

Abstract
Introduction: Palmaris longus variations may include complete agenesis, variation in the location and form of the fleshy portion, aberrancy in attachment, duplication or triplication, accessory tendinous slips, replacing elements of similar form or position.
Description of case: An anomalous palmaris longus muscle was found in the right upper extremity of a 63 year-old male cadaver. The muscle was totally fleshy without a long insertion tendon. Its origin was normal, the belly was rather broad and long, fusiform at the upper half and unipennate at the lower half of the forearm, and it was toggled into a short and thick tendon. At its insertion the tendon was split forming a second thinner tendon. The thick tendon was inserted into the flexor retinaculum and the thinner one into the palmar aponeurosis. The muscle compressed the median nerve although no related symptoms were reported on the cadaver's medical history.
Discussion: This variation is of clinical importance because it may cause carpal tunnel syndrome or difficulties in image interpretation by radiologists. In addition the palmaris longus muscle is an anatomical landmark for operations at the forearm and wrist and its tendon can be used as a graft.
Keywords: anatomical variations, muscle variations, forearm, hypertrophy
Introduction
The Palmaris Longus (PL) is one of the most variable muscles in the human body. Its variations may include complete agenesis, variation in the location and form of the fleshy portion, aberrancy in attachment, duplication or triplication, accessory tendinous slips, replacing elements of similar form or position1-3. These variations are of clinical importance because they may cause compartment syndrome of the forearm and the wrist, carpal tunnel syndrome, Guyon's syndrome or difficulties in image interpretation by radiologists. Moreover the palmaris longus muscle is an anatomical landmark for operations on the forearm and wrist and its tendon can be used as a graft4-6. The purpose of the present study is the detailed description of a variant fleshy palmaris longus muscle with reference to its clinical impact.
Case report
Our finding was revealed during routine anatomical dissection of a 63 year-old formaline embalmed, male cadaver. In the right upper limb of the cadaver the palmaris longus muscle was totally fleshy without a long insertion tendon. It originated at the medial epicondyle of the humerus along with the other flexor muscles, the flexor carpi radialis (FCR), the flexor digitorum superficialis (FDS) and the flexor carpi ulnaris (FCU) of the forearm, according to the normal anatomical pattern. The muscle belly was rather broad (length: 12.4 cm, width: 1.7 cm) following a downward and outward direction to the upper middle of the forearm, where it was toggled into a short and thick tendon (length: 107 mm, width: 5 mm). The muscle fibers continued on the radial edge of this tendon, forming an unipennate muscle (length: 10 cm, width: 1.2 cm) at the lower middle of the forearm, covering the tendons of the FDS muscle and compressing the median nerve. At its insertion the tendon was split forming a second thinner tendon (length: 9.4 cm, width: 0.3 cm). The thick tendon was inserted into the flexor retinaculum and the thinner one into the palmar aponeurosis (Figure 1).
Figure 1. The fleshy Palmaris Longus (PL) muscle, fusiform (f) at the upper half and unipennate (u-p) at the lower half of the forearm and its relationship with the Flexor Carpi Radialis (FCR). The thick tendon (arrowheads) and the thin tendon (thin arrows) of the PL can also be seen, as well as the median nerve (thick arrows).

Discussion
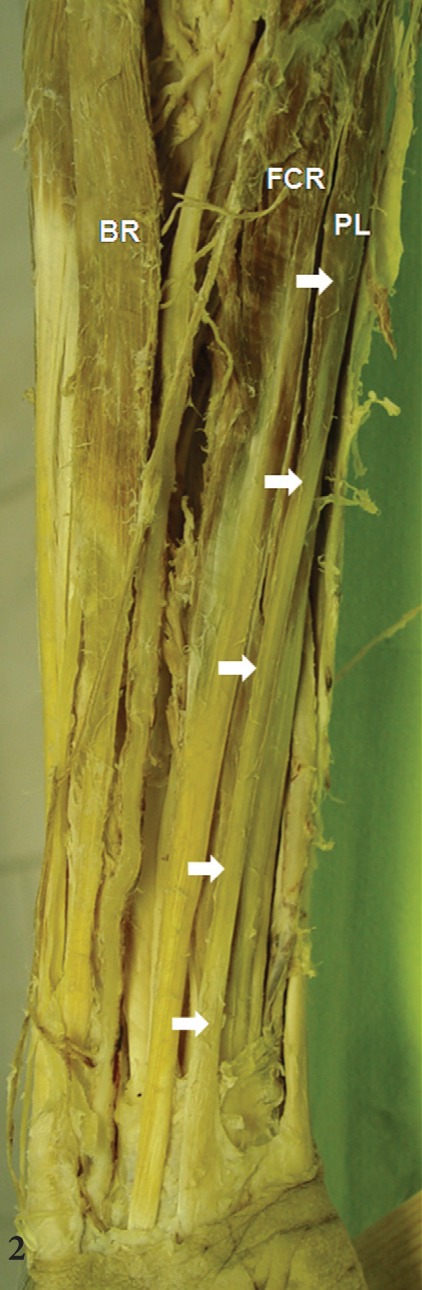
The palmaris longus muscle is a superficial flexor muscle of the forearm and arises along with the other superficial flexor muscles from the medial epicondyle of the humerus by a common tendon (Figure 2). These muscles are the pronator teres (PT), the FCR, the PL, the FDS and the FCU. Palmaris longus is a slender, fusiform muscle (muscular belly length: 95-230mm) and it is located just under the skin, the subcutaneous fat and the forearm's fascia, superficial to FDS and between FCR (lateral) and FCU (medial). It originates at the medial epicondyle, adjacent intermuscular septa and the deep fascia. It runs downwards and outwards and converges on a long tendon (length: 80-155 mm, width: 4mm) constituting the lower two thirds of the muscle and passes superficial to the flexor retinaculum. A few tendon fibres interweave with the transverse fibres of the retinaculum, but the main part of the tendon passes distally. As the tendon crosses the flexor retinaculum it broadens out to become a flat sheet which becomes incorporated into the palmar aponeurosis. The median nerve at the wrist lies partly under the palmaris longus tendon, and partly between the PL and FCR tendons7,8.
