

Abstract
The aim of this study was to examine the effect of changes in speed and incline slope on plantar pressure distribution of the foot during treadmill jogging. Plantar pressure parameters were measured with the Pedar-X system in twenty healthy girls (mean age of 20.7 years, mean height of 1.60m, and a mean weight of 53.35kg). Because variations in walking speed or slope can significantly change the magnitude of plantar pressure, comparisons of plantar pressure distribution between the two independent protocols during treadmill jogging were considered in this study. First, the subjects ran at the same speed of 2 m·s-1 with different incline slopes of 0%, 5%, 10%, and 15%. Second, they ran on the same slope of 0% with different speeds of 1.5 m·s-1, 2.0 m·s-1, and 2.5 m·s-1. The peak pressure of the eight plantar surface areas, apart from the medial forefoot and the hallux, significantly increased (p < 0.05) with an increase of 33% of peak pressure from 1.5 m·s-1 to 2.5 m·s-1 (speed) at heel region. In contrast, the peak pressures at the heel, medial fore-foot, toe and hallux decreased significantly (p < 0. 05) with increasing incline slope. At the heel, peak pressure reduced by 27% from 0% to 15% incline, however, pressure at the lateral midfoot region increased as following. Different speeds and incline slopes during jogging were associated with changes in plantar pressures. By systematic investigation of foot kinematics and plantar pressure during jogging with varying incline slope and speed, the results of this study provided further insight into foot biomechanics during jogging.
Key points.
The study aimed to compare the plantar pressure distribution of the foot between different incline and speed during treadmill jogging by using plantar insole measurement system.
With the increase of speed, apart from the hallux and medical forefoot, the peak pressure of all regions was raised significantly.
As the slope increased, there was reduced peak pressure of the heel, medial forefoot, and hallux and toes.
Key words: Jogging, plantar pressure, incline, speed
Introduction
There is an increasing trend for people to choose jogging as a form of physical activity to maintain their health (Razeghi and Batt, 2000; Thompson et al., 2003). For instance, in the United States, more than 30 million people prefer jogging as their basic form of exercise (Nagel et al., 2007). Recently, there are more people jogging with a treadmill at the gym or the home setting. In the past, many studies also used treadmill to study the relative effect of running at different speeds or gradients. Guo et al., 2006 studied the effects of speed and incline on lower extremity kinematics during treadmill jogging in healthy subjects. The main advantage of jogging is to improve cardiopulmonary fitness. Aerobic and endurance-type activities such as jogging can result in improvements of physical fitness and aid in the prevention of cardiovascular disease (Razeghi and Batt, 2000). For subjects with hypertension, after forty-five minutes of running at 70% VO2max, previous study showed that systolic blood pressure (BP) post-exercise hypotension (PEH) lasting for two hours and diastolic BP PEH lasting for one hour and fifteen minutes (Hagberg et al., 1987). Mota et al., 2009 found that twenty minutes of treadmill running resulted in PEH lasted more than seven hours as well as a higher decrease of systolic BP (-11.1 ± 7.6 mmHg) and decreases of diastolic BP (-4.0 ± 6.4 mmHg).
Jogging is one of the common sports activities that contribute to lower limb injuries in the foot. The potential factors include overuse or repetitive loading stress. Stress fractures of the metatarsals are frequently reported in overloading injuries of long distance runners and are considered a result of a multi-factorial process (Van Mechelen, Hlobil et al., 1992). Jogging is associated with increased risk of incurring lower limb injuries. Approximately 90% of running related injuries occur in the lower extremity (Marti et al., 1988). Nagel et al., 2007 found that long distance runners show increased peak pressure of the metatarsal bones during running, and these results indicate that the long distance runners are prone to sustain metatarsal stress fractures. James and associates (1978) showed that two-thirds of the chronic injuries were attributed to high mileage, workout intensity, running on inclines and hard surfaces, and rapid change in training routine. Moreover, several authors have postulated that impact forces on the lower limbs associated with repetitive loading are responsible for overuse injuries in the musculoskeletal system (Cavanagh and Lafortune, 1980; Nigg et al., 1987). On the other hand, most sport injury researchers suggest that the types of injuries may differ between genders. Anatomically, females have shorter legs, narrower shoulders, wider pelvises, and a greater valgus angulation at the knees than males (Arendt and Dick, 1995; Dugan, 2005; Hale, 1984; Klafs and Lyon, 1978; Sallis et al., 2001; Thomas, 1979). Our purpose was to study the effect of changes in speed and incline slope on plantar pressure distribution of the foot during treadmill jogging for females.
