease of FeO2 were coupled with the lowest increase of the perceived exertion in ERT, while the opposite trends were recorded in AERT. These results suggest that, in a concurrent training, the order of execution of the training sessions affects both objective (e.g. VO2) and subjective (i.e. RPE) variables. The relationship between RPE and objective variables, such as heart rate and oxygen consumption, (Borg, 1998; Warburton et al., 2006) is the basis of the use of RPE as methods to prescribe physical exercise. Taking into account that the absence of the recording of metabolic parameters during training is a limitation of the study, the high degree of standardization of both measurements and execution of the exercises are the strengths of the study. Our results suggest that the AERT protocol has the greater capacity to maintain a constant higher level of VO2 and ventilatory demand to physiologically and energetically sustain the training, compared with ERT and RET. However, more studies are needed to verify whether the organization of concurrent endurance and resistance exercise differently affects the trend of the observed variables during exercise.
Conclusion
The results of this study suggest that the order of execution of concurrent alternated endurance and resistance training affects the physiological responses to training during the recovery period. Hence, while the use of concurrent training could be useful to encourage compliance with the weekly exercise prescription when there is a lack of time, concurrent AERT, in a circuit manner, should be useful to optimize the recovery period due to the higher increase, from baseline, of fat-powered energy consumption compared with the other exercise protocols tested.
Acknowledgements
The authors thank Teca srl for technical support given during the study and for the supply of technical equipment.
Biographies
Andrea Di Blasio
Employment
Research Fellow, Department of Medicine and Sciences of Aging, G. d’Annunzio University, Chieti, Italy
Degrees
PhD, MSc, BSc
Research interest
Optimization of exercise for health
E-mail: andiblasio@gmail.com
Eugenio Gemello
Employment
Unit of Clinical Nutrition, G. d’Annunzio University, Chieti, Italy
Degree
MD
Research interest
Sport nutrition
E-mail: egemello@libero.it
Angelo Di Iorio
Employment
Researcher, Laboratory of Clinical Epidemiology and Aging; Depart. of Medicine and Sciences of Aging; Univ. Centre of Sports Medicine; G. d’Annunzio University, Chieti, Italy
Degrees
MD, Geriatrician, PhD, MSc in Epidemiology and Statistics
Research interest
Aging, disability, epidemiology
E-mail: a.diiorio@unich.it
Gabriella Di Giacinto
Employment
Research Fellow, University Centre of Sports Medicine; G. d’Annunzio University, Chieti, Italy
Degree
MD
Research interest
Sports medicine, rehabilitation
E-mail: gabry.digiacinto@libero.it
Tiziana Celso
Employment
University Centre of Sports Medicine, G. d’Annunzio University, Chieti, Italy
Degrees
MSc, BSc
Research interest
Health and fitness
E-mail: tizianacelso@hotmail.it
Donatella Di Renzo
Employment
University Centre of Sports Medicine, G. d’Annunzio University, Chieti, Italy
Degrees
BSc
Research interest
Sport nutrition
E-mail: d.direnzo@unich.it
Andrea Sablone
Employment
University Centre of Sports Medicine, G. d’Annunzio University, Chieti, Italy
Degrees
MSc, BSc
Research interest
Health and fitness
E-mail: sablone.andrea@gmail.com
Patrizio Ripari
Employment
Associate Professor, Faculty of Motor Sciences Education, Department of Biomedical Sciences: Director of Sports Medicine and Cardiology Section of the University Centre of Sports Medicine G. d’Annunzio University, Chieti, Italy
Degree
MD, Cardiologist and Sports Medicine Specialist
Research interest
Sports medicine, sports cardiology, exercise prescription in diseases, nutrition
E-mail: p.ripari@unich.it
References
- ACSM(2006) ACSM Guidelines for Exercise Testing and Prescription. 7th edition.Philadelphia: Lippincott Williams & Wilkins; [Google Scholar]
- American Dietetic Association, Dietitians of Canada, American College of Sports Medicine, Rodriguez N.R., Di Marco N.M., Langley S.(2009) American College of Sports Medicine position stand. Nutrition and athletic performance. Medicine and Science in Sport and Exercise 41, 709–731 [DOI] [PubMed] [Google Scholar]
- Bahr R., Hansson P., Sejersted O.M.(1990) Triglyceride/fatty acid cycling is increased after exercise. Metabolism 39, 993–999 [DOI] [PubMed] [Google Scholar]