Figure 2. The normal Palmaris Longus (PL) muscle and its route in the forearm (thick arrows). Also visible are the Flexor Carpi Radialis (FCR) and the Brachioradialis (BR).
Palmaris longus is considered as a phylogenetically degenerate metacarpophalangeal joint flexor. Although it plays a role in carpal flexion, its main function appears to be as an anchor for the skin and fascia of the hand, in resisting horizontal shearing forces in a distal direction, as in holding a golf club7. It also takes part in thumb abduction9.
The palmaris longus muscle is one of the most variable muscles in the human body and it belongs in the class of retrogressive muscles. With the palmar aponeurosis the muscle represents the most superficial part of the primitive common flexor muscle of the fingers3. Among vertebrates the palmaris longus is restricted to the mammals and among primates it is found in the lower groups (urangutan) being variably absent in the higher apes (gibbon, chimpanzee and gorilla)10,11. This retrogression is considered to be due to the gradual development of prehension, achieved by diversion of muscular power for the independent motion of parts of the hand12.
An extensive research and classification of the palmaris longus muscle variations has been made by Reimann et al3. These variations involve both the muscle belly and the tendon. The most common of them is the agenesis of the muscle with an incidence of 12.8% in American whites and blacks3 and 3.4% in Japanese13, being a bit more often on the right forearm. All the remaining variations (except from agenesis) have an incidence of about 9% and are observed more frequent on the right side3.
Variations in form are the most commonly seen and constitute 50% of them. Their incidence is about 4.3%3. The muscle belly is normally short, fusiform and proximal in position and it is toggled into a long tendon7. However, all phases of muscular development are encountered from a type completely muscular from origin to insertion, to a form in which only a fibrous vestige remains. The muscle belly may be centrally placed, entirely distal or double, forming a digastric muscle. In addition the muscle belly or its tendon may be bifid or both parts may be split3.
Variations in attachment occur with an incidence of about 0.5%3. They may be present in the muscle origin or insertion but the insertion is highly variable. The tendon normally gives some fibres to the flexor retinaculum and after turning into a flat sheet is incorporated into the palmar aponeurosis7. Variable insertions include the antebrachial fascia, the fascia of the thenar eminence, the expansion of the flexor carpi ulnaris insertion over the wrist, the transverse carpal ligament, the interosseus membrane, the carpal bones, the tendons of the flexor digitorum profundus, FDS and FCR. The tendon may be bifid distally with the extra slip inserting into any one of the above structures3.
We present a unique case of a variant-in-form palmaris longus muscle on the right forearm being completely muscular from origin to insertion. It was fusiform at the upper middle and unipennate at the lower middle of the forearm. Moreover the muscle's tendon was divided at its distal part forming two different tendons with different insertions, one into the flexor retinaculum and the other into the palmar aponeurosis.
The anomalous palmaris longus muscle with muscular distal part has been associated with carpal tunnel-like symptoms because of the pressure applied on the median nerve proximal to its insertion into the carpal tunnel. This correlation is well established in cases of a reversed palmaris longus muscle which is muscular at its lower and tendinous at its upper part. Swelling in the palmar surface of the wrist, reduction of the hands muscular power, pain and numbness in the distribution of the median nerve are common symptoms4,5. Guyon's syndrome is a similar condition caused by the compression of the ulnar nerve at the wrist and the patient experiences pain or numbness in the distribution of the ulnar nerve4.