A typical gait cycle can be subdivided into two phases: contact phase and support phase. During the contact phase, the ground reaction force (GRF) generated is the sum of body weight and all force that accelerate and/or decelerate the body mass. GRF produces plantar pressure during body motion. Numerous studies have investigated the increase in plantar pressure and GRF with increases in the speed of walking (Alexander and Jayes, 1980; Bates et al., 1983; Bobbert et al., 1991; Cavanagh and Lafortune, 1980; Jacobs et al., 1972; Dickinson et al., 1985; Munro et al., 1987; Nigg et al., 1987; Roy, 1982). Those studies showed that the vertical maximum force of walking falls within the range of 1.1-1.5 times of body weight (BW). The plantar pressure on the heel, medial and central metatarsals, and toes are significantly higher when walking speeds increase from 57 m·min-1 to 80 m·min-1. With faster speed of walking (greater than 80 m·min-1), there is increased pressure on the toes and heel (Keller et al., 1996). As walking speed increases, people will adopt from walking to running. The difference between walking and running lies in the shorter double support phase during running. Due to these changes in gait cycle, the pattern of plantar pressure and GRF are also altered. However, to the best of our knowledge, there are few arguments about the plantar pressure and GRF increase with increases in speed. Munro et al., 1987 indicate when speeds of 3-5 m·s-1 the vertical maximum forces is ranging from 2.51 BW to 2.83 BW. The load-bearing during running gait is almost two times of walking. Changes in incline slope can also alter biomechanical factors such as vertical GRF and peak pressure, but few studies have systematically examined this.
Increased incline and speed will not only increase stress on the cardiopulmonary system, but may also alter the plantar pressure pattern on the foot. Biomechanical factors such as maximum force and peak pressures can play an essential role for the detection of runner injury. Pressure (Messier and Pittala, 1988) and impact forces (Hreljac et al., 2000; Van Mechelen, 1992) on the foot have been implicated as the primary causes of running injuries. Most studies have examined these factors through the use of force plates. However, there are three disadvantages in using force plates to interpret forces at the foot: First, force plates need to be built into the runway or path; second, the number of different contact surfaces that can be measured on a force plate is limited; and third, only one step can be measured during one measurement cycle. Thus, the force plate is not ideal for measurement of plantar pressure in this study. There-fore, in the current study, we used an in-sole plantar pres-sure system to overcome these problems. Here we aimed to compare the plantar pressure distribution of the foot between different incline and speed during treadmill jogging. Based on different inclines and speeds, we hypothesized that the peak pressure and contact area would decrease in the heel and increase in the lateral metatarsal independent of the shoe being used.
Methods
Twenty healthy females with no history of neuromuscular disease or serious musculoskeletal injury participated in this study. Participants had a mean age of 20.7 ± 4.7 years, mean height of 1.60 ± 0.07 m, and a mean weight of 53.3 ± 6.8 kg. All subjects were collegiate students and reported that they did not do regular jogging. These participants were recruited from the campus to meet the inclusion and exclusion criteria. Informed consent, approved by the university ethical review committee, was obtained from all volunteers prior to involvement in the study.
We collected anthropometric data of each subject including age, height, and weight. The Pedar-X system pressure insoles (Novel, St. Paul, MN) were placed inside their shoes. Prior to testing, all subjects were requested to warm up including some regular stretch exercise and running at slow speed that they can to familiarize the treadmill. The pressure insoles were calibrated by instructing subjects to lift each leg from the ground. All subjects were informed about the procedures and signed a written consent. The treadmill (IEC EN 60335-1, h/p/cosmos sports & medical gmbh, Germany) consisted of walking surface of 1.5 0.5 m. There were different modes to be used in different speeds: (1) 1.5 m·s-1, 2.0 m·s-1, and 2.5 m·s-1 with the slope at zero, and (2) the same speeds with different slopes that were 0%, 5%, 10%, 15%. Prior to starting the test, one trial was collected at each condition. Each trial lasted for ~30 seconds. Initially, the slope was kept flat and the speed was gradually increased. While the speed at 1.5 m·s-1, we collected the data which is 1.5 m·s-1 and 0%. And then we kept on increasing speed gradually at 2.0 m·s-1 and 2.5 m·s-1 collecting data. The speed was slowed down to 2.0 m·s-1. At this speed, the incline gradually was gradually increased to 0%, 5%, 10%, and 15%.
Novel Groupmask Evaluation software (Pedar®-x, Novel Co., Germany) was used to quantify forces and pressures in different regions of the foot. For analysis of plantar pressure pattern, the insole data were divided into eight regions (masks) as defined in the software. The regions include heel, medial arch, lateral arch, medial metatarsal, central metatarsals, lateral metatarsals, great toe, and little toes (Figure 1). The heel comprised of the first 0% to 30% of foot length, the midfoot the next 30% to 60%, the forefoot the following 60% to 85%, and the hallux/toe the remaining 85% to 100%. The midfoot region width was divided into two equal parts. The forefoot region width was divided into equal thirds, creating three forefoot regions. The hallux/toe region width was also divided into two parts, with the hallux region occupying the medial 40% and the toe region occupying the lateral 60%. At each condition, we only used entire foot contact period to analysis the maximum force and the peak pressure. Maximum force is calculated from the summation of the measured force on each sensor in the insole. This was used to predict the loaded energy on foot. Peak pressure represents the aggregate of the all the measured pressures from different sensors in specific parts of the foot, and is important while investigating foot injury mechanism. Repeated-measures ANOVA, followed by a post-hoc Tukey test, were used to compare plantar pressure and maximum force with changes in jogging speed and incline slope. Significance level was set up as 0.05.
