

Abstract
Background: Congenital anomalies of the coronary arteries are rarely encountered in patients undergoing cardiac catheterization. In patients undergoing coronary angioplasty or cardiac surgery, angiographic recognition of coronary anomalies is important for the proper management of these patients.
Method: We retrospectively reviewed the records of 12,844 patients who had previously undergone coronary angiography in the catheterization laboratory of Trakya University Cardiology Department over the past 14 years. We tried to investigate the presence of a variety of coronary anomalies in these patients to determine the prevalence of various types of anomalies and their anatomic variation in a selected population of the European part of Turkey. The potential association between coronary atherosclerosis and congenital coronary anomalies was also investigated.
Results: Among these patients, 95 patients were found to have major coronary anomalies that predominantly comprised anomalous aortic origin of coronary arteries. Among the major anomalies, anomalous aortic origin of the left circumflex (LCX) artery from the right sinus of Valsalva or right coronary artery (RCA) was found to be the the most prevalent (46 out of 95 patients) outnumbering the second most common anomaly that was anomalous aortic origin of the RCA (32 out of 95 patients). In the present study, the incidence of major coronary arterial anomaly was found to be 0.74 %. However, only about one third of the patients (31 out of 95, 32.6%) with major anomaly had significant coronary atherosclerotic lesions among whom nine were found to involve the LCX artery with a posterior course.
Conclusion: The incidence of congenital coronary anomalies in a selected population of the European part of Turkey is similar to those of other populations. Congenital coronary anomalies generally present as isolated anomalies and are not associated with an increased risk of coronary atherosclerosis in this series. Cardiologists and surgeons should be familiar with these entities for the proper management of patients undergoing cardiac surgery or coronary angioplasty.
Keywords: Congenital coronary anomaly, coronary atherosclerosis, incidental finding
Introduction Congenital anomalies of the coronary arteries are rarely encountered in patients undergoing cardiac catheterization. Previous reports have particularly focused on the benign nature of a coronary anomaly suggesting this entity as an incidental finding during coronary angiography (CAG) or at autopsy1-5. In patients undergoing coronary angioplasty or cardiac surgery, angiographic recognition of coronary anomalies is important for the proper management of these patients. Accordingly, the present retrospective study was designed to angiographically determine the prevalence of various types of anomalies and their anatomic variation in a selected Turkish adult population.
Patients and methods
We retrospectively reviewed the records of 12,844 patients who had previously undergone coronary angiography for various cardiovascular conditions in the catheterization laboratory of Trakya University Cardiology Department over the past 14 years (between the dates of 1 January 1996 and 1 May 2010). Coronary angiography was performed via Judkins femoral or Sones brachial technique using a 6-inch image intensifier. We tried to investigate the presence of a variety of coronary anomalies, particularly focusing on major anomalies, in the angiographic records of patients to determine the prevalence of various types of anomalies and their anatomic variation in a selected Turkish adult population. The potential association between coronary atherosclerosis and congenital coronary anomalies was also investigated.
