

Abstract
Introduction: The issue of evaluating the efficiency of health systems has been elaborated upon frequently. Since “health” is a multi-faceted concept, many variables of different measurement units must be included in its analysis; consequently, this presents a great obstacle for researchers to overcome.
Materials and Methods: A novel statistical approach for evaluating the efficiency of organizational units is here proposed, which can also be easily applied to the health sector. For these purposes, the health status of the 27 countries belonging to the European Union has been examined by employing a statistical Ivanovic-Jeremic Distance Based Analysis (DBA) on various health indicators.
Results: The subsequent outcome of the Distance Based Analysis has shown that Cyprus and Ireland have a most efficient health system sectors. Greece also has exceptional indicators of health service, yet health on the individual level is not comparable.
Limitations: Since it synthesizes many variables into an efficiency score, a DBA can be easily applied to other regions/countries. However, the choice of input and output variables can be considered to be potential limitations since a different choice of variables may cause different efficiency scores for the countries selected.
Conclusions: A DBA approach contributes significantly to the efficiency in the field of research measurement. This analysis can be additionally performed alongside DEA and SFA methods, as a new measure of efficiency.
Keywords: health system evaluation, statistical methods, hospital efficiency
Evaluating the efficiency of organizational units has always represented quite a challenge for researchers. Many papers are particularly focused on evaluating the socio-economic efficiency of countries/regions1. Since health is considered to be a fundamental contributor to the welfare of every country2, the performance of a country’s health system must be thoroughly evaluated3-7. In order to rank countries, researchers often have used their mortality rates as an indicator of their health system performance8. However, this approach assumes that health is a one-dimensional concept which is not precisely accurate. Indeed, the definition of health by the WHO suggests that it is a multi-faceted concept2.
In order to evaluate health system efficiency, WHO health indicators must be divided into two groups: input and output. Input indicators represent health services such as the number of physicians per 10,000 inhabitants, a government’s per capita expenditure on health, etc… Conversely, output indicators represent the health of individuals, such as mortality rate(s), life expectancy, HALE. The aim of this study is to present the Ivanovic-Jeremic Distance Based Analysis (DBA) as a new measure of efficiency. Utilizing this distance based method shall allow for the implementation of a large number of input and output variables in the actual analysis, and shall determine which countries make appropriate use of their health service resources.
Materials and Methods
Quite often, the ranking of specific marks is done in such a way that it can seriously affect the process of taking exams, sport competitions, UN participation, University ranking, medicine selection, and many others aspects reliant upon their rankings9-13.
I-distance is a metric distance in an n-dimensional space. It was first proposed and defined by B. Ivanovic, and has appeared in various publications since 196314. Ivanovic devised this method to rank countries according to their level of development on the basis of several indicators. Many socio-economic development indicators were originally considered and the problem was how to use all of them in order to calculate a single synthetic indicator which would thereafter represent the rank.
For a selected set of variables XT= (X1, X2, … Xk) chosen to characterize the entities, the I-distance between the two entities er = (x1r,x2r,…,xkr) and es = (x1s,x2s,…,xks) is defined as where di(r,s) is the distance between the values of variable Xi for er and es, e.g. the discriminate effect, di(r,s) = xir – xis , i∈{1, ... , k} (2) σi the standard deviation of Xi, and rji.12..j-1 is a partial coefficient of the correlation between Xi and Xj, (j<i),9,12.
Table 1. The Results of the I-distance Method, I-distance Values and Rank for Input Variables (Indicators of Health Services).

The construction of the I-distance is iterative; it is calculated through the following steps:
- Calculate the value of the discriminate effect of the variable X1 (the most significant variable, that which provides the largest amount of information on the phenomena that are to be ranked)
- Add the value of the discriminate effect of X2 which is not covered by X1
- Add the value of the discriminate effect of X3 which is not covered by X1 and X2
- Repeat the procedure for all variables15-18.
In order to rank the entities (in this case, countries), it is necessary to have one entity fixed as a referent in the observing set using the I-distance methodology. The entity with the minimal value for each indicator, a fictive maximal, or an average value entity can be set up as the referent entity. The ranking of entities in the set is there based on the calculated distance from the referent entity19.
