

Abstract
Background: New surgical technologies have been introduced in thyroid surgery, to achieve vessel sealing and hemostasis. The aim of the study was to examine their effectiveness and compare the outcome of total thyroidectomy using the Harmonic Focus™, the LigaSure® Precise and the conventional technique of suture ligation.
Methods: A retrospective case-matched study of all total thyroidectomies between October 2008 through May 2010 was conducted. Patients (n=240) underwent total thyroidectomy using three different methods; the Harmonic Focus™ (Group F, n=80), the LigaSure Precise® (Group L, n=80) and the conventional technique of suture ligation (Group C, n=80).
Results: No significant differences were identified between the 3 groups in terms of demographics, thyroid gland weight, pathologic diagnosis, preoperative and postoperative calcium levels, postoperative complications, duration of hospital stay, and final outcome. The operative time was shorter with Harmonic Focus® by about 15%. Statistical analysis revealed a statistically significant difference between operations with F (62.7±14.1 minutes) and C (72.7±13.6minutes) with (p=0.019).
Conclusion: Both devices were safe and efficient. A significant reduction of the operative time was found with Harmonic Focus® compared to the other two techniques with no statistically significant differences in postoperative complications in the 3 groups.
Keywords: thyroidectomy, surgical devices, operative time, complications
Total thyroidectomy is now routinely used even in benign pathologies1 greatly increasing the number of procedures performed. Standardization of the technique has decreased the incidence of complications to minimal levels, mainly due to the importance placed on an adequate control of hemostasis reducing the risk of damaging the superior and recurrent laryngeal nerves and the parathyroid glands.
In the recent years several novel instruments have been developed and implemented in both open and laparoscopic surgery. These instruments utilize the properties and the effects of different energy sources, including radiofrequencies and ultrasound. Further refinements have led to devices with specific characteristics for use in thyroid surgery2-5. Even the comparison of the two devices has not produced clear results: some authors reported a greater incidence of complications with Harmonic, but a longer surgical time with Ligasure6.
A new scissor has recently been introduced with the intent of increasing efficacy and intraoperative security. This is a retrospective case-matched study with the aim of comparing the results obtained using three techniques: the electrothermal bipolar vessel sealing system (Ligasure®), the harmonic curved shears (Harmonic Focus™) and the traditional technique in total thyroidectomy.
Methods
From October 2008 through May 2010, 240 adult patients affected by benign thyroid disease were operated in our University General Surgery Department. This is a retrospective case-matched study of all total thyroidectomies. Study’s patients were divided into three groups. All patients were scheduled for total thyroidectomy at the Surgical Department of Chieti-Pescara, G.D’Annunzio University in Italy. The study’s patients were introduced into three groups according to the hemostatic technique: conventional technique of tying and knots (C), Focus® (F) (Focus® Ethicon Endosurgery, Johnson & Johnson, USA) and the Ligasure Precise® (L), specific for thyroid surgery.
In order to obtain groups which were more homogeneous, patients with neoplastic disease and relapse (reoperation) were not included in the study because both cases require more complex surgical procedures, thus eliminating a confounding factor. For the same purpose we also excluded the use of clips which have been shown to reduce the duration of surgical procedures7. These were the only exclusion criteria which were adopted in the study.
The Ligasure, is used, very often by the surgeons in other branches of general surgery such as the abdomen surgery, where named with the generic name of the device; Ligasure Vessel Sealing System®. The physical principle that is used by F is ultrasonic energy; L makes use of radiofrequency. All procedures were performed by the same surgical team specialized in endocrine surgery. Authors do not use neuromonitoring of the recurrent laryngeal nerve. The study was composed of 47 male and 193 female patients, with a mean age of 51 years.
The parameters that have been evaluated in each of 240 patients were: Preoperatively: age, gender, diagnosis, thyroid hormones (TSH, T3 and T4), PTH and calcium levels. During the operation: duration of the operation (measured in minutes), complications and weight of the thyroid gland removed.
