

Abstract
In this study, we assessed biochemical outcomes after robot-assisted radical prostatectomy (RARP). Between July 2005 and November 2007, one hundred and seventy-six consecutive patients treated by RARP without neoadjuvant treatment were included in this study. All procedures were performed by a single surgeon and the median follow-up period was 60 months (interquartile range (IQR): 59–69). The median prostate specific antigen was 7.50 ng ml−1 (IQR: 5.14–11.45) and 39.2% of the patients were classified as intermediate risk and 15.3% were classified as high risk; on final pathological examination, 35.2% of the patients had non-organ confined disease and 37.5% and 14.2% had Gleason scores of 7 and 8–10, respectively. The biochemical recurrence (BCR)-free survival rates at 3 and 5 years were 85.6% and 81.2%, respectively. The 5-year BCR-free survival rates stratified by pathologic Gleason scores were 93.1% in Gleason scores of 6 or less, 74.5% in a Gleason score of 7, and 58.1% in Gleason scores of 8 or greater, respectively (P<0.001). When stratified by pathologic stage, the BCR-free survival rates were 89.8% in pT2 patients, 66.2% in pT3a patients, and 39.3% in pT3b patients at 5 years following RARP, respectively (P<0.001). Preoperative prostate-specific antigen (PSA), pathologic stage, postoperative Gleason score and surgical margin status were independently associated with BCR in multivariate analysis. In this study, we report biochemical outcomes after RARP with the longest follow-up periods to date in Asian men. We found that robotic surgery provided satisfactory biochemical outcomes, and that RARP is a safe and effective procedure in terms of oncologic outcomes.
Keywords: prostatectomy, prostatic neoplasm, recurrence, robotics
Introduction
Radical prostatectomy is a mainstay treatment for men with localized prostate cancer with a demonstrated survival advantage1 and surgical techniques have been refined by a number of advances in the past decades.2,3,4 Following the introduction of robot-assisted laparoscopic techniques,5 the use of robot-assisted radical prostatectomy (RARP) has rapidly increased in the United States and Europe.6,7 Robotic systems were first installed in a few Asian centers in 2004–2005, but the acceptance of RARP in Asia has been slower than Western countries for several reasons, such as cost, insurance, or public policy.8
Given the natural history of prostate cancer and the relatively recent adoption of robotic techniques, the oncologic outcomes after RARP have not been sufficiently assessed compared with open series, which have included more than 10 years of follow-up.9,10 Recently, several studies have reported the biochemical outcomes of RARPs with more than 5 years of median follow-up.11,12,13 Evaluating the oncologic outcomes of RARP has great significance in several aspects. As one of the standard treatments of prostate cancer, effective oncologic control is of paramount importance. In addition, the outcomes of prostate cancer are influenced not only by treatment modality, but also by patient characteristics. Considering the rapid and wide assimilation of robotic techniques in the treatment of prostate cancer, the oncologic outcomes after RARP may reflect the oncologic outcomes of contemporary populations.
After the initial use of RARP in Korea at Yonsei University on 15 July 2005, one thousand and thirty-six patients underwent RARP by a single surgeon (KHR) until December 2011, the largest single surgeon series in Asian men.14 While several studies have reported on the feasibility, technical aspects, or functional outcomes of RARP,14,15,16 the current body of published literature is insufficient on the oncologic outcomes after RARP in Asian men, especially with long-term follow-up. Thus, in this study, we examined the biochemical outcomes in patients who underwent RARP between 2005 and 2007. All surgeries were performed by a single surgeon and the median follow-up was 5 years.
Materials and methods
From July 2005 to December 2011, one thousand and thirty-six patients with prostate cancer underwent RARP by a single surgeon (KHR). All data was collected prospectively into an electronic database and analysed after obtaining institutional review board approval (4-2012-0706). There were 191 patients who underwent RARP between July 2005 and November 2007 and were eligible for follow-ups more than 5 years. Sixteen patients who had received neoadjuvant treatment were excluded, leaving 176 eligible men as the study cohort.