The basic idea of this paper is to present a novel DBA approach as a new measure of efficiency. In that, the I-distance method shall be applied to several Input indicators and their I-distantinput values calculated. The same approach shall be applied to Output indicators and I-distantoutput values will be calculated as well. The obtained values are to be brought to 0-1 level by implementing a L∞ norm. The efficiency of a country’s health system will be then calculated as the Ef=I-distantoutput/I-distantinput Any health system with an efficiency ratio of at least 1 is to be considered as efficient. As an example dataset, attention shall be focused on evaluating the health status of countries within the European Union.
Results
The selection of indicators has been done in order to reflect the health of individuals, as well as the quality of health services. Variables representing the quality of health services are the input variables by all means, while the health of the individual represents the output variables. Those variables representing the indicators of health services (Input) used in this study are: (I1) the number of dentists per 10,000 people, (I2) the number of nurses per 10,000 people, (I3) the number of physicians per 10,000 people, (I4) the number of pharmacists per 10,000 people, (I5) the number of hospital beds per 10,000 people, (I6) per capita government expenditure on healthcare (PPP int. $), and (I7) per capita total expenditure on health (PPP int. $). On the other hand, the health of the individual (Output) is represented by the following variables: (O1) healthy life expectancy, (O2) life expectancy at birth, (O3) the mortality rate in adults, (O4) the under-5 mortality rate, (O5) the infant mortality rate, and (O6) the mortality rate in mothers. In line with previous research on the subject of evaluating a nation’s health status2,18, data from the Statistical Information System of the World Health Organization20 has also been included in this evaluation.
The results achieved through the use of the I-distance ranking method for the Input variables are presented in Table 1.
Table 1. The Results of the I-distance Method, I-distance Values and Rank for Input Variables (Indicators of Health Services).