Postoperatively: complications, body’s temperature, calcium levels in the 1st, 2nd and 3rd postoperative day, hospital stay and finally presence or absence of dysphonia. The F group, consisted of 14 patients with retrosternal multinodular goiter, 60 patients with multinodular goiter and 6 patients with Graves’ disease. The L group, consisted of 18 patients with retrosternal multinodular goiter, 53 patients with multinodular goiter and 9 patients with Graves’ disease. The C group, was composed of 15 patients with retrosternal multinodular goiter, 56 patients with multinodular goiter and finally 9 patients with Graves’ disease.
For retrosternal goiter authors intend a goiter with mediastinal immersion by a minimum of two centimeters (2 cm), with patient’s neck in hyperextension.
Preoperative levels of thyroid hormones (TSH, T3 and T4) in the 3 groups of patients were normal (including the Graves’ disease patients, who had been previously treated pharmacologically and become euthyroid). PTH was also normal.
All patients underwent total thyroidectomy “in principle” for benign thyroid disease with laryngeal nerve preparation and identification, with preservation of at least 3 parathyroid glands. A drainage was always used after total thyroidectomy and was removed after 24 h. The thyroid glands were weighed before being immersed in formalin. All patients were monitored for 15 days and at three months, six months, one year and two years after the operation, with a mean follow-up period of two years. In all patients, the assessment of the motility of the vocal cords was performed pre-operatively and postoperatively with laryngoscopy. Postoperatively, laryngoscopy was difficult in 13 patients of our series, because it was not well tollerated.
Postoperative calcemia:
Ionized calcemia was tested every day until hospital discharge. All patients with postoperative calcium levels below the lower limit of normal range (8 mg/dL) were considered as having hypocalcemia and received oral calcium carbonate and vitamine D3 supplementation. Clinical hypocalcemia was defined as ionized calcium below 1.14 mmol/l associated to positive Chvostek’s sign or patient complaint of paresthesia.
Statistical analysis:
Quantitative variables (age, calcium level, operative time, gland weight and hospital stay) were expressed as mean ± standard deviation (SD). Qualitative variables (gender and diagnosis) were given as frequency and percentage. The results were reported separately for each of the three groups.
Statistical analysis was performed using non-parametric tests (Shapiro-Wilk test) because distributions were not normal.
Statistical significance between group differences for qualitative variables was assessed using Chi-squared test or Fischer’s Exact Test, where appropriate. Kruskal-Wallis test was applied to assess the comparison of the quantitative variables between the three groups. The comparison of ligasure and focus groups vs control group was evaluated using Kruskal-Wallis post-hoc test.
All statistical tests were evaluated at an alpha level of 0.05. Statistical analysis was performed using SPSS’ Advanced Statistical 11.0 software (SPSS Inc, Chicago, Illinois, USA).
Results
Total thyroidectomy was completed in all patients. There were no mortalities, cases of intra- or post-operative hemorrhage, cervical hematomas or wound infections.
The three groups did not present statistically significant differences in terms of age, gender, pathology or weight of thyroid gland (Tables 1, 2).
Patients were well matched for age, gender, pathology, and weight of the thyroid gland and no significant difference among the three groups was detected as reported in Tables 1 and 2 (p>0.05).
Group differences in pre-operative calcemia were not statistically significant and were located into the normal range. Preoperative calcium levels in all patients in all the three study’s groups are shown in Table 1.
Table 1. Patients’ demographics and laboratory measurements.
