

Abstract
Rhinoplasty has grown and developed over so many years but the choice of the graft material in revision rhinoplasty and rhinoplasty for post-traumatic cases still remains debatable. In such patients, non-availability of adequate autogenous graft, multiple septal fractures and skin fibrosis are a challenge to the rhinologist. To deal with this problem authors have used diced cartilage pieces as a grafting material. Secondary rhinoplasty for correction of the nasal dorsum was done in 32 patients and evaluated. The study, highlights the distinct advantages of using diced cartilage wrapped in fascia for dorsal augmentation. Full length grafts were used in all patients and this was supported on a L-shaped cartilage fixed between the two upper lateral cartilage. Fascial tube was prepared from fascia lata and conchal, rib or septal cartilage was the source of diced cartilage (0.5–1 mm sized pieces). The L-shaped structural support was prepared from the remnant of septal cartilage if any or from the conchal or rib cartilage. Patients were followed for a period of 6 months–3 years. In 30 patients post-op course was uneventful with good reconstruction results. Step-deformity was encountered in one patient and in another patient the tube opened with extrusion of diced cartilage pieces. Both these patients were effectively managed. In conclusion, diced cartilage wrapped in fascial tube has distinct advantages like it is simpler procedure and graft material is adequate and autogenous. Grafts can be prepared as per the desired length, shape and size to fit the specific defect. These being highly malleable can be used without any tension on the already thickened and fibrosed skin and soft tissue. Complications like step deformity and extrusion rarely occur and can be easily managed. Over correction and graft visibility were not met with.
Keywords: Diced cartilage, Revision rhinoplasty, Fascia lata
Introduction
Patients report to rhinoplastic surgeons for varied complaints like visible nasal deformity or nasal blockage. Reconstruction of the dorsum is difficult and requires good pre-op planning, intra-op implementation and post-op care. Open and closed rhinoplasty along-with different grafting technique (classical en-bloc cartilage/osseous dorsal augmentation) and osteotomy techniques have been judiciously used in primary rhinoplasty but their role in secondary rhinoplasty is debatable. The rhinoplasty technique has grown all these years to come to present form where we have started using diced cartilage with or without fascia in various ways and overcome the problem of non-availability of adequate graft material. These grafts are, autogenous and fresh therefore more viable [1], sometimes even leading to fresh bone formation. They are easy to prepare and need not be freezed.
Surgical Steps
The operation is begun as an open rhinoplasty. The dorsal skin flap is dissected and raised to analyse the intra-op nasal anatomy and surgical plan is readdressed. Following points are to be considered—obtain fascia lata, obtain cartilage (and dice it), prepare fascial bag as per the measure, fill the diced cartilage in the fascial bag and finally use this for filling the defect by placing it on a L-shaped cartilaginous support between the two upper lateral cartilage. This method can effectively augment up to a height of 1–8 mm of any length and shape.
Raising the dorsal skin flap.
Obtain fascia lata: Lateral side of one of the thighs is prepared by shaving, painting and draping. About 2 inches long skin incision is given and deepened to the fascia. This is freed from the overlying and underlying soft tissue. A 2 × 2 inches (or bigger for larger defects) area of fascia lata is taken out and teased off the fibrous tissue.
Obtain cartilage: The pinna (one or both) is prepared. The outline of the conchal eminence is marked with the help of 26 gz. needles. An incision is made along this line and deepened up to the perichondrium. This is elevated and the cartilage harvested by separating it from underlying perichondrium. This is cut into small pieces (diced cartilage) with a 11 no. surgical blade (Fig. 1). These are filled in a tuberculin syringe and kept on one side.
Prepare fascial bag: The sheet of fascia is spread around the tuberculin syringe and two opposite borders stitched together and then the base sewed to prepare a bag open at one end. Now, the plunger of the syringe is withdrawn while pushing the diced cartilage filled previously in the syringe (Fig. 2). Thus a malleable pillow of diced cartilage is formed ready to be used for desired augmentation.
Placing the diced cartilage pillow: An L-shaped support is created from the septal cartilage remnant and the cartilage bag placed between the two upper lateral cartilage into the desired recipient pocket after measuring (Fig. 3) and preparing it to the desired shape and size.
Finally the skin is closed and plaster cast applied.
Fig. 1.