Figure 1.
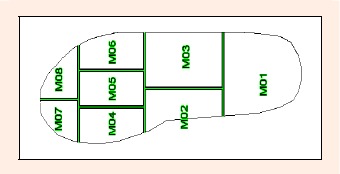
Eight anatomical regions of the foot defined to be used for plantar pressure distribution analysis. M01: Heel, M02: Medial midfoot, M03: Lateral midfoot, M04: Medial forefoot, M05: Central forefoot, M06: Lateral forefoot, M07: Hallux, M08: Toes.
Results
With the increase of speed, apart from the medial forefoot and hallux, the peak pressure of all regions was raised significantly (p < 0.05). As the speed increased from 1.5 m·s-1 to 2.5 m·s-1, the peak pressure of heel region increased about 33%, that in the medial arch increased about 16%, and that in the lateral arch lift increased about 25%. In the forefoot, the peak pressure of central forefoot increased about 19% and that in the lateral forefoot increased about 18% (Table 1). When the speed increased from 1.5 m·s-1 to 2.5 m·s-1, the maximum force of heel increased about 46%, the medial arch increased about 67% and that in lateral arch lift increased about 48%. In addition, the maximum forces of central forefoot increases about 23%, that in the lateral forefoot raised about 27%, and that in the medial forefoot lift raised about 17% (Table 2).
Table 1.
The peak pressure at same slope 0% with different speeds. Data are means (±SD).
| Mask | Speed 1.5 | Speed 2.0 | Speed 2.5 | F Value | Post Hoc |
|---|---|---|---|---|---|
| He(M01) | 143.6 (73.6) | 170.7 (85.7) | 191.3 (71.8) | 4.54* | S2.5>S2.0>S1.5 |
| MM(M02) | 154.1 (79.2) | 172.9 (83.9) | 178.2 (92.2) | 7.23* | S2.5,2.0>S1.5 |
| LM(M03) | 130.3 (44.8) | 149.5 (41.9) | 162.3 (46.4) | 19.17* | S2.5>S2.0>S1.5 |
| MF(M04) | 339.8 (108.1) | 360.7 (114.2) | 377.8 (101.2) | 2.42 | S2.5>S1.5 |
| CF(M05) | 223.8 (48.6) | 244.5 (53.1) | 266.5 (64.6) | 10.74* | S2.5>S2.0>S1.5 |
| LF(M06) | 172.7 (51.3) | 189.0 (49.9) | 203.9 (54.4) | 11.76* | S2.5>S2.0>S1.5 |
| Ha(M07) | 309.3 (123.9) | 323.6 (123.1) | 333.1 (103.4) | 0.94 | |
| To(M08) | 126.3 (47.4) | 139.0 (49.3) | 147.8 (50.7) | 5.13* | S2.5>S1.5 |
He(M01): Heel, MM(M02): Medial midfoot, LM (M03): Lateral midfoot, MF(M04): Medial forefoot, CF(M05): Central forefoot, LF(M06): Lateral forefoot, Ha(M07): Hallux, To(M08): Toes.
* p < 0.05
Table 2.
The maximum force at same slope 0% with different speeds. Data are means (±SD).
| Mask | Speed 1.5 | Speed 2.0 | Speed 2.5 | F Value | Post Hoc |
|---|---|---|---|---|---|
| He(M01) | 281.7 (159.7) | 354.1 (188.1) | 410.5 (169.0) | 7.51* | S2.5>S2.0>S1.5 |
| MM(M02) | 45.7 (31.8) | 78.2 (111.7) | 76.1 (39.5) | 2.96* | |
| LM(M03) | 151.0 (79.2) | 193.9 (80.9) | 223.1(79.2) | 17.87* | S2.5>S2.0>S1.5 |
| MF(M04) | 251.8 (79.2) | 278.6 (74.3) | 294.1 (75.0) | 5.49* | S2.5>S1.5 |
| CF(M05) | 195.1 (60.6) | 219.5 (60.4) | 239.3 (65.8) | 14.90* | S2.5>S2.0>S1.5 |
| LF(M06) | 116.1 (59.0) | 136.7 (55.2) | 147.3 (59.9) | 14.90* | S2.5>S1.5 |
| Ha(M07) | 101.7 (53.8) | 101.3 (39.7) | 108.6 (41.0) | 0.87 | |
| To(M08) | 55.7 (30.4) | 59.1 (25.9) | 64.2 (24.9) | 2.11 |
He(M01): Heel, MM(M02): Medial midfoot, LM (M03): Lateral midfoot, MF(M04): Medial forefoot, CF(M05): Central forefoot, LF(M06): Lateral forefoot, Ha(M07): Hallux, To(M08): Toes.