As shown in Table 1, Greece ranks first among EU countries, while Belgium and Luxembourg are placed slightly lower. From all ranked EU countries, these invest the most in their respective health sectors and have the largest number of physicians per 10,000 inhabitants. Conversely, Poland and Romania are at the bottom of the list. In order to fully understand these rankings, it is essential to clarify which input variables are the most important when evaluating a country’s health service. Hence, the data set was further examined, and a correlation coefficient of each variable with its I-distance value was determined. The results of this further analysis show that the most significant variable for evaluating a country’s health service performance is its number of physicians per 10,000 inhabitants, with r=.769, p<.01. This finding is in accordance with previous research which establishes a country’s number of physicians as being a crucial health system performance indicator21.
After applying the I-distance method to the Input variables, the same procedure was then performed on a set of Output variables that represent health indicators of individual health and the I-distance values for the Output variables were calculated. These results are presented in Table 2.
Table 2. The Results of the I-distance Method, I-distance Values and the Rank for Output Variables (Indicators of Health of the Individual).
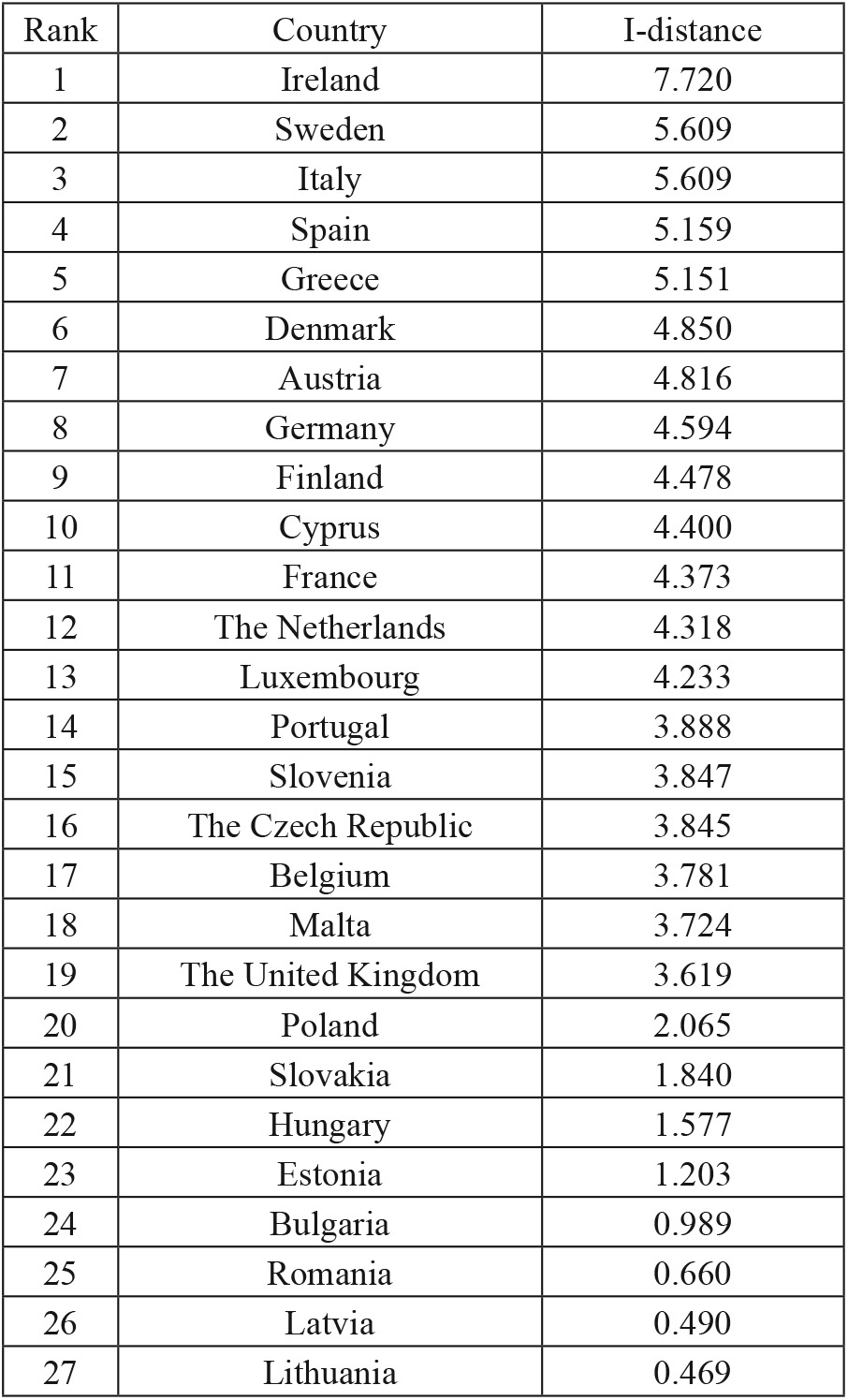
As shown in Table 2, Ireland tops the list of “healthiest countries” in the EU. Sweden and Italy are tied closely behind in second and third place, respectively. On the other hand, Bulgaria, Romania, Latvia and Lithuania are placed lowest. In order to better understand these rankings, it is essential to determine the most important variables in evaluating the health of the individual. Thus, this data set was further examined and a correlation coefficient of each variable with its I-distance value was determined. As it appears, the most significant variables in determining a country’s health status are Life Expectancy at Birth and Healthy Life Expectancy (HALE), with r=.922, p<.01 and r=.872, p<.01, respectively. This result is far from surprising: various papers have elaborated on the importance of life expectancy and HALE in determining a country’s health system performance22,23.
Nonetheless, a crucial point of this paper is to evaluate the efficiency of a country’s health system. In order to do so, each country’s Output I-distance value was divided by its Input I-distance value (values are first corrected with a L∞ norm); the results of which are presented in Table 3.
Table 3. The Efficiency of Health Systems among EU Countries.