All patients underwent preoperative staging with computed tomography or magnetic resonance imaging and bone scan, which confirmed no evidence of metastatic disease. RARP was performed via a transpertioneal approach using the daVinci Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). We routinely placed six trocars and the port configuration was described in detail in our previous report.14 Excluding the initial 26 patients, standard lymph node dissection including the external iliac, obturator and infraobturator area was carried out during the study period regardless of the risk of lymph node metastasis. Prostatectomy specimens were fixed and processed using the whole mount technique with 3–5 mm transverse sections. Extraprostatic extension was defined as the extension of cancer into the periprostatic soft tissue and the presence of tumour cells at the inked margin was considered as a positive surgical margin.
After surgery, prostate-specific antigen (PSA) was assessed every three months for the first year and semi-annually thereafter. Biochemical recurrence (BCR) was defined as the detection of serum PSA greater than 0.2 ng ml−1 with a secondary confirmatory increase at least 6 weeks after surgery. Subsequent treatments such as radiotherapy or hormonal therapy were not performed in the adjuvant setting and were delayed until documented biochemical failure.
Clinicopathological variables including age, body mass index, preoperative PSA, clinical stage and biopsy Gleason score, as well as postoperative variables including postoperative Gleason score, pathologic stage, surgical margin status and the presence of lymph node invasion were assessed. The BCR-free survival rate was calculated by Kaplan–Meier analysis and compared among groups using the log-rank test. Of the 150 patients who underwent lymph node dissection, only 4 (2.6%) patients had lymph node metastases. The presence of lymph node metastases was not included in the analysis of BCR-free survival rate due to the small number of patients with lymph node metastases. The Cox proportional hazard regression model was used to estimate the impact of clinicopathological variables on BCR-free survival. PSA, pathologic stage, pathologic Gleason score and surgical margin status were incorporated in multivariate analysis and the backward elimination method was used.
The Statistical Package for Social Science for Windows, version 18.0 (SPSS, Chicago, IL, USA) was used for all statistical analyses. A P<0.05 was considered significant, and all P values were two-sided.
Results
Clinicopathological characteristics of all patients are summarized in Table 1. The median age was 63 years (interquartile range (IQR): 59–69) and median PSA was 7.50 ng ml−1 (IQR: 5.14–11.45). A total of 39.2% of the patients were deemed intermediate risk and 15.3% of the patients were deemed high risk according to D'Amico risk stratification risk criteria.17 On postoperative pathologic examination, 62 (35.2%) had non-organ confined prostate cancer and the Gleason score was 7 in 66 patients (37.5%) and 8 or greater in 25 patients (14.2%), respectively. Of 110 patients with a biopsy Gleason score of 6, upgrading of the Gleason score was observed in 31 patients (28.1%), of which 25 patients (22.7%) were upgraded to a Gleason score of 7 (22.7%) and 6 patients (5.5%) to 8–10. Positive surgical margins were found in 59 patients (33.5%). The incidence of positive surgical margins was 17.5% in pT2 and 62.9% in pT3, respectively. Of the 150 patients who underwent lymph node dissection, 4 (2.6%) patients had lymph node metastases.
Table 1. Clinical and pathological characteristics of all patients.
| No. patients (n=176) | |
|---|---|
| Median age, year (IQR) | 63 (59–69) |
| Median PSA, ng ml−1 (IQR) | 7.50 (5.14–11.45) |
| Median BMI, kg m−2 (IQR) | 24.3 (22.6–26.0) |
| Clinical stage, n (%) | |
| T1 | 149 (84.7) |
| ≥T2 | 27 (15.3) |
| Biopsy Gleason score, n (%) | |
| ≤6 | 110 (62.5) |
| 7 | 43 (24.4) |
| ≥8 | 23 (13.1) |
| Risk category, n (%) | |
| Low | 80 (45.5) |
| Intermediate | 69 (39.2) |
| High | 27 (15.3) |
| Pathologic stage, n (%) | |
| T2 | 114 (64.8) |
| T3a | 51 (29.0) |
| T3b | 11 (6.2) |
| Pathologic Gleason score, n (%) | |
| ≤6 | 85 (48.3) |
| 7 | 66 (37.5) |
| ≥8 | 25 (14.2) |
| Lymph node invasion, n (%) | 4 (2.3) |
| Positive surgical margin, n (%) | 59 (33.5) |
| Median prostate weight, g (IQR) | 31.6 (25.4–42.1) |
Abbreviations: BMI, body mass index; IQR, interquartile range; PSA, prostate-specific antigen.