* p < 0.05
As the slope increased, there was reduced peak pressure of the heel, medial forefoot, and hallux and toes (p < 0.05). In the heel, the peak pressure decreased about 27% when slope increased from 0% to 15%. In addition, the peak pressure of medial forefoot decreased about 15%. With the slope increasing from 0% to 15%, the peak pressures of hallux decreased about 26% and that in the toes reduced about 19% (Table 3). There were no significant differences between lateral arch and medial arch in midfoot, the peak pressure of lateral arch increased about 8% and that in the medial arch decreased about 8%. The maximum force is similar to the peak pressure. As the jogging slope increased, there was reduced maximum force of heel, the medial forefoot, and hallux and toes (p < 0.05) (Table 4). However, the lateral arch increased (p < 0.05) with increasing slope.
Table 3.
The peak pressure at same speed 2.0m·s-1 with different slopes. Data are means (±SD).
| Mask | SL0 | SL5 | SL10 | SL15 | F Value | Post Hoc |
|---|---|---|---|---|---|---|
| He(M01) | 170.7 (85.7) | 161.4 (56.6) | 142.6 (40.3) | 124.1 (41.6) | 4.36* | SL0,5>SL10,15; SL10>SL15 |
| MM(M02) | 172.9 (83.9) | 155.1 (77.5) | 164.8 (82.3) | 159.3 (83.2) | 1.17 | |
| LM(M03) | 149.5 (41.9) | 155.2 (33.9) | 161.1 (44.4) | 161.7 (46.6) | 2.32 | |
| MF(M04) | 360.7 (114.2) | 322.1 (90.1) | 318.5 (78.0) | 306.8 (105.5) | 3.98* | SL0>SL5,10,15 |
| CF(M05) | 244.5 (53.1) | 290.8 (290.3) | 249.1 (51.6) | 240.7 (54.4) | 1.14 | |
| LF(M06) | 189.0 (49.9) | 192.9 (48.3) | 196.3 (51.4) | 194.1 (55.0) | 1.00 | |
| Ha(M07) | 323.6 (123.1) | 277.5 (90.7) | 258.5 (82.2) | 238.9 (71.9) | 9.26* | SL0>SL5,10,15; SL5>SL15 |
| To(M08) | 139.0 (49.3) | 120.4 (36.3) | 116.0 (30.7) | 113.0 (30.2) | 9.92* | SL0>SL5,10,15 |
He(M01): Heel, MM(M02): Medial midfoot, LM (M03): Lateral midfoot, MF(M04): Medial forefoot, CF(M05): Central forefoot, LF(M06): Lateral forefoot, Ha(M07): Hallux, To(M08): Toes.
* p < 0.05
Table 4.
The maximum force at same speed 2.0m·s-1 with different slopes. Data are means (±SD).
| Mask | SL0 | SL5 | SL10 | SL15 | F Value | Post Hoc |
|---|---|---|---|---|---|---|
| He(M01) | 354.1 (188.1) | 364.2 (135.9) | 319.4 (104.8) | 270.4 (113.9) | 3.49* | SL5>SL10,15; SL0,10>SL15 |
| MM(M02) | 78.2 (111.7) | 73.3 (40.0) | 81.3 (43.3) | 75.5 (43.4) | 0.08 | |
| LM(M03) | 193.9 (80.9) | 223.3 (78.5) | 242.9 (90.7) | 234.8 (87.2) | 8.53* | SL10>5,0; SL15,5>SL0 |
| MF(M04) | 278.6 (74.3) | 257.0 (60.0) | 255.3 (61.3) | 238.6 (78.3) | 4.33* | SL0>SL10,15 |
| CF(M05) | 219.5 (60.3) | 218.2 (57.6) | 222.0 (54.8) | 212.7 (53.3) | 1.07 | |
| LF(M06) | 136.7 (55.2) | 132.7 (56.7) | 137.3 (52.6) | 138.3 (54.1) | 0.22 | |
| Ha(M07) | 101.3 (39.7) | 94.4 (41.6) | 83.6 (36.8) | 76.5 (30.5) | 13.58* | |
| To(M08) | 59.1 (25.9) | 56.1 (22.5) | 49.9 (17.9) | 47.4 (16.4) | 10.19* | SL0>SL10,15; SL5>SL15 |
He(M01): Heel, MM(M02): Medial midfoot, LM (M03): Lateral midfoot, MF(M04): Medial forefoot, CF(M05): Central forefoot, LF(M06): Lateral forefoot, Ha(M07): Hallux, To(M08): Toes.