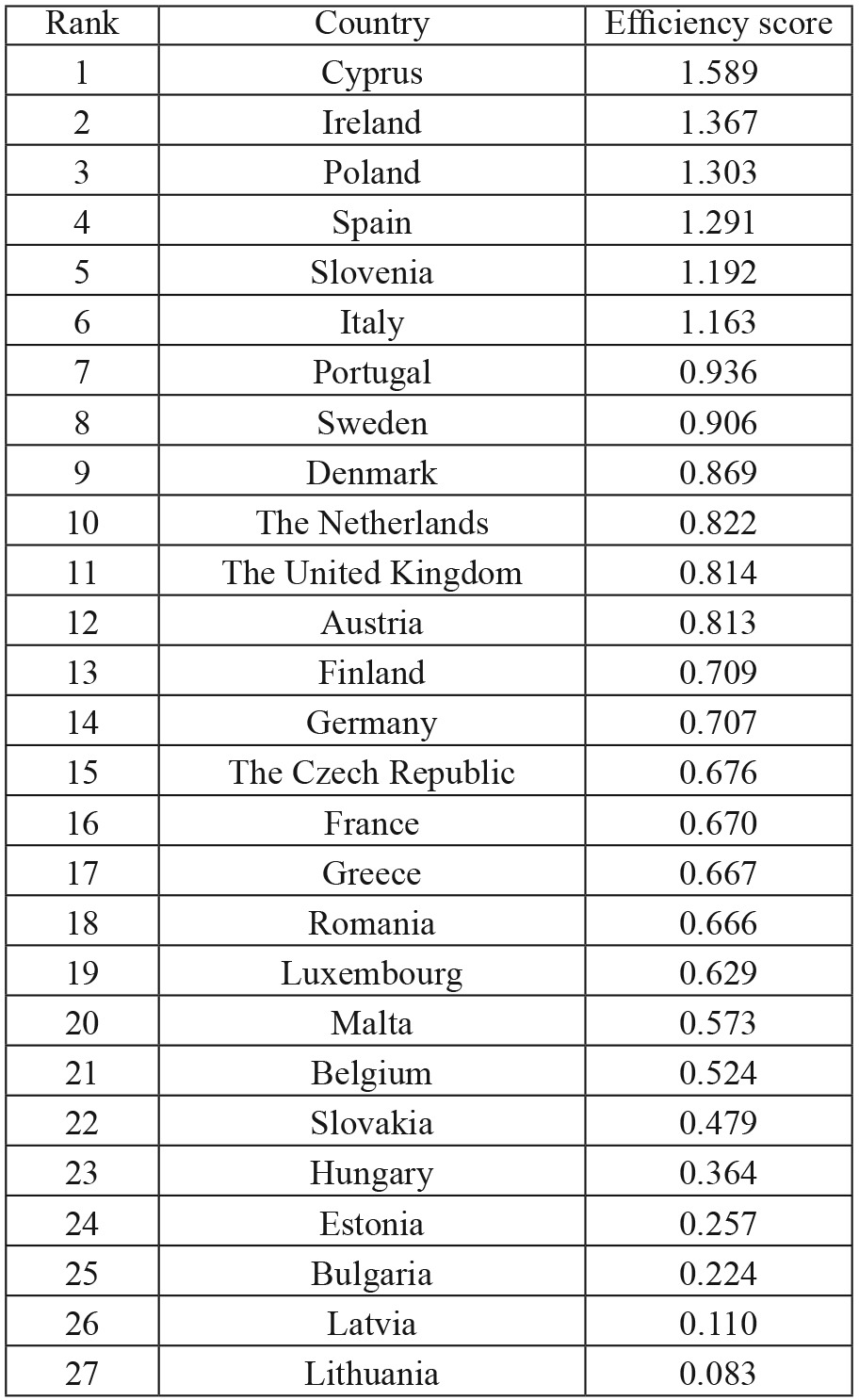
As can be observed, Cyprus ranks as the most efficient country in terms of its health system. The principal reason behind this ranking lies in the fact that Cyprus has very poor health service indicators (ranked at 25th), as well as a quite high rank for health of the individual (ranked at 10th). It is evident that with poor health service indicators - such as 23 physicians per 10,000 inhabitants (the EU average is 33) - Cyprus has tried its best. Particularly interesting is the finding that Cyprus has exceptionally long life expectancy, something which has mostly been attributed to its Mediterranean diet24. Still, Cyprus has to dramatically improve its health service indicators25. In opposition to Cyprus, Belgium has a quite low efficiency value in comparison to its astonishing input variables: its health service indicators are ranked 2nd; yet, its output is low, as the health of the individual is ranked 17th. As a possibility to improve their efficiency, the authors of this paper would like to note the need for Belgium to improve their IT systems, especially in regard to their general hospitals26.
Conclusion
In this paper, the aim has been to evaluate the health system performances of European Union countries by applying an Ivanovic-Jeremic distance based analysis. The results have clearly shown a great disparity between EU members. Indeed, Scandinavian and Western Europe countries lead the way in health service indicators, but fail to transpose them into an adequate level of health on the level of the individual. On the other hand, newly integrated members from Eastern and South-eastern Europe have huge problems in reaching the high EU standards of health service indicators.