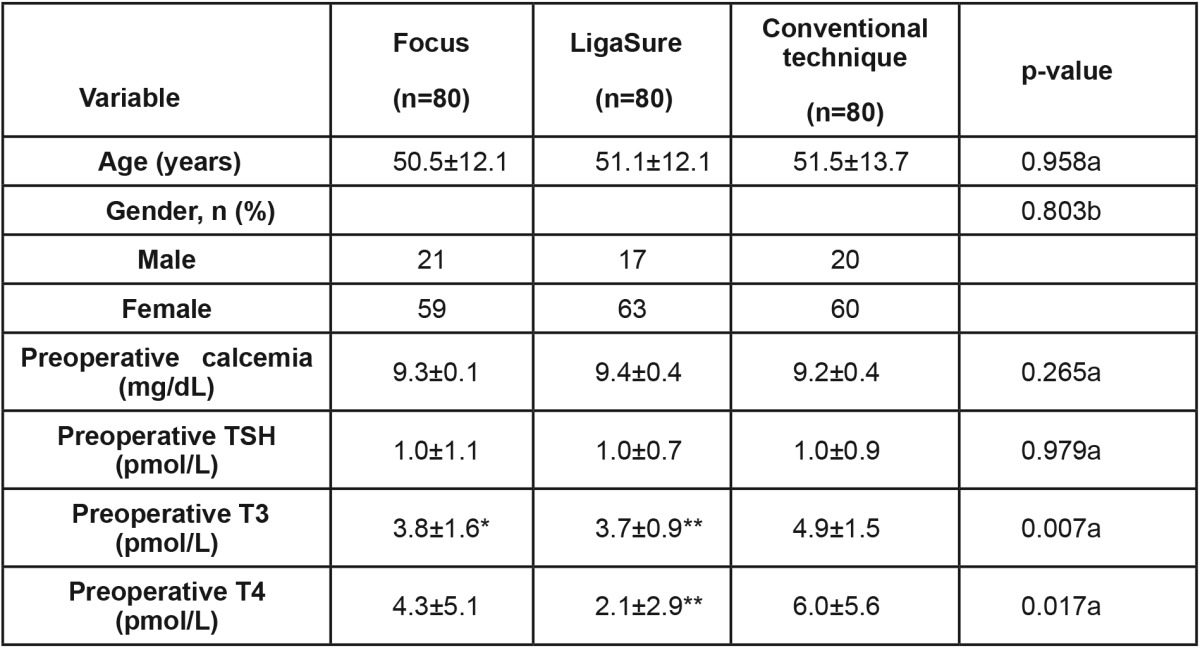
All P<0.05, are reported for statistical significance. a Kruskal-Wallis test; b Chi square test; * p<0.05; ** p<0.01 post hoc test vs control group (conventional technique group). SD: Standard Deviation, range
There was no statistically significant difference in postoperative hypocalcemia between patients operated with conventional technique versus newer devices.
Hypocalcemia in all other patients was resolved within 30 days following medical treatment.
The duration of surgery was significantly reduced by 15% (Kruskal-Wallis test: p=0.019) in Group F compared to the C group, while the difference between Groups L and C did not reach statistical significance (Table 2).
Table 2. Diagnosis and results (operative time and weight of the excised gland).
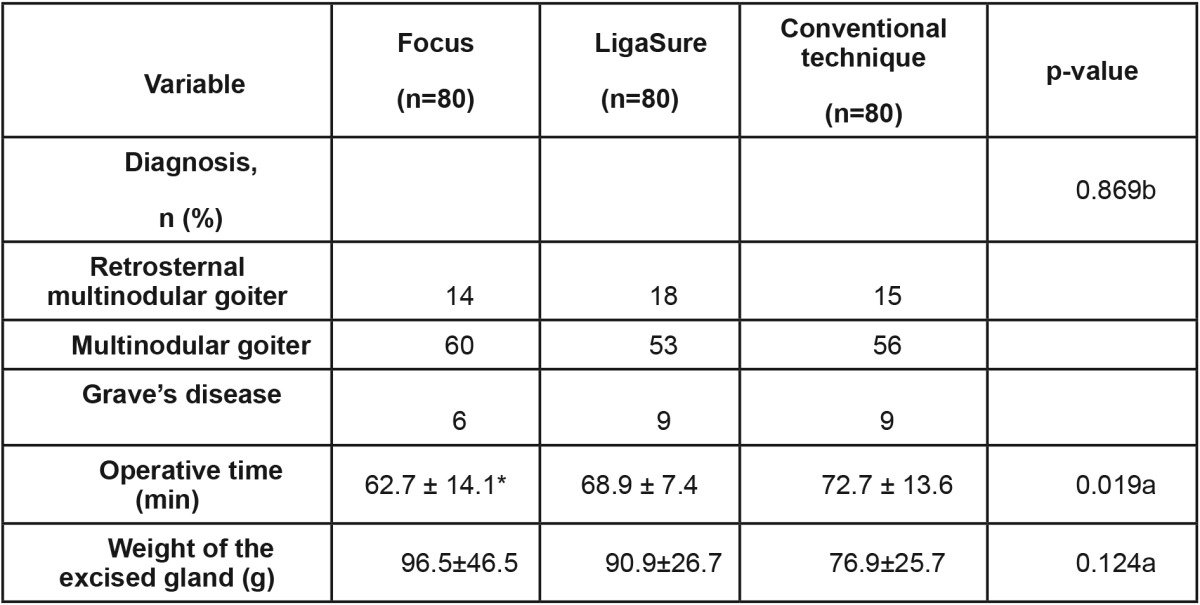
All p<0.05, are reported for statistical significance. a Kruskal-Wallis test; b Chi square test; * p<0.05; ** p<0.01 post hoc test vs control group (conventional technique group). SD: Standard Deviation, range
In fact, in the F group the surgical time was shorter 62.7±14.1 minutes, while in the conventional technique (C group) it was 72.7±13.6 minutes. The L group had an intermediate surgical time of 68.9±7.4 minutes.
Differences in mean post-operative hospital stay were not statistically significant (mean 2 days).
The statistical elaboration demonstrates that the incidence of transient hypocalcemia was of 24.5%. There were not statistically significant differences in the incidence of transient hypocalcemia in the three groups of study. From 59 patients who experienced transient hypocalcemia, only 8 of them had clinical symptoms. Three cases of permanent hypoparathyroidism, continued postoperatively for six months, were found; two cases in the C group and another case in the F group (1.2 % of the study’s patients), (p>0.05).
Ten temporary palsies of the recurrent laryngeal nerve occurred (four in the F group, three in the L group and three other cases in the C group), with full recovery in three months (4.1 % of all cases), (p>0.05). There was no case of permanent laryngeal nerve palsy; that derives from the accurate and precise surgical technique of our university team and mostly from knowledge and recognition of anatomical structures.