Results
Among the 12,844 retrospectively reviewed subjects, 95 patients [69 men (72.6%) and 26 women (27.3%)) patients were found to have major coronary anomalies predominantly comprising anomalous aortic origin of coronary arteries. Among the major anomalies, anomalous aortic origin of the LCX artery from the right sinus of Valsalva or RCA was found to be the the most prevalent (46 out of 95 patients, 48.4%) outnumbering the second most common anomaly that was anomalous aortic origin of the RCA (32 out of 95 patients, 33.6 %). Left and right coronary arteries arising from the right aortic sinus was the third most commonly encountered anomaly (6 out of 95 patients, 6.3%). Some coronary anomalies demonstrated in Figures 1-4.Figure 1, Figures 2-3, Figure 4. The types of major anomalies are demonstrated in Table 1. Table 2 demonstrates the types of minor coronary anomalies. Of the 188 subjects diagnosed as having minor coronary anomalies, the most common ones the myocardial bridge (83/188; 44.1%) and absence of the left main coronary artery (LMCA) (56/188 patients; 29.7%). Other minor anomalies were high take-off coronary artery (32/188; 17.0%), accessory RCA arising from the proximal portion of RCA (6/188; 3.2%) or RCA arising from an unusual site within the right sinus of Valsalva (3/188; 1.6%), the presence of a minor communication between LAD and PA (3/188; 1.6%), coronary anomalies as a component of a complex congenital heart disease (with tetralogy of fallot (2/188, 1.0%) interarterial communication (3/188; 1.6%). Fifteen subjects with minor anomalies were found to have a coronary stenosis of ≥ 80%, and were symptomatic (15/188; 7.9 %). In the present study, the total incidence of major coronary arterial anomaly was found to be 0.74 %. However, only about one third (31 out of 95, 32.6%) of patients with major anomaly had significant coronary atherosclerotic lesions among which nine were found to involve the LCX artery with a posterior course.
Figure 1. LMCA arise from right sinus valsalva.
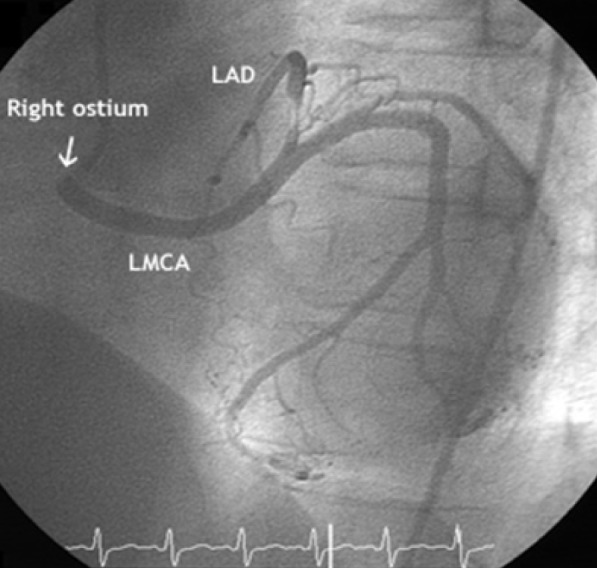
Figure 2-3. Double Cx (Accessory Cx arise from left system and second Cx arise from right ostium).
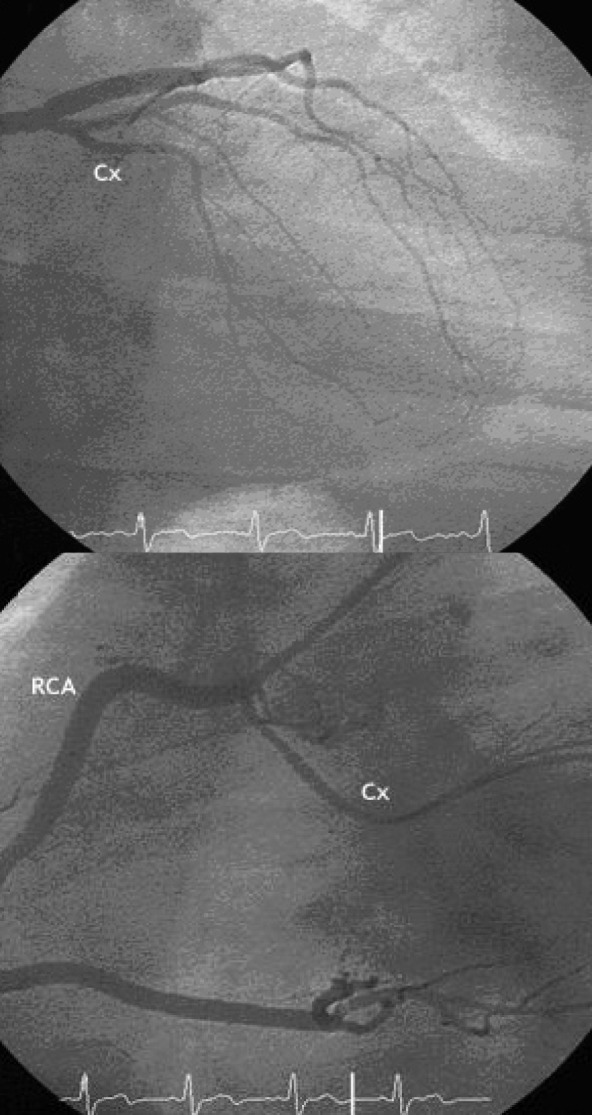
Figure 4. Fistulae between Cx and Pulmonary artey. Cx course as a fistulae.