There are several contributions which must be singled out:
First of all, by utilizing the approach presented in this work, it is possible to evaluate every country’s health system performance. Moreover, not only is a ranking provided, but so is the difference between countries. A large number of variables can be included in the analysis, generating one aggregated quantitative indicator. In addition to the above mentioned contributions, it should be noted that DBA has provided information as to which input variables are crucial for determining a country’s health system performance. Thus, each country can re-evaluate its health system performance and try to improve its ranking by further developing the most significant indicators of its own health status.
Finally, a completely new model for evaluating the efficiency of any organizational unit has been presented in this paper. This model has many advantages, but its primary is the possibility to implement a large number of variables that are of various units of measure. Therein, this model can significantly contribute to the field of efficiency measurement. Currently, the majority of research papers employ DEA and SFA as efficiency measurement methods27-30. However, DBA possesses numerous advantages over these two methods, as it does not place any weighting factor on variables (DEA) or is based on dissimilar assumptions about the distribution of the inefficiency term u.
It is hoped that this paper shall contribute to the growing studies of evaluating health system performance31 and provide a foundation in the integration of the DBA approach into DEA and SFA methodology.
Acknowledgments
This work has been done in cooperation with and as a project funded by the Serbian Ministry of Science and Technological Development, contract no. 41023.
References
- 1.Martic M, Savic G. An application of DEA for comparative analysis and ranking of regions in Serbia with regards to social-economic development. Eur J Oper Res. 2011;132:343–356. [Google Scholar]
- 2.Al-Lagilli S, Jeremic V, Seke K, Jeremic D, Radojicic Z. Evaluating the health of nations: a Libyan perspective. Libyan J Med. 2011;6:6021. doi: 10.3402/ljm.v6i0.6021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pijalovic V, Kudumovic M. Analysis of health expenditure in the EU8 countries and Bosnia and Herzegovina. HealthMED. 2010;4:819–828. [Google Scholar]
- 4.Garman A, McAlearney AS, Harrison M, Song P, McHugh M. High-performance work systems in health care management, Part 1: Development of an evidence-informed model. Health Care Manage Rev. 2011;36:201–213. doi: 10.1097/HMR.0b013e318201d1bf. [DOI] [PubMed] [Google Scholar]
- 5.McAlearney AS, Garman A, Song P, McHugh M, Robbins J, Harrison M. High-performance work systems in health care management, Part 2: Qualitative evidence from five case studies. Health Care Manage Rev. 2011;36:214–226. doi: 10.1097/HMR.0b013e3182100dc4. [DOI] [PubMed] [Google Scholar]
- 6.Munkhsaikhan S, Tsai AC, Chang MC. Technical efficiency of public hospitals in Mongolia. HealthMED. 2011;5:360–365. [Google Scholar]
- 7.Nuti S, Daraio C, Speroni C, Vainieri M. Relationships between technical efficiency and the quality and costs of health care in Italy. Int J Qual Health Care. 2011;23:324–330. doi: 10.1093/intqhc/mzr005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nolte E, McKee C. Measuring the health of nations: Updating an earlier analysis. Health Affair. 2008;27:58–71. doi: 10.1377/hlthaff.27.1.58. [DOI] [PubMed] [Google Scholar]
- 9.Ivanovic B. A method of establishing a list of development indicators. Paris. United Nations educational, scientific and cultural organization. 1973 [Google Scholar]
- 10.Ivanovic B, Fanchette S. Grouping and ranking of 30 countries of Sub-Saharan Africa, Two distance-based methods compared. Paris. United Nations educational, scientific and cultural organization. 1973 [Google Scholar]