Discussion
Total thyroidectomy requires a rigorous surgical technique in order to identify and respect pertinent anatomical structures. A strict control of hemostasis is required in order to avoid serious complications and to reduce the incidence of common post-operative complications involving recurrent laryngeal nerve and parathyroid glands.
The use of vascular dissecting and sealing devices is common in thyroid surgery8 and reported to be safe and useful9,10.
Ligasure permits dissection in situations where Harmonic Scalpel presents difficulties. The latter has the advantage of directly cutting the tissue after its application while the former requires the use of scissors. Ligasure is also capable of hemostasis of blood vessels up to 7 mm in diameter with a thermal damage limited to 2-3 mm while Harmonic Scalpel can seal vessels up to 3 mm with 2 mm of thermal damage11,12. The advantage of using these instruments with respect to traditional techniques is essentially the reduction in the duration of the surgical procedure13, while the incidence of complications is not modified14.
Recently, a new ultrasound scissor (Harmonic FocusTM) was introduced. The main advantages offered by this device are that it can easily dissect tissue and has an ergonomic design, similar to traditional instruments, rendering it comfort and easier-to-use. It also has an acoustic signal and is capable of coagulating vessels up to 5 mm in diameter.
The aim of this study was to compare the results obtained using three techniques: an electrothermal bipolar vessel sealing system (Ligasure®), a harmonic curved shears (Harmonic Focus™) and the traditional technique in total thyroidectomy.
The three groups were also homogeneous for presenting pathology, age and gender as well as weight of thyroid gland. Hemorrhagic complications were not seen in any patients. In fact, meticulous hemostasis is the basis of correctly performing a surgical procedure. These devices cannot substitute a rigorous technique but only improve the practicality of the surgery. In fact, experienced surgeons have no more complications and a shorter learning curve15,16.