Dicing the cartilage into 1–2 mm pieces
Fig. 2.
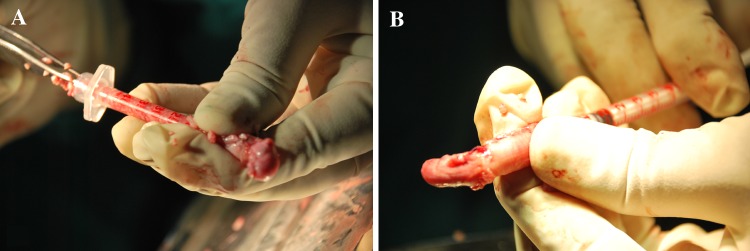
a Filling the fascial tube with diced cartilage, b Gradually withdrawing the syringe while filling it
Fig. 3.

Measuring and preparing the desired shape and size of the cartilage pillow
In this way the diced cartilage graft sits onto the desired site and possibility of palpability is also avoided by use of fascia.
Discussion
The idea of grafting diced cartilage pieces in rhinoplasty especially for revisions has stood the test of time for last 5–7 decades. Their utility in rhinoplasty has been studied and highlighted by various authors [2–4]. The use of diced cartilage chopped into 0.5–1 mm pieces was first introduced by Peer [5] and then popularised by Erol [6]. It is probably the best of fillers available to camouflage various forms of nasal defects like that at radix, half length, full length, peri-pyriform, infra-lobule or lateral nasal wall. The results in secondary rhinoplasty have dramatically improved ever-since the use of diced cartilages as it can be used in various forms—freely or along-with fascia or surgical. It survives as living tissue, is seldom resorbed and doesn’t stimulate immune response [7–9]. Uncorrected deficiencies above dorsal hump from previous osteotomies or fractures are corrected more aesthetically. Ease of insertion and malleability is a big advantage with use of diced cartilage. Moreover, over corrections and under-corrections are predictable as the graft remains mobile for almost 2 weeks. Some authors have advocated use of autogenous soft tissue like temporalis fascia [10] and dermal grafts [11] for covering dorsal irregularities.
At times the radix grafts become visible, therefore it is best to use full length grafts as we have used in all our patients. Also, in this way we can at best avoid supratip deformities. Just as in all other studies none of our patients had post-op warping or malalignment. Further extrusion or graft resorption is also avoided, the graft being autogenous.
It is to be learnt that the graft prepared inside the fascial sleeve needs to be placed in the exact desired area where the graft must stay. These need not be over-corrected as the diced cartilages do not resorb. Over corrections if at all encountered can be dealt with pituitary rongeur or if small enough covered with fascia. However, the revision cases in this study were free of any such complications.
The fascial sleeve may be prepared from temporalis fascia or the fascia lata, later was used for all the cases included in this study. This procedure is simple, quick and aesthetically superior. Cartilage can be obtained from rib cartilage or septal cartilage or the concha. All cases included in this study were grafted with conchal or rib cartilage. It is easy to harvest and large enough to prepare as big dorsal constructs as required to reconstruct full length larger defects also. Septal cartilage may not be enough to fill larger defects in revision cases or in post-traumatic cases wherein there is loss of tissue. Rib cartilage harvesting is difficult and may leave a big scar or pneumothorax or persistent pain.
Although cartilage has been used freely or under fascial cover or wrapped in fascial tube, all revision cases in this study underwent grafting with fascial tube filled with diced conchal cartilage. It is possible to combine these grafts with solid rib grafts, dorsal struts or columellar support. The author here have supported the wrapped diced cartilage on L-shaped septal support fixed between the two upper lateral cartilages. Some investigators [12] have implanted diced cartilage into prepared tissue pockets by syringing the graft material through small incisions.
Careful note was taken to prepare a tight pocket so that perfect contouring could be achieved. All revision cases had good post-op results. Two cases had post-op complication one in the form of opening of the tube spilling out of the diced cartilage pieces (cleft lip) and other with a radix graft had a step deformity. Both these cases were handled effectively and were uneventful later. Step deformities are more identifiable in thin skinned population.
To summarize, in cases with thickened skin, scars and fibrosis the pocket for placing the graft is very tight and therefore a more malleable graft is required for correction in these patients. Moreover, stretching and skin necrosis is known with use of bone grafts in such cases, which again can be avoided with diced cartilage technique. Further osseous tissue may undergo ossification and harden, it can wrap and curl over a period of few years.
To conclude, the technique of using diced cartilage is definitely advantageous in cases with multiple septal fractures (post-traumatic) or in cases when the graft material is inadequate or when there thickening of the skin (revision or trauma). Revision is possible as early as 2 months after the previous surgery, which may otherwise will have to be delayed for as long as 6 months. The postoperative results are very good as can be seen in Figs. 4 and 5.
Fig. 4.