- Borg G.(1998)Borg's Perceived Exertion and Pain Scales. Champaign: Human Kinetics; [Google Scholar]
- Borsheim E., Bahr R.(2003) Effects of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports Medicine 33, 1037-1060 [DOI] [PubMed] [Google Scholar]
- Braun W.A., Hawthorne W.E., Markofski M.M.(2005) Acute EPOC response in women to circuit training and treadmill exercise of matched oxygen consumption. European Journal of Applied Physiology 94, 500–504 [DOI] [PubMed] [Google Scholar]
- Compher C., Frankenfield D., Keim N., Roth-Yousey L.(2006) Best practice methods to apply measurement of resting metabolic rate in adults: a systematic review. Journal of the American Dietetic Association 106, 881–903 [DOI] [PubMed] [Google Scholar]
- Drummond M.J., Vehrs P.R., Schaalje G.B., Parcell A.C.(2005) Aerobic and resistance exercise sequence affects excess postexercise oxygen consumption. Journal of Strength and Conditioning Research 19, 332–337 [DOI] [PubMed] [Google Scholar]
- Frey G.C., Byrnes W.C., Mazzeo R.S.(1993) Factors influencing excess postexercise oxygen consumption in trained and untrained women. Metabolism 42, 822–828 [DOI] [PubMed] [Google Scholar]
- Fukuba Y., Yano Y., Murakami H., Kan A., Miura A.(2000) The effect of dietary restriction and menstrual cycle on excess post-exercise oxygen consumption (EPOC) in young women. Clinical Physiology 20, 165–169 [DOI] [PubMed] [Google Scholar]
- Gaesser G.A., Brooks G.A.(1984) Metabolic bases of excess post-exercise oxygen consumption: a review. Medicine and Science in Sports and Exercise 16, 29–43 [PubMed] [Google Scholar]
- Gillette C.A., Bullough R.C., Melby C.L.(1994) Postexercise energy expenditure in response to acute aerobic or resistive exercise. International Journal of Sport Nutrition 4, 347–360 [DOI] [PubMed] [Google Scholar]
- Haddock B.L., Wilkin L.D.(2006) Resistance training volume and post exercise energy expenditure. International Journal of Sports Medicine 27, 143–148 [DOI] [PubMed] [Google Scholar]
- Haskell W., Lee IM., Pate R.R., Powell K.E., Blair S.N., Franklin B.A., Macera C.A., Heath W., Thompson P.D., Bauman A.(2007) Physical activity and public health. Circulation 1116, 1081-1093 [DOI] [PubMed] [Google Scholar]
- Henry C.J., Lightowler H.J., Marchini J.(2003) Intra-individual variation in resting metabolic rate during the menstrual cycle. British Journal of Nutrition 86, 811–817 [DOI] [PubMed] [Google Scholar]
- Kraemer W., Fry A.(1995)Strength testing: development and evaluation of methodology. In: Physiological assessment of human fitness. Eds: Maud P.J., Foster C.Champaign: Human Kinetics; 115–138 [Google Scholar]
- Marfell-Jones M., Olds T., Stewart A., Carter L.(2006)International Standards for Anthropometric Assessment. ISAK, Potchefstroom; [Google Scholar]
- Matsuo T., Saitoh S., Suzuki M.(1999) Effects of menstrual cycle on excess postexercise oxygen consumption in healthy young women. Metabolism 48, 275–277 [DOI] [PubMed] [Google Scholar]
- Moschny A., Platen P., Klaaßen-Mielke R., Trampish U., Hinrics T.(2011) Barriers to physical activity in older adults in Germany: a cross-sectional study. International Journal of Behavioural Nutrition and Physical Activity 8, 121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oliveira N.L., Oliveira J.(2011) Excess postexercise oxygen consumption is unaffected by the resistance and aerobic exercise order in an exercise session. Journal of Strength and Conditioning Research 25, 2843-2850 [DOI] [PubMed] [Google Scholar]
- Oosthuyse T., Bosch A.N.(2010) The effect of the menstrual cycle on exercise metabolism: implications for exercise performance in eumenorrheic women. Sports Medicine 40, 207–227 [DOI] [PubMed] [Google Scholar]
- Solomon S.J., Kurzer M.S., Calloway D.H.(1982) Mentrual cycle and basal metabolic rate in women. American Journal of Clinical Nutrition 36, 611–616 [DOI] [PubMed] [Google Scholar]
- Villaca Alves J., Saavedra F., Simao R., Novaes J., Rhea M.R., Green D., Machado Reis V.(2011)Does aerobic and strength exercise sequence in the same session affect the oxygen uptake during and post-exercise? Journal of Strength and Conditioning Research DOI: 10.519/JSC.0b013e318238e852 [DOI] [PubMed] [Google Scholar]
- Warburton D.E.R., Nicol C.W., Bredin S.S.D.(2006) Prescribing exercise as preventive therapy. Canadian Medical Association Journal 174, 961–974 [DOI] [PMC free article] [PubMed] [Google Scholar]