At the time of analysis, the median follow-up was 60 months (IQR: 54–65) and 150 patients (85.2%) had a minimum of 3 years of follow-up. Thirty-three (18.7%) patients experienced BCR and the 3- and 5-year BCR-free survival rates were 85.6% and 81.2%, respectively in all of the patients (Figure 1). The 3- and 5-year BCR-free survival rates stratified by pathologic Gleason scores were 96.2% and 93.1% in Gleason scores of 6 or less, 82.3% and 74.5% in a Gleason score of 7, and 62.6% and 58.1% in Gleason scores of 8 or greater, respectively (P<0.001, Figure 2a). When stratified by pathologic stage, the BCR-free survival rates were 91.8% and 89.8% in pT2 patients, 79.1% and 66.2% in pT3a patients, and 58.9% and 39.3% in pT3b patients at 3 and 5 years following RARP, respectively (P<0.001, Figure 2b). The 3- and 5-year BCR-free survival rates were 91.1% and 88.7% in patients with negative surgical margins and 76.3% and 65.8% in patients with positive surgical margins, respectively (P<0.001, Figure 2c). Of four patients who had lymph node metastases, PSA did not reach undetectable levels in two patients and the other two patients experienced BCR at 9 and 11 months respectively after surgery.
Figure 1.
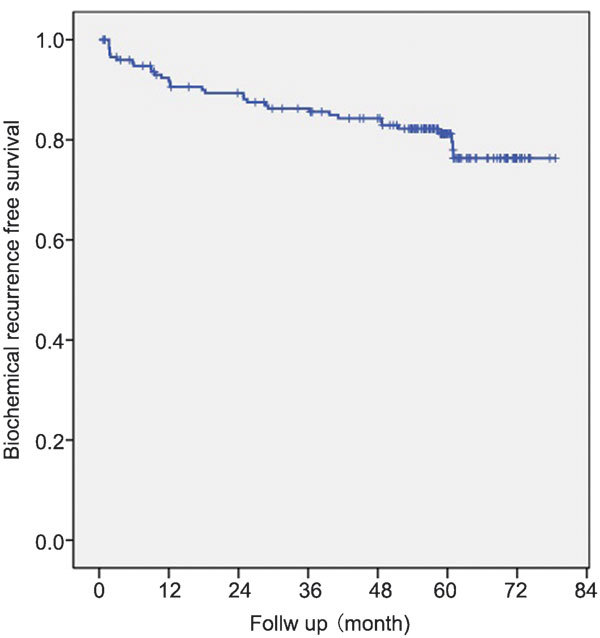
Kaplan–Meier curve of biochemical recurrence-free survival in all patients.
Figure 2.
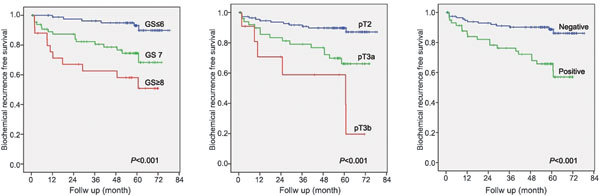
Kaplan–Meier curves of biochemical recurrence-free survival stratified by postoperative Gleason score (a), pathologic stage (b) and surgical margin status (c).
The results of univariate and multivariate Cox regression analysis were summarised in Table 2. On multivariate analysis, PSA (hazard ratio (HR): 1.02, P<0.001), pathologic stage (HR for T3a vs. T2: 1.12, P=0.629; HR for T3b vs. T2: 3.14, P=0.011), pathologic Gleason score (HR for 7 vs. ≤6: 2.13, P=0.094; 8 vs. ≤6: 3.57, P=0.008) and positive surgical margin (HR: 2.26, P=0.035) were independently associated with BCR.
Table 2. Univariate and multivariate Cox proportional hazard regression model for risk of biochemical recurrence.
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | |
| PSA | 1.03 (1.02–1.04) | <0.001 | 1.02 (1.01–1.04) | <0.001 |
| Pathologic stage | <0.001 | 0.012 | ||
| T2 | 1 | 1 | ||
| T3a | 3.34 (1.67–6.67) | 0.001 | 1.12 (0.53–2.77) | 0.629 |
| T3b | 9.38 (4.45–19.79) | <0.001 | 3.14 (1.30–7.57) | 0.011 |
| Pathologic GS | <0.001 | 0.026 | ||
| ≤6 | 1 | 1 | ||
| 7 | 3.55 (1.55–8.13) | 0.003 | 2.13 (0.87–5.15) | 0.094 |
| ≥8 | 8.24 (3.62–18.75) | <0.001 | 3.57 (1.39–9.14) | 0.008 |
| Positive surgical margin | 3.64 (1.97–6.75) | <0.001 | 2.26 (1.06–4.85) | 0.035 |
Abbreviations: CI, confidence interval; GS, Gleason score; HR, hazard ratio; PSA, prostate-specific antigen.