1 Pre-op. and 2 Post-op. a front view, b basal view, c side view
Fig. 5.

1 Pre-op. and 2 Post-op. a front view, b basal view, c side view
References
- 1.Breadon GE, Kern EB, Neel B., III Autografts of uncrushed and crushed bone and cartilage: experimental observations and clinical observations. Arch Otolaryngol. 1979;105:75–80. doi: 10.1001/archotol.1979.00790140021004. [DOI] [PubMed] [Google Scholar]
- 2.Daniel RK. Diced cartilage grafts in rhinoplasty: current techniques and applications. Plast Reconstr Surg. 2008;122(6):1883–1891. doi: 10.1097/PRS.0b013e31818d2104. [DOI] [PubMed] [Google Scholar]
- 3.Daniel RK. The role of diced cartilage grafts in rhinoplasty. Aesthet Surg J. 2006;26:209–213. doi: 10.1016/j.asj.2006.01.006. [DOI] [PubMed] [Google Scholar]
- 4.Harma ST. Diced cartilage grafts in rhinoplasty. Plast Reconstr Surg. 1993;116(2):352–356. doi: 10.1097/01.prs.0000175954.55796.9e. [DOI] [PubMed] [Google Scholar]
- 5.Peer LA. Diced cartilage grafts. Arch Otolaryngol. 1943;38:156–165. doi: 10.1001/archotol.1943.00670040167008. [DOI] [Google Scholar]
- 6.Erol OO. The turkish delight: a pliable method for rhinoplasty. Plast Reconstr Surg. 2000;105:2229–2241. doi: 10.1097/00006534-200005000-00051. [DOI] [PubMed] [Google Scholar]
- 7.Peer LA. The neglected septal cartilage (with experimental observations on the growth of human cartilage grafts) Arch Otolaryngol. 1945;42:384–396. doi: 10.1001/archotol.1945.00680040504008. [DOI] [PubMed] [Google Scholar]
- 8.Parker Porter J. Grafts in rhinoplasty: alloplastic versus autogenous. Arch Otolaryngol Head Neck Surg. 2000;126:558–561. doi: 10.1001/archotol.126.4.558. [DOI] [PubMed] [Google Scholar]
- 9.Cakmak O, Ergin NT. The versatile autogenous coastal cartilage graft in septorhinoplasty. Arch Fac Plast Surg. 2002;4:172–176. doi: 10.1001/archfaci.4.3.172. [DOI] [PubMed] [Google Scholar]
- 10.Baker TM, Cortiss EH. Temporalis grafts in open secondary rhinoplasty. Plast Reconstr Surg. 1994;93:802–810. doi: 10.1097/00006534-199404000-00023. [DOI] [PubMed] [Google Scholar]
- 11.Reich J. The application of dermis grafts in deformities of the nose. Plast Reconstr Surg. 1983;71:772–782. doi: 10.1097/00006534-198306000-00005. [DOI] [PubMed] [Google Scholar]
- 12.Stoksted P, Ladefoged C. Crushed cartilage in nasal reconstruction. J Laryngol Otol. 1986;100:897–906. doi: 10.1017/S0022215100100295. [DOI] [PubMed] [Google Scholar]