In our case the unipennate form of the palmaris longus at its lower part repulsed the median nerve. No associated symptoms were reported in the cadaver's medical history nor was there any atrophy in the muscles of the hand innervated by the median nerve. On the ulnar side of the thick tendon no muscle fibers were present so the ulnar nerve followed its normal route.
The knowledge of this variation is significant for radiologists, orthopaedic and plastic surgeons to bear in mind during differential diagnosis because the lower fleshy part of the muscle can be mistaken for a tumor or a ganglion on MRI or on clinical examination5. Forearm free flaps with palmaris longus tendon in reconstruction of total maxillectomy have been applied with success14. The palmaris longus muscle is also an anatomical landmark for hand surgeons and its tendon can be used as a graft in order to bridge tendinous defects15. When the muscle is completely fleshy and there is no tendon or the existing tendon is short (as in our case) the overhead-mentioned useful characteristics are lost.
Conflicts of interest:
The authors declare there are no conflicts of interest.
References
- 1.Natsis K, Levva S, Totlis T, Anastasopoulos N, Paraskevas G. Three-headed reversed palmaris longus muscle and its clinical significance. Ann Anat. 2007;189:97–101. doi: 10.1016/j.aanat.2006.07.008. [DOI] [PubMed] [Google Scholar]
- 2.Paraskevas G, Tzaveas A, Natsis K, Kitsoulis P, Spyridakis I. Failure of palmaris longus muscle duplication and its clinical application. Folia Morphol (Warsz) 2008;67:150–153. [PubMed] [Google Scholar]
- 3.Reimann A, Daseler E, Anson B, Beaton L. The Palmaris longus muscle and tendon. A study of 1600 extremities. Anat Rec. 1944;89:495–505. [Google Scholar]
- 4.Acikel C, Ulkur E, Karagoz H, Celikoz B. Effort-related compression of median and ulnar nerves as a result of reversed three-headed and hypertrophied palmaris longus muscle with extension of Guyon's canal. Scan J Plast Reconstr Surg Hand Surg. 2007;41:45–47. doi: 10.1080/02844310500453708. [DOI] [PubMed] [Google Scholar]
- 5.Bencteux P, Simonet J, el Ayoubi L, Renard M, Attignon I, Dacher JN, et al. Symptomatic palmaris longus muscle variation with MRI and surgical correlation: report of a single case. Surg Radiol Anat. 2001;23:273–275. doi: 10.1007/s00276-001-0273-x. [DOI] [PubMed] [Google Scholar]
- 6.Polesuk BS, Helms CA. Hypertrophied palmaris longus muscle, a pseudomass of the forearm: MR appearance--case report and review of the literature. Radiology. 1998;207:361–362. doi: 10.1148/radiology.207.2.9577481. [DOI] [PubMed] [Google Scholar]
- 7.Ellis H, Healy JC, Johnson D, Williams A. Forearm. In: Standring S. Edinburg, editor. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 39th Ed. Elsevier Churchill Livingstone, Philadelphia. 2005:873–887. [Google Scholar]
- 8.Ito MM, Aiko M, Kida MY, Ishii S, Kumaki K, Tanaka S. Length and width of the tendinous portion of the palmaris longus: a cadaver study of adult Japanese. J Hand Surg Am. 2001;26:706–710. doi: 10.1053/jhsu.2001.26026. [DOI] [PubMed] [Google Scholar]
- 9.Gangata H. The Clinical Surface Anatomy Anomalies of the Palmaris Longus Muscle in the Black African Population of Zimbabwe and a Proposed New Testing Technique. Clin Anat. 2009;22:230–235. doi: 10.1002/ca.20751. [DOI] [PubMed] [Google Scholar]
- 10.Keith A. On the Chimpanzees and their relationship to the Gorilla. Proc Zool Soc London. 1899:296–314. [Google Scholar]
- 11.Windle BCA, Parsons FG. On the myology of Edentata. Proc Zool Soc London. 1899:210–221. [Google Scholar]
- 12.Humphry GM. The muscles of vertebrates. J Anat and Physiol. 1872;6:293–376. [PMC free article] [PubMed] [Google Scholar]
- 13.Adachi B. Beitrage zur Anatomie der Japaner. Die Statistik der Muskelvarietaten Zweite Mitteilung. Zeitsch Morphol Anthropol. 1909;12:261–312. [Google Scholar]
- 14.Askar I, Oktay MF, Kilinc N. Use of radial forearm free flap with palmaris longus tendon in reconstruction of total maxillectomy with sparing of orbital contents. J Craniofacial Surg. 2003;14:220–227. doi: 10.1097/00001665-200303000-00017. [DOI] [PubMed] [Google Scholar]
- 15.Kleinert HE, Pulvertaft RG. Flexor tendon grafting in the hand. In: Jupiter JB, editor. Flynn's hand surgery. 4th ed. Williams and Wilkins, Baltimore. 1991:285. [Google Scholar]