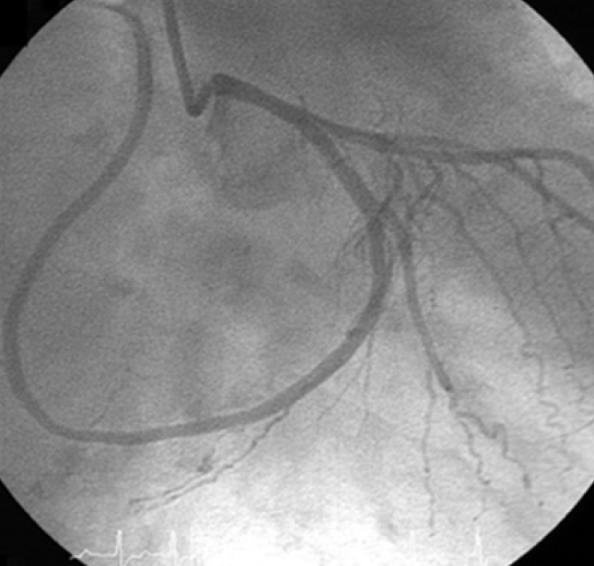
Table 1. Major coronary anomalies.
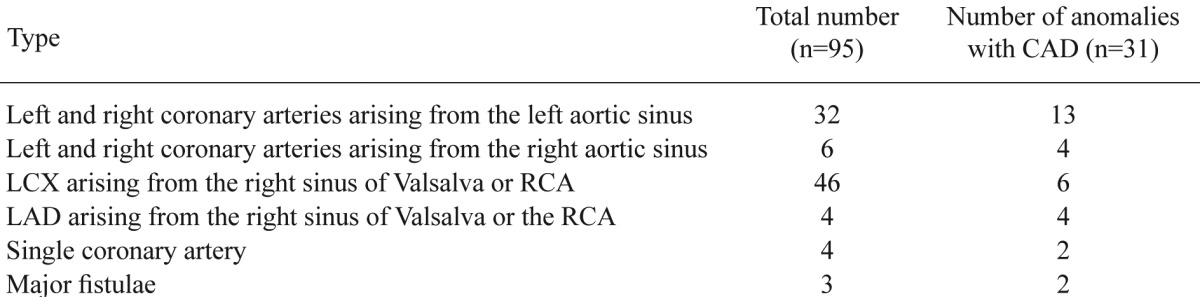
RCA: right coronary artery, LAD: left anterior descending artery, LCX: left circumflex artery, CAD: coronary artery disease
Table 2. Minor coronary anomalies.