The hemorrhagic complications reported for the most part involve the superior thyroid artery and can have serious consequences, even if these complications mostly occur with the Harmonic Scalpel14.
The most common complication following total thyroidectomy is hypocalcemia. Previous studies reported differing results. Foreman17 reported a decreased incidence with the use of Harmonic scalpel while Pons18 did not report any differences.
Our results did not indicate statistically significant differences in the incidence of complications between the three groups. Only three patients who underwent total thyroidectomy (two with the traditional technique and another one with the focus), had hypocalcemia after six months.
We did have ten cases of temporary palsy of the recurrent laryngeal nerve which resolved within 60 days. However, there was no permanent palsy of the recurrent laryngeal nerve. An increased incidence was initially reported by Marchesi19 when the Harmonic Scalpel was first introduced. But as surgeons gained experience with its use and considering the theoretical limits of the lateral thermal damage induced, this case does not represent anymore a common event20.
Our results indicate a statistically significant reduction in duration of surgery in Group F of approximately 15% with respect to the group C. Group L had a reduced duration compared to Group C but this difference was not statistically significant. In addition, no statistical significance comparing group L to F, was observed.
Our previous experience with the Harmonic Scalpel was not completely positive. The major drawbacks were the length of the handle and a lack of dissecting capacity which gave us the impression that this device was not adapt for routine use but probably more adapt for mini-invasive thyroid surgery21.
In regards to the Ligasure Precise, it seems to be a reliable device, which is easy to learn and is also technically straightforward in its use. Given its similarity with other ultrasound hemostatic devices, the learning curve of the LigaSure should be considered minimal15.
Some authors of that study, had an initial experience with these devices which originated from an inferior number of enrolled patients. Their first results, represented authors’ premature experience with the devices which had just demonstrated a reduction in the operative time in the group operated with focus . Although, the restricted arm of the study, which enrolled a small number of patients did not offer any validity of the results, to permit generalization and abstraction of safe conclusions22.
The new FocusTM scissors has introduced numerous advantages to ultrasound devices: it is easier to handle and dissects well while maintaining the advantage of coagulating while cutting. These characteristics are probably responsible for the reduction in duration of surgery we observed.
It seems evident that important steps in the evolution of all branches of surgery, including endocrine surgery of the thyroid, can be achieved with the refinement of surgical technologies through the application of the appropriate devices.
Previously reported analyses of economic comparisons of these techniques have not yielded concordant results. Some authors reported an increased cost associated with the use of these devices23 while others have not24. The major obstacle in this type of analysis is the identification of objective economic parameters for differing hospital and health care system settings. The possibility of a temporary increased use of the operating theater is a factor to be considered, especially in centers with a high affluence of highly specialized procedures.
An important observation that derives from our experience in endocrine surgery is that there is a tendency to avoid the use of such devices in those thyroidectomies considered “easier” to perform where operating times are content with the conventional technique. It seems more appropriate to use the new devices in these thyroidectomies that are considered “more demanding” from the operators, such as: Large goiters and / or mediastinal immersion. This tendency is justified in part, by the relatively high cost of the new surgical instruments in thyroid surgery, which requires their use with rational criteria; that would seem to indicate an operation with the conventional technique, if the thyroid is easy to operate, and make use of the new “devices” in more voluminous thyroid glands that require substantially more difficult and longer operations.
Our experience shows that both Focus and Ligasure Vessel Sealing System, have a good practical use. The only real advantage of the new “devices” in thyroid surgery is the time saving, that should offset the higher expenditure. In our study there was no improvement in postoperative hypocalcemia. Finally, many authors argue that in their series the latest surgical devices were also effective in reducing the severity of postoperative hypocalcemia, an event that we did not observe in our study25, we indeed found an homogeneous distribution of postoperative complications in the 3 groups of patients without statistically significant differences.
Conflict of Interest:
Authors declare no conflict of interest.