* p < 0.05
Discussion
As expected, faster speeds resulted in higher peak plantar pressures and greater maximum force in all regions (Table 1 and Figure 2). It could be argued that subjects increased their inversion of the ankle/foot when running speed is increased. In contrast, as jogging slope is increased, the peak pressure of heel, the medial forefoot, the medial midfoot, hallux and toes decreased (Table 3 and Figure 3). In other words, the peak pressure decreased in all regions except lateral side. The decreased plantar pressure is likely to result from reduced vertical component of GRF with increased slope. The increased pressure in the lateral side could be a consequence of the inverted foot while jogging on an incline slope. At heel strike, the body needs to initially decrease contact speed (acceleration of gravity) of body mass and maintain balance. In our findings, the maximum force and peak pressure of a heel region increased with greater speed. As the speed increased from 1.5 m·s-1 to 2.5 m·s-1, the peak pressure and maximum force also increased in the heel region.
Figure 2.
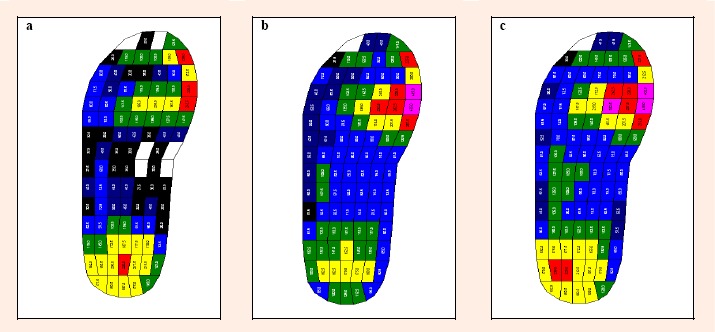
The peak pressure at same slope 0% with different speeds (a) 1.5 m·s-1 (b) 2.0 m·s-1 (c) 2.5 m·s-1 with the increasing speed, the value of the peak pressure would become larger.
Figure 3.
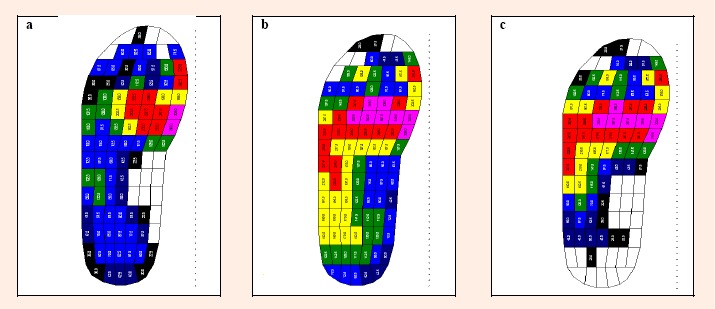
The peak pressure at same speed 2m·s-1 with different slope (a) 5% (b) 10% (c) 15% the increased pressure in the lateral metatarsal could be the consequence of the inverted foot while slope jogging.
We found that GRF and peak pressure of the entire foot increased with increasing speed. This result is similar with the other studies (Burnfield et al., 2004; Chuckpaiwong et al., 2008; Segal et al., 2004). Burnfield et al., 2004 indicate that faster walking resulted in higher pressures under all foot regions except for the arch and lateral metatarsal, primarily due to greater forces under the heel, medial metatarsal and toes. The results of the current study showed that plantar pressure increased in all regions and the peak pressure was greater in the hallux and medial forefoot, and thus is consistent with findings from Burnfield et al., 2004. In our study, peak pressure increased significantly in lateral side with increased speed. These results are different with that from previous findings. One possible explanation for the discrepancy could be that those authors examined slower speeds (0.95 m·s-1, 1.33 m·s-1, 1.62 m·s-1). Thus it is possible that foot patterns observed in that study are not typical of running. Moreover, peak pressure and maximum force of heel during running is significant higher than that of walking (Hennig and Rosenbaum, 1991). We also found that peak pressure and maximum force increase from 1.5 m·s-1 (similar to the fast walking speed) to 2.5 m·s-1 (similar to the running speed).
There are two possible reasons to explain the major findings. One reason is that the midfoot is better at adapting to changes in forces as it may help to absorb shock from the ground. The body has to move in response to GRFs to the midfoot quickly in order to deal with increased shock at higher speeds. We divided the midfoot into two sub-areas such as medial midfoot and lateral midfoot. Medial midfoot is approximately the arch of the foot and lateral midfoot was defined the as lateral arch. The results confirmed that the maximum force of medial midfoot increased when speed was increased. The foot arch plays an important role of absorbing shock. Not only foot arch, but the knee may also aid in reducing the shock by slight flexion and following extension at the early stand phase. (Guo et al., 2006). After knee extension, therefore, the foot arch of the medial midfoot becomes flatter to absorb shocks with increases in speed. GRFs and the peak pressure of lateral midfoot also increase significantly with increasing speed. In lateral arch, the lateral midfoot, the peak pressure also increased with increases in speed. The peak pressure of medial arch also increased with increased speed. As the result, it is likely that the foot produces more inversion with increases in speed. It could be argued that due to increased speed, the demand for the foot to maintain stability greatly increases. One method to achieve this is to increase foot toe-in with subtalar inversion to produce a stable lever. Not only can this mechanism provide stability, but it may also increase propulsion force for push off (Guo et al., 2006).