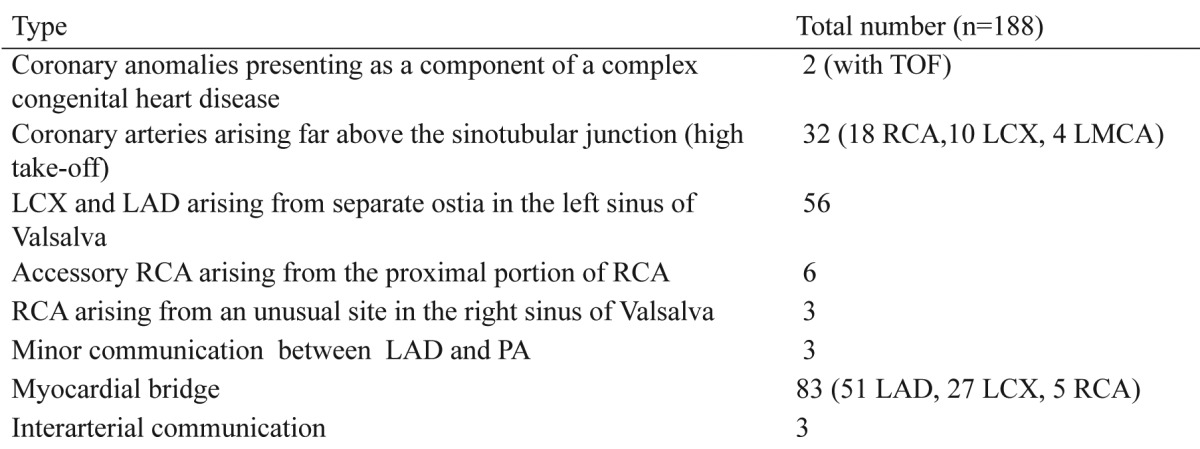
TOF: tetralogy of fallot, RCA: right coronary artery, LCX: left circumflex artery, LMCA: left main coronary artery, LAD: left anterior desendan artery, PA: pulmonary artery
Discussion
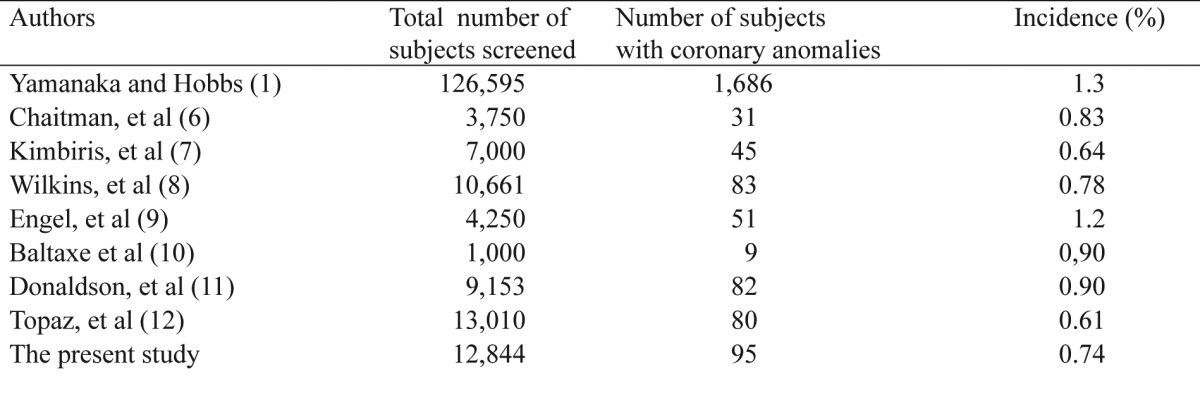
The incidence of major coronary anomaly in the present retrospective series is similar to those of some previous reports1-8. Consistent with the previous literature, anomalus origin of the LCX artery is the most common major anomaly along with the presence of an overall male gender predilection. In the literature, the largest study on coronary anomalies was reported by Yamanaka and Hobbs1. A total of 126,595 CAG were retrospectively analysed in this study concluding that 80% of the coronary anomalies were benign in nature1. The most commonly encountered minor anomaly was the presence of LAD and LCX arteries arising from separate ostia in this study1. Based on various studies, the incidence of angiographically determined coronary artery anomalies ranges from 0.61 to 1.301,6-12 (Table 3).