References
- 1.Friguglietti CU, Lin CS, Kulcsar MA. Total thyroidectomy for benign thyroid disease. Laryngoscope. 2003;113:1820–1826. doi: 10.1097/00005537-200310000-00030. [DOI] [PubMed] [Google Scholar]
- 2.Ortega J, Sala C, Flor B, Lledo S. Efficacy and cost-effectiveness of the UltraCision harmonic scalpel in thyroid surgery: an analysis of 200 cases in a randomized trial. J Laparoendosc Adv Surg Tech A. 2004;14:9–12. doi: 10.1089/109264204322862289. [DOI] [PubMed] [Google Scholar]
- 3.Lombardi CP, Raffaelli M, Cicchetti A, Marchetti M, De Crea C, Di Bidino R, et al. The use of “harmonic scalpel” versus “knot tying” for conventional “open” thyroidectomy: results of a prospective randomized study. Langenbecks Arch Surg. 2008;393:627–631. doi: 10.1007/s00423-008-0380-9. [DOI] [PubMed] [Google Scholar]
- 4.Yao HS, Wang Q, Wang WJ, Ruan CP. Prospective clinical trials of thyroidectomy with LigaSure vs conventional vessel ligation: a systematic review and meta-analysis. Arch Surg. 2009;144:1167–1174. doi: 10.1001/archsurg.2009.201. [DOI] [PubMed] [Google Scholar]
- 5.Cirocchi R, D’Ajello F, Trastulli S, Santoro A, Di Rocco G, Vendettuoli , et al. Meta-analysis of thyroidectomy with ultrasonic dissector versus conventional clamp and tie. World J Surg Oncol. 2010;8:112. doi: 10.1186/1477-7819-8-112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sartori PV, De Fina S, Colombo G, Pugliese F, Romano F, Cesana G, et al. Ligasure versus ultracision in thyroid surgery: a prospective randomized study. Langenbecks Arch Surg. 2008;393:655–658. doi: 10.1007/s00423-008-0386-3. [DOI] [PubMed] [Google Scholar]
- 7.Seiler CM, Frohlich BE, VeitJA G, Gazyakan E, Wente MN, Wollermann C, et al. Protocol design and current status of CLIVIT: a randomized controlled multicenter relevance trial comparing clips versus ligatures in thyroid surgery. Trials. 2006;7:27. doi: 10.1186/1745-6215-7-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Goretzki PE, Schwarz K, Lammers BJ. Implementing the general use of dissection devices in thyroid surgery from prospective randomized trial to daily use. Surg Technol Int. 2009;18:86–92. [PubMed] [Google Scholar]
- 9.Cordon C, Fajardo R, Ramirez J, Herrera MF. A randomized, prospective, parallel group study comparing the harmonic scalpel to electrocautery in thyroidectomy. Surgery. 2005;137:337–341. doi: 10.1016/j.surg.2004.09.011. [DOI] [PubMed] [Google Scholar]
- 10.Franco J, Kish KJ, Pezzi CM, Pak H, Kukora JS. Safely increasing the efficiency of thyroidectomy using a new bipolar electrosealing, device (LigaSure) versus conventional clamp and tie technique. Am Surg. 2006;72:132–136. [PubMed] [Google Scholar]
- 11.Landman J, Kerbl K, Rehman J, Andreoni C, Humphrey PA, Collyer W, et al. Evaluation of a vessel sealing system, bipolar electrosurgery, harmonic scalpel, titanium clips, endoscopic gastrointestinal anastomosis vascular staples and sutures for arterial and venous ligation in a porcine model. J Urol. 2003;169:697–700. doi: 10.1097/01.ju.0000045160.87700.32. [DOI] [PubMed] [Google Scholar]
- 12.Goldstein SL, Harold KL, Lentzner A, Matthews BD, Kercher KW, Sing RF, et al. Comparison of thermal spread after ureteral ligation with the Laparo-Sonic ultrasonic shears and Ligasure system. J Laparoendosc Adv Surg Tech A. 2002;12:61–63. doi: 10.1089/109264202753486957. [DOI] [PubMed] [Google Scholar]