Propulsion force is another reason why GRFs tend to shift to the midfoot more quickly when jogging at higher speeds. As speed is increased, the force of propulsion increases gradually. In the push-off stage, the ankle will exhibit increased plantarflexion with greater speeds to generate more power for forward motion (Guo et al., 2006), with increases in peak values for positive angular velocities. Therefore, we hypothesized that the maximum force at the forefoot will increase with increasing speed. The maximum force of all regions increased significantly with increased speed Increased foot toe-in is accompanied with subtalar inversion for providing a stable level for push off as required for increased propusion force as increased speed or slope.
The GRF decreased with increasing slope during jogging. It could be argued that this may be due to a shifting of first contact area from the heel to the midfoot. At the contact phase, ankle motion is not altered between level and uphill running (Roberts and Belliveau, 2005). Therefore, the maximum force and peak pressure decrease significantly at heel with slopes up. Grampp et al (Grampp et al., 2000) indicated that an increased plantar pressure and force was found over the hallux and medial forefoot with increasing slope. These findings may reflect increased muscle activation patterns in conjunction with increased normal forces. However, the current study showed reduced plantar pressure in all regions except for lateral side, which was a result of decreased vertical component of GRF. Furthermore, increased pressure in the lateral side could be the consequence of the inverted foot while slope jogging. During level running, body major use screw home mechanism and the foot arch to overcome this situation. In stance phase during knee extension, prolonged anterior glide on the medial side produces external tibial rotation (the “screw-home ”mechanism). Thus, the knee is in the close-pack position. At this position the knee is more stable. In push off phase the mechanism had enough power to push off. In the end of stance phase subtalar inversion would cause foot arch increased. Furthermore, transverse tarsal joint would converge and become rigid for the foot to push off. With increasing speed, the foot arch will play an important role for this purpose. This is similar between level and uphill running. Because of the range of motion of keen is decreasing with incline increasing (Roberts and Belliveau, 2005). According to this finding, foot arch instead of the knee can provide the primary assistance for shock absorption. It was not surprising that the maximum force and peak pressure of lateral midfoot increased significantly with increases in slope of incline during jogging.
According the finding above, although there was no significant difference in medial midfoot, the foot still demonstrated more inversion with increased slope. As slope rise, foot increased toe-in to provide a stable level for push off at terminal stand phase. However, the ankle is not the chief propulsion for uphill running. There was no increase in ankle or knee work to compensate for the increasing work during jogging on an incline (Roberts and Belliveau, 2005). Instead, the hip is required to produce most of the work for propulsion (Guo et al., 2006). Increased hip, knee and ankle flexion in swing and early stance phase is important to ensure foot clearance and heel contact as jogging at increased slope. Therefore, the maximum force of forefoot displays no significant difference in uphill running.
In the current study, we used an in- sole plantar pressure system instead of force plates as this allowed the collection of plantar pressure data across a greater sample of walking strides. However, in-sole plantar pressure system could not measure shear force and propulsion force. This was a major limitation in the study. As subjects run on an incline, shearing force occurs. Shear forces alone may not cause tissue injury, but may contribute so that in the presence of increased pressure, more severe tissue damage will occur (Bennett, 1988). Another limitation is we also could not obtain the value of the propulsion force. Friction occurs when patients drag their foot across an external surface. This results in an abrasion with damage to the most superficial layer of skin. Therefore, in future studies, it would be important to determine both of parameters. Consequently, the results of this study could be a reference to clinician and coach to prevent further sport injury while jogging on a treadmill, especially when we design an exercise prescription for the patients who have foot ailment.
Conclusion
With increasing of speed, the peak pressure of all regions except the medial forefoot and hallux increased significantly. Apart from the regions of the hallux and toes, the maximum force increased significantly with increases in speed. As the jogging slope increased, the peak pressure of heel, the medial forefoot, and hallux and toes were significantly decreased. The maximum force of heel, the medial forefoot, and hallux and toes reduced significantly. However, lateral arch increases significantly with rising of jogging slope. Hence, the results of this study may offer a reference for young females to choose a more suitable gradient and treadmill speed.
Acknowledgments
This work is supported by Nation Science Council NSC 94-2320-B-037-017, Taiwan.
Biographies

I-Ju Ho
Employment
Student in the Department of Veterinary Medicine, National Chia Yi University, Taiwan.
Degree
BSc.
Research interests
Veterinary physiology and cardiopulmonary biomechanics.
E-mail: camille751110@hotmail.com

Yi-You Hou
Employment
Department of Sports Medicine, College of Medicine, Kaohsiung Medical University, Taiwan.
Degree
PhD.
Research interests
Control theory, artificial intelligence, biomechanics, and sports medicine.