Table 3. Incidences of major coronary anomalies in the current literature and the present study.
According to the current literature, the majority of coronary anomalies are associated with the origin or distribution (course, structure) of a coronary artery whereas the anomalies of termination (fistulae, etc.) are relatively less frequent. Consistent with this notion, the majority of the major anomalies in the present study was associated with the origin of the coronary arteries. Coronary arteries arising from the contralateral aortic sinus or PA may be of paramount clinical importance given the potentially life threatening conditions including severe myocardial ischemia or sudden cardiac death (SCD), etc. Thorough identification of the origin and distribution of the anomalous coronary artery arising from the contralateral aortic sinus has been considered imperative as this anomaly, in the setting of an interarterial course (between aorta and PA) may be associated with ischemic symptoms13, malignant arrhythmic events and even SCD, etc, particularly during physical activity. In a similar manner, single coronary artery may also be associated with an increased risk of SCD in the setting of an interarterial course14. Besides inherent risks, coronary intervention (balloon angioplasty, etc.) in the setting of a single coronary artery may be quite challenging, and has been rarely reported15-18. Interestingly, coronary anomalies including anomalous origin of coronary arteries from the PA, major structural malformations (hypoplasia, agenesis, etc ) were encountered in none of the subjects in the present study. This might have been due to the relatively worse prognosis and premature death of these subjects before angiographic evaluation. Coronary anomalies may also present as a component of a complex congenital heart disease. LAD arising from RCA or right sinus of Valsalva is generally associated with congenital heart diseases including TOF, and has been very rarely reported as an isolated anomaly19 as in the present study. There were 2 patients with the diagnosis of TOF in the present series, however, these patients were found to have a minor connection between LAD and PA as an accompanying congenital coronary anomaly. Single coronary artery may also be associated with congenital heart disease including transposition of great arteries1. However, single coronary artery was also encountered as an isolated anomaly in the present study. It may be suggested that coronary anomalies have generally been considered as isolated anomalies and has no significant association with other complex heart diseases13. Interestingly, some previous reports suggested the presence of a strong association between coronary atherosclerosis and coronary anomalies8. Contrary to these reports, only one third of patients with coronary anomalies were found to have atherosclerosis in the present study. However, the most common anomalous coronary artery with an atherosclerotic involvement was the LCX artery with a posterior course suggesting its particular proclivity for atherogenesis. Since coronary flow patterns are well known to play a fundamental role in atherogenesis, this might have been due to a particular impairment of coronary flow kinetics (slow flow, etc.) in this anomaly. However, the exact mechanisms have yet remained to be established.
In conclusion, the incidence of congenital coronary anomalies in a selected population of the European part of Turkey is similar to those of other populations. Congenital coronary anomalies (even those well known to be as a component of complex congenital heart diseases) generally present as isolated anomalies in this series and are not associated with an increased risk of coronary atherosclerosis. Cardiologists and surgeons should be familiar with these entities for the proper management of patients undergoing cardiac surgery or coronary angioplasty.