- 13.Manouras A, Lagoudianakis EE, Antonakis PT, Filippakis GM, Markogiannakis H, Kekis PB. Electrothermal bipolar vessel sealing system is a safe and time-saving alternative to classic suture ligation in total thyroidectomy. Head Neck. 2005;27:959–962. doi: 10.1002/hed.20271. [DOI] [PubMed] [Google Scholar]
- 14.Manouras A, Markogiannakis H, Koutras AS, Antonakis PT, Drimousis P, Lagoudianakis EE, et al. Thyroid surgery: comparison between the electrothermal bipolar vessel sealing system, harmonic scalpel and classic suture ligation. Am J Surg. 2008;195:48–52. doi: 10.1016/j.amjsurg.2007.01.037. [DOI] [PubMed] [Google Scholar]
- 15.Kiriakopoulos A, Dimitrios T, Dimitrios L. Use of a diathermy system in thyroid surgery. Arch Surg. 2004;139:997–1000. doi: 10.1001/archsurg.139.9.997. [DOI] [PubMed] [Google Scholar]
- 16.Rosato L, Avenia N, Bernante P, De Palma M, Gulino G, Nasi PG, et al. Complications of thyroid surgery: analysis of a multicentric study on 14.934 patients operated on in Italy over 5 years. World J Surg. 2004;28:271–276. doi: 10.1007/s00268-003-6903-1. [DOI] [PubMed] [Google Scholar]
- 17.Foreman E, Aspinall S, Bliss RD, Lennard TW. The use of the harmonic scalpel in thyroidectomy: ‘beyond the learning curve’. Ann R Coll Surg Engl. 2009;91:214–216. doi: 10.1308/003588409X391811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pons Y, Gauthier J, Ukkola-Pons E, Clément P, Roguet E, Poncet JL, et al. Comparison of ligasure vessel sealing system, harmonic scalpel and conventional hemostasis in total thyroidectomy. Otorinolaringol Head Neck Surg. 2009;141:496–501. doi: 10.1016/j.otohns.2009.06.745. [DOI] [PubMed] [Google Scholar]
- 19.Marchesi M, Biffoni M, Cresti R, Mulas MM, Turriziani V, Berni A, et al. Ultrasonic scalpel in thyroid surgery. Chir Ital. 2003;55:299–308. [PubMed] [Google Scholar]
- 20.Dionigi G. Energy based devices and recurrent laryngeal nerve injury: the need for safer instruments. Langenbecks Arch Surg. 2009;394:579–580. doi: 10.1007/s00423-008-0454-8. [DOI] [PubMed] [Google Scholar]
- 21.Miccoli P, Berti P, Dionigi G, D’Agostino J, Orlandini C, Donatini G. Randomized controlled trial of harmonic scalpel use during thyroidectomy. Arch Otolaryngol Head Neck Surg. 2006;132:1069–1073. doi: 10.1001/archotol.132.10.1069. [DOI] [PubMed] [Google Scholar]
- 22.Di Rienzo RM, Bove A, Bongarzoni G, Palone G, Corradetti L, Corbellini L. Comparison of conventional technique, Ligasure Precise and Harmonic Focus in total thyroidectomy. G Chir. 2010;31:296–298. [PubMed] [Google Scholar]
- 23.Sebag F, Fortanier C, Ippolito G, Lagier A, Auquier FPJ, Henry JF. Harmonic scalpel in multinodular goiter surgery: impact on surgery and cost analysis. J Laparoendosc Adv Surg Tech A. 2009;19:171–174. doi: 10.1089/lap.2008.0043. [DOI] [PubMed] [Google Scholar]
- 24.Leonard DS, Timon C. Prospective trial of the ultrasonic dissector in thyroid surgery. Head Neck. 2008;30:904–908. doi: 10.1002/hed.20805. [DOI] [PubMed] [Google Scholar]
- 25.Oussoultzoglou E, Panaro F, Rosso E, Zeca I, Bachellier P, Pessaux P, et al. Use of BiClamp Decreased The severity of hypocalcemia after total thyroidectomy Compared with LigaSure: a prospective study. World J Surg. 2008;32:1968–1973. doi: 10.1007/s00268-008-9671-0. [DOI] [PubMed] [Google Scholar]