E-mail: hou.yi_you@msa.hinet.net

Chich-Haung Yang
Employment
Lecturer in Department of Physical Therapy in Tzu-Chi College of Technology, Hualien, Ta.
Degree
PhD Candidate, MSc.
Research interests
Musculoskeletal physiotherapy, manual therapy, sports medicine, biomechanics, and movement science.
E-mail: r.chyang@mail.tcu.edu.tw

Wen-Lan Wu
Employment
Associate professor in the Department of Sports Medicine in Kaohsiung Medical University.
Degree
PhD.
Research interests
biomechanics of human motion, biomechanical engineering, orthopedic physical therapy, and rehabilitation engineering.
E-mail: wenlanwu@kmu.edu.tw

Sheng-Kai Chen
Employment
Associate professor of the Department of Sports Medicine, Kaohsiung Medical University, Taiwan.
Degree
PhD.
Research interests
Arthroscopic surgery, shoulder reconstruction, and sports medicine.
E-mail: shenkai@kmu.edu.tw

Lan-Yuen Guo
Employment
Associate Professor at the Department of Sports Medicine, Kaohsiung Medical University, Taiwan.
Degree
PhD.
Research interests
Sports medicine, biomechanics, movement science, and physical therapy.
E-mail: yuen@kmu.edu.tw
References
- Alexander R.M., Jayes A.S. (1980) Fourier analysis of forces exerted in walking and running. Journal of Biomechanics 13, 383-390 [DOI] [PubMed] [Google Scholar]
- Arendt E., Dick R. (1995) Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. American Journal of Sports Medicine 23, 694-701 [DOI] [PubMed] [Google Scholar]
- Bates B.T., Osternig L.R., Samhill J.A., James S.L. (1983) An assessment of subject variability, subject-shoe interaction, and the evaluation of running shoes using ground reaction force data. Journal of Biomechanics 16, 181-191 [DOI] [PubMed] [Google Scholar]
- Belli A., Kyrolainen H., Komi P. V. (2002) Moment and power of lower limb joints in running. International Journal of Sports Medicine 23, 136-141 [DOI] [PubMed] [Google Scholar]
- Bennett L., Lee B.Y. (1988) Vertical shear existence in animal pressure threshold experiments. Decubitus 1, 18. [PubMed] [Google Scholar]
- Bobbert M.F., Schamhardt H.C., Nigg B.M. (1991) Calculation of vertical ground reaction force estimates during running from positional data. Journal of Biomechanics 24, 1095-1105 [DOI] [PubMed] [Google Scholar]
- Burnfield J.M., Few C.D., Mohamed O.S., Perry J. (2004) The influence of walking speed and footwear on plantar pressures in older adults. Clinical Biomechanics 19, 78-84 [DOI] [PubMed] [Google Scholar]
- Cavanagh P. R., Lafortune M. A. (1980) Ground reaction forces in distance running. Journal of Biomechanics, 13, 397-406 [DOI] [PubMed] [Google Scholar]
- Chuckpaiwong B., Nunley J.A., Mall N.A., Queen R.M. (2008) The effect of foot type on in-shoe plantar pressure during walking and running. Gait & Posture 28, 405-411 [DOI] [PubMed] [Google Scholar]
- Dickinson J.A., Cook S.D., Leinhardt T.M. (1985) The measurement of shock waves following heel strike while running. Journal of Biomechanics 18, 415-422 [DOI] [PubMed] [Google Scholar]
- Dugan S.A. (2005) Sports-related knee injuries in female athletes: what gives? American Journal of Physical Medicine & Rehabilitation 84, 122-130 [DOI] [PubMed] [Google Scholar]
- Grampp J., Willson J., Kernozek T. (2000) The plantar loading variations to uphill and downhill gradients during treadmill walking. Foot & Ankle International 21, 227-231 [DOI] [PubMed] [Google Scholar]
- Guo L. Y., Su F. C., Yang C. H., Wang S. H., Chang W. L., Lin H. T. (2006). Effects of speed and incline on lower extremity kinematics during treadmill jogging in health subjects. Biomedical Engineering- Applications, Basis & Communications 18, 73-79 [Google Scholar]
- Hagberg J. M., Montain S. J., Martins W. H. (1987) Blood pressure and hemodynamic responses after exercise in older hypertensives. Eur J Appl Physiol 63, 270-276 [DOI] [PubMed] [Google Scholar]
- Hale R. (1984) Factors important to women engaged in vigorous physical activity. In: Sports Medicine. Ed: Strauss R.H.Philadelphia: W. B. Saunders Co.259-269 [Google Scholar]
- Hennig E.M., Rosenbaum D. (1991) Pressure distribution patterns under the feet of children in comparison with adults. Foot & Ankle International 11, 306-311 [DOI] [PubMed] [Google Scholar]