Discussion
Several studies have reported the oncologic outcomes after RARP.18,19,20 Even though these series reported favourable biochemical outcomes, most were based on short-term follow-ups with medians less than 3 years. Recently, Menon et al.12 published the oncologic outcomes of 1384 patients who underwent RARP with a median 5-year follow-up. Subsequently, Suardi et al.13 and Sooriakumaran et al.11 reported the biochemical outcomes after RARP in European men with a minimum follow-up of 5 years. Despite the slightly different pathologic features and inclusion criteria, the 5 years BCR-free survival rates in those studies were 86%–87%. It seems therefore that RARP can achieve oncologic outcomes comparable to an open approach.
In this series, we examined the biochemical outcomes of 176 patients after RARP with a median follow-up of 5 years. In our cohort, BCR-free survival rates were 85.6% and 81.2% at 3 and 5 years, respectively. This finding is inconsistent with recent reports of the long-term outcomes after RARP, with the BCR-free survival rates in the current series seemingly inferior to published results.11,12,13 However, our series included a higher proportion of high-grade disease and non-organ confined tumours compared with those in recent RARP series. Indeed, 14.2% of our patients had Gleason scores of 8–10 and approximately 35% had non-organ confined tumours. Although the surgeon's preferences may have contributed to the more aggressive patient characteristics in this study, recent reports from single or multi-institution studies in Korea have demonstrated similar pathologic characteristics and biochemical outcomes to our series.21,22 The median PSA was also relatively high in this study. In another multi-institutional study from Korea, patients were grouped by the year of surgery, and the median value of PSA was 10.0 ng ml−1 in one group (1995–2003) and 7.5 ng ml−1 in the other group (2004–2007), respectively.23 Despite a rather high PSA, more contemporary population cohorts presented with lower PSA levels and our results were similar with the latter group. The increased use of the PSA test may have contributed to a trend toward decreasing PSA at diagnosis and this trend is expected to continue.
Nevertheless, we believe that the higher proportion of high grade in this study is in large part due to ethnic differences in prostate cancer that have been well described in published reports. Reviewing the literature, a multi-institutional study performed in Korea showed that a significant proportion of prostate cancer exhibited poor differentiation.24 A significant proportion of high-grade disease was also noted in studies of Chinese and Japanese populations.25,26 Even in patients who underwent radiotherapy, Asian men had twice the percentage of disease with Gleason scores of 8 or greater compared with non-Asian men.27 Pathologic Gleason scores of 8–10 is one of the most influential determinants for BCR. A greater portion of patients with high-grade disease may have affected the outcomes in this study. When stratified by pathologic stage or Gleason score, the biochemical outcomes of our series seemed similar with the results of previous RARP11,12,13 or open28,29,30 series. Regarding the relatively high incidence of positive surgical margin in this study, this may be partly associated with immature surgical techniques as initial cases of RARP were included in this study. However, other radical prostatectomy series on Korean or Japanese men have also showed similar incidences of positive surgical margins, ranging from 32% to 35%.22,31,32 A significant proportion of these tumours were poorly differentiated and it may have contributed to the higher incidence of positive surgical margins. Moreover, prostate sizes of Asian men are smaller than Western men and smaller prostate sizes have been demonstrated to be independently associated with a higher incidence of positive surgical margins.33
While the incidence of prostate cancer is relatively low in Asian men, it has been increasing over the years.34,35 Currently, Korea has the largest number of robotic systems in Asia, and RARP is rapidly gaining acceptance in the urologic community in other Asian countries.8 With regards to the oncologic outcomes after RARP, there are only a few Asian studies, and most have short-term follow-up. Recently, Yip et al.36 reported 235 patients treated with RARP between 2005 and 2009 in Hong Kong, China. However, the mean follow-up period was 24 months and the biochemical outcomes were not analysed in detail. Although our group has previously reported the oncologic outcomes after RARP with more detailed pathologic variables such as perineural invasion and lymphovascular invasion, the median follow-up did not exceed 2 years. In another large series for a single surgeon in Korea, which compared the functional outcomes between robotic and open prostatectomy, the oncological outcomes were not fully analysed due to insufficient length of follow-up.15
In this study, we assessed the biochemical outcomes after RARP of a single surgeon series. In the oncological outcome assessment, sufficient follow-up is critical and we included the initial patients who underwent RARP between 2005 and 2007. The median follow-up of these patients was 5 years, which was to our knowledge the longest follow-up after RARP in an Asian population. Moreover, the current study was based on a contemporary population and all procedures were performed by a single surgeon with consistent technique. All patients were followed according to a uniform protocol and no patients received secondary treatment in an adjuvant setting. Including or excluding patients treated with adjuvant therapy whom harboured more aggressive tumour characteristics may skew the results. Our results provide unbiased evidence for the biochemical outcomes after RARP.