- 11.Jeremic V, Radojicic Z. A New Approach in the Evaluation of Team Chess Championships Rankings. J Quant Anal Sports. 2010;6: Article 7 [Google Scholar]
- 12.Jeremic V, Bulajic M, Martic M, Radojicic Z. A fresh approach to evaluating the academic ranking of world universities. Scientometrics. 2011;87:587–596. [Google Scholar]
- 13.Jeremic V, Markovic A, Radojicic Z. ICT as crucial component of socio-economic development. Manage. 2011;16:5–9. [Google Scholar]
- 14.Ivanovic B. Classification Theory. Belgrade. Institute for Industrial Economic. 1977 [Google Scholar]
- 15.Mihailovic N, Bulajic M, Savic G. Ranking of banks in Serbia. YUJOR. 2009;19:323–334. [Google Scholar]
- 16.Jeremic V, Isljamovic S, Petrovic N, Radojicic Z, Markovic A, Bulajic M. Human development index and sustainability: What’s the correlation? Metal Int. 2011;16:63–67. [Google Scholar]
- 17.Jeremic V, Vukmirovic D, Radojicic Z, Djokovic A. Towards a framework for evaluating ICT infrastructure of countries: a Serbian perspective. Metal Int. 2011;16:15–18. [Google Scholar]
- 18.Jeremic V, Seke K, Radojicic Z, Jeremic D, Markovic A, Slovic D, et al. Measuring health of countries: a novel approach. HealthMED. 2011;6:1762–1766. [Google Scholar]
- 19.Knezevic S, Jeremic V, Zarkic-Joksimovic N, Bulajic M. Evaluating the Serbian banking sector: a statistical approach. Metal Int. 2012;17:171–174. [Google Scholar]
- 20.World Health Organization statistical information system. WHO. 2010 [Google Scholar]
- 21.White H, Glazier RH. Do hospitalist physicians improve the quality of inpatient care delivery? A systematic review of process, efficiency and outcome measures. BMC Med. 2011;9 Article 58 doi: 10.1186/1741-7015-9-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Karim SA, Eikembo TA, Bambra C. Welfare state regimes and population health: Integrating the East Asian welfare states. Health Policy. 2010;94:45–53. doi: 10.1016/j.healthpol.2009.08.003. [DOI] [PubMed] [Google Scholar]
- 23.Stiefel MC, Perla RJ, Zell BL. A Healthy Bottom Line: Healthy Life Expectancy as an Outcome Measure for Health Improvement Efforts. Milbank Q. 2010;88:30–53. doi: 10.1111/j.1468-0009.2010.00588.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tourlouki E, Polychronopoulos E, Zeimbekis A, Tsakountakis N, Bountziouka V, Lioliou E, et al. The ‚secrets‘ of the long livers in Mediterranean islands: the MEDIS study. Eur J Public Health. 2010;20:659–664. doi: 10.1093/eurpub/ckp192. [DOI] [PubMed] [Google Scholar]
- 25.Samoutis G, Paschalides C. When will the sun shine on Cyprus‘s National Health Service? Lancet. 2011;377:29. doi: 10.1016/S0140-6736(10)62337-9. [DOI] [PubMed] [Google Scholar]
- 26.Colpaert K, Vanbelleghem S, Danneels C, Benoit D, Steurbaut K, Van Hocke S, et al. Has information technology finally been adopted in Flemish intensive care units? BMC Med Inform Decis Mak. 2010;10: Article 62 doi: 10.1186/1472-6947-10-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Furukawa MF, Raghu TS, Shao BBM. Electronic medical records and cost efficiency in hospital medical-surgical units. Inquiry-J Health Car. 2010;47:110–123. doi: 10.5034/inquiryjrnl_47.02.110. [DOI] [PubMed] [Google Scholar]
- 28.Rosko MD, Mutter RL. Inefficiency differences between critical access hospitals and prospectively paid rural hospitals. J Health Polit Polic. 2010;35:95–126. doi: 10.1215/03616878-2009-042. [DOI] [PubMed] [Google Scholar]
- 29.Halkos GE, Tzeremes NG. A conditional nonparametric analysis for measuring the efficiency of regional public healthcare delivery: An application to Greek prefectures. Health Policy. 2001;103:73–82. doi: 10.1016/j.healthpol.2010.10.021. [DOI] [PubMed] [Google Scholar]
- 30.Afonso A, Aubyn MS. Assessing health efficiency across countries with a two-step and bootstrap analysis. Appl Econ Lett. 2011;18:1427–1430. [Google Scholar]
- 31.Jovanovic-Milenkovic M. Interest of the population in electronic communication in the health services provision: Research results. Manage. 2011;16:79–85. [Google Scholar]