- Hreljac A., Marshall R.N., Hume P.A. (2000) Evaluation of lower extremity overuse injury potential in runners. Medicine and Science in Sports and Exercise 32, 1635-1641 [DOI] [PubMed] [Google Scholar]
- Jacobs N.A., Skorecki J., Charnley J. (1972). Analysis of the vertical component of force in normal and pathological gait. Journal of Biomechanics 5, 11-34 [DOI] [PubMed] [Google Scholar]
- James S.L., Bates B.T., Osterning L.R. (1978) Injuries to runners. The American Journal of Sports Medicine 6, 40-50 [DOI] [PubMed] [Google Scholar]
- Keller T.S., Weisberger A.M., Ray J.L., Hasan S.S., Shiavi R.G., Spengler D.M. (1996) Relationship between vertical ground reaction force and speed during walking, slow jogging, and running. Clinical Biomechanics (Bristol, Avon) 11, 253-259 [DOI] [PubMed] [Google Scholar]
- Klafs C., Lyon J. (1978) The female athlete. 2ndedition CV Mosby, St Louis [Google Scholar]
- Lanese R.R., Strauss R.H., Leizman D.J., Rotondi A.M. (1990) Injury and disability in matched men's and women's intercollegiate sports. American Journal of Public Health 80, 1459-1462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marti B., Vader J.P., Minder C.E., Abelin T. (1988) On the epidemiology of running injuries. The 1984 Bern Grand-Prix study. The American Journal of Sports Medicine 16, 285-294 [DOI] [PubMed] [Google Scholar]
- Messier S.P., Pittala K.A. (1988) Etiologic factors associated with selected running injuries. Medicine and Science in Sports and Exercise 20, 501-505 [PubMed] [Google Scholar]
- Mota M.R., Pardono E., Lima L.C.J., Arsa G., Bottaro M., Campbell C.S.G., Simoes H.G. (2009) Effects of treadmill running and resistance exercises on lowering blood pressure during the daily work of hypertensive subjects. Journal of Strength and Conditioning Research 23, 2331-2338 [DOI] [PubMed] [Google Scholar]
- Munro C.F., Miller D.I., Fuglevand A.J. (1987) Ground reaction forces in running: a reexamination. Journal of Biomechanics 20, 147-155 [DOI] [PubMed] [Google Scholar]
- Nagel A., Fernholz F., Kibele C., Rosenbaum D. (2007) Long distance running increases plantar pressures beneath the metatarsal heads A barefoot walking investigation of 200 marathon runners. Gait & Posture 27, 152-155 [DOI] [PubMed] [Google Scholar]
- Nakaya S., Nishswaki T. (2007) Motion analysis of treadmill running for foorwear designing. In. Proceedings 8th Footwear Biomechanics Symposium, June 27-29, Taipei, Taiwan: 135-136 [Google Scholar]
- Nigg B.M., Bahlsen H.A., Luethi S.M., Stokes S. (1987) The influence of running velocity and midsole hardness on external impact forces in heel-toe running. Journal of Biomechanics 20, 951-999 [DOI] [PubMed] [Google Scholar]
- Razeghi M., Batt M.E. (2000). Biomechanical analysis of the effect of orthotic shoe inserts: a review of the literature. Sports Medicine 29, 425-438 [DOI] [PubMed] [Google Scholar]
- Roberts T.J., Belliveau R.A. (2005) Sources of mechanical power for uphill running in humans. Journal of Experimental Biology 208, 1963-1970 [DOI] [PubMed] [Google Scholar]
- Roy B. (1982) Biomechanical characteristics of endurance running. Canadian Journal of Applied Sport Sciences 7, 104-115 [PubMed] [Google Scholar]
- Sallis R.E., Jones K., Sunshine S., Smith G., Simon L. (2001) Comparing sports injuries in men and women. International Journal of Sports Medicine 22, 420-423 [DOI] [PubMed] [Google Scholar]
- Segal A., Rohr E., Orendurff M., Shofer J., Obrien M., Sangeorzan B. (2004) The effect of walking speed on peak plantar pressure. Foot & Ankle International 25, 926-933 [DOI] [PubMed] [Google Scholar]
- Thomas C. (1979) Factors important to women participants in vigorous athletics. In: Sports Medicine and Physiology. Ed: Strauss R.WB. Saunders, Philadelphia [Google Scholar]
- Thompson P.D., Buchner D., Pina I.L., Balady G.J., Williams M.A., Marcus B.H., Berra K., Blair S.N., Costa F., Franklin B., Fletcher G.F., Gordon N.F., Pate R.R., Rodriguez B.L., Yancey A.K., Wenger N.K. (2003) Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 107, 3109-3116 [DOI] [PubMed] [Google Scholar]
- Van Mechelen W. (1992) Running injuries. A review of the epidemiological literature. Sports Medicine 14, 320-335 [DOI] [PubMed] [Google Scholar]
- Van Mechelen W., Hlobil H., Kemper H.C. (1992) Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Medicine 14, 82-99 [DOI] [PubMed] [Google Scholar]