Our study has limitations. Although the current series has the potential advantage of being from a single surgeon series, it may not be representative of contemporary Korean or Asian populations. In addition, BCR does not necessarily accompany clinical progression or death from cancer and the median follow-up of 5 years is not long enough to assess more meaningful outcomes such as metastasis-free survival or cancer-specific survival. Finally, the effect of the learning curve was not reflected in the analysis of biochemical outcomes. This study included the learning curve of initial patients and may have overestimated the BCR. Nevertheless, the present study represents the largest series with the longest follow-up to date examining the oncological outcomes of Asian men following RARP. Although the present study is a single-arm analysis, the evidence suggests that robotic surgery provides effective oncological outcomes. Further analysis is required to determine long-term oncological outcomes such as metastases-free survival and cancer-specific mortality.
Author contributions
KHR conceived of the study. KHK and KHR participated in the design of the study. KHK and TYS performed statistical analysis and KHK drafted the manuscript under the supervision of BHC, SJH and KHR. SKL helped to draft the manuscript. All authors read and approved the final manuscript.
Competing financial interests
All authors declare that there are no competing financial interests.
Acknowledgments
This study was supported by the Research Foundation of Korea (NRF) grant funded by the Korean government (MEST) (2011-0029348) and the faculty research grant of Yonsei University College of Medicine for 2012 (6-2012-0181).
All authors declare that there are no competing financial interests.
References
- Bill-Axelson A, Holmberg L, Ruutu M, Garmo H, Stark JR, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2011;364:1708–17. doi: 10.1056/NEJMoa1011967. [DOI] [PubMed] [Google Scholar]
- Millin T. Retropubic prostatectomy. J Urol. 1948;59:267–80. doi: 10.1016/S0022-5347(17)69374-1. [DOI] [PubMed] [Google Scholar]
- Young H. The early diagnosis and radical cure of carcinoma of the prostate. Being a study of 40 cases and presentation of a radical operation which was carried out in four cases. 1905. J Urol. 2002;168:914–21. doi: 10.1016/S0022-5347(05)64542-9. [DOI] [PubMed] [Google Scholar]
- Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol. 1982;128:492–7. doi: 10.1016/s0022-5347(17)53012-8. [DOI] [PubMed] [Google Scholar]
- Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, et al. Laparoscopic radical prostatectomy with a remote controlled robot. J Urol. 2001;165:1964–6. doi: 10.1097/00005392-200106000-00027. [DOI] [PubMed] [Google Scholar]
- Lowrance WT, Elkin EB, Jacks LM, Yee DS, Jang TL, et al. Comparative effectiveness of prostate cancer surgical treatments: a population based analysis of postoperative outcomes. J Urol. 2010;183:1366–72. doi: 10.1016/j.juro.2009.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mottrie AM. The introduction of robot-assisted surgery in urologic practice: why is it so difficult. Eur Urol. 2010;57:747–9. doi: 10.1016/j.eururo.2010.01.008. [DOI] [PubMed] [Google Scholar]
- Sundram M. Asian robotic experience. Urol Oncol. 2010;28:677–81. doi: 10.1016/j.urolonc.2010.03.003. [DOI] [PubMed] [Google Scholar]
- Han M, Partin AW, Zahurak M, Piantadosi S, Epstein JI, et al. Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J Urol. 2003;169:517–23. doi: 10.1097/01.ju.0000045749.90353.c7. [DOI] [PubMed] [