References
- 1.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 2.Eid AH, Itani Z, Al-Tannir M, Sayegh S, Samaha A. Primary congenital anomalies of the coronary arteries and relation to atherosclerosis: an angiographic study in Lebanon. J Cardiothorac Surg. 2009;4:58. doi: 10.1186/1749-8090-4-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aydinlar A, Ciçek D, Sentürk T, Sentürk T, Gemici K, Serdar OA, Kazazoglu AR, Kumbay E, Cordan J. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study in Western Turkey. Int Heart J. 2005;46:97–103. doi: 10.1536/ihj.46.97. [DOI] [PubMed] [Google Scholar]
- 4.Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study. Int J Cardiol. 2000;74:39–46. doi: 10.1016/s0167-5273(00)00243-6. [DOI] [PubMed] [Google Scholar]
- 5.Yildiz A, Okcun B, Peker T, Arslan C, Olcay A, Bulent Vatan M. Prevalence of coronary artery anomalies in 12,457 adult patients who underwent coronary angiography. Clin Cardiol. 2010;33:E60–E64. doi: 10.1002/clc.20588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chaitman BR, Lesperance J, Saltiel J, Bourassa MG. Clinical, angiographic, and hemodynamic findings in patients with anomalous origin of the coronary arteries. Circulation. 1976;53:122–131. doi: 10.1161/01.cir.53.1.122. [DOI] [PubMed] [Google Scholar]
- 7.Kimbiris O, Iskandrian AS, Segal BC, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978;58:606–615. doi: 10.1161/01.cir.58.4.606. [DOI] [PubMed] [Google Scholar]
- 8.Wilkins CE, Betancourt B, Mathur VS, Massumi A, De Castro CM, Garcia E, et al. Coronary artery anomalies: a review of more than 10,000 patients from the clayton cardiovascular laboratories. Tex Heart Inst. J 1988;15:166–173. [PMC free article] [PubMed] [Google Scholar]
- 9.Engel HJ, Torres C, Page HL. Major variations in anatomical origin of the coronary arteries: angiographic observations in 4,250 patients without associated congenital heart disease. Cathet Cardiovasc Diagn. 1975;1:157–169. doi: 10.1002/ccd.1810010205. [DOI] [PubMed] [Google Scholar]
- 10.Baltaxe HA, Wixson D. The incidence of congenital anomalies of the coronary arteries in the adult population. Radiology. 1977;122:47–52. doi: 10.1148/122.1.47. [DOI] [PubMed] [Google Scholar]
- 11.Donaldson RM, Raphael M, Rodley-Smith R, Yacoub MH, Ross DN. Angiographic identification of primary coronary anomalies causing impaired myocardial perfusion. Cathet Cardiovasc Diagn. 1983;9:237–249. doi: 10.1002/ccd.1810090303. [DOI] [PubMed] [Google Scholar]
- 12.Topaz O, DeMarchena R, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol. 1992;34:129–138. doi: 10.1016/0167-5273(92)90148-v. [DOI] [PubMed] [Google Scholar]
- 13.Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978;58:25–34. doi: 10.1161/01.cir.58.1.25. [DOI] [PubMed] [Google Scholar]
- 14.Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39–47. doi: 10.1148/130.1.39. [DOI] [PubMed] [Google Scholar]
- 15.Chan CN, Berland J, Cribier A, Letac B. Angioplasty of the right coronary artery with origin of all three coronary arteries from a single ostium in the right sinus of Valsalva. Am Heart. J 1993;126:985–987. doi: 10.1016/0002-8703(93)90716-m. [DOI] [PubMed] [Google Scholar]
- 16.Lawton J, McGrath J, Jones JS, Dehmer GJ. Treatment of coronary artery disease in an anomalous coronary artery by placement of an intracoronary stent. Cathet Cardiovasc Diagn. 1997;41:185–188. doi: 10.1002/(sici)1097-0304(199706)41:2<185::aid-ccd17>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 17.Hsu LA, Chu PH, Ko YS, Ko YL, Chiang CW. Transluminal coronary angioplasty and stenting in a patient with single coronary artery and acute myocardial infarction. Changgeng Yi Xue Za Zhi. 1997;20:299–303. [PubMed] [Google Scholar]
- 18.Gambhir DS, Singh S, Bharadwaj S, Arora R. Rotablation and elective stenting of stenosis in the left anterior descending coronary artery arising from an anomalous single coronary artery. Indian Heart J. 2000;52:459–460. [PubMed] [Google Scholar]
- 19.Lardani H, Sheldon WC. Ectopic origin of the left anterior descending coronary artery from the right coronary sinus: report of a case simulating anterior descending obstruction. Chest. 1976;69:548–549. doi: 10.1378/chest.69.4.548. [DOI] [PubMed] [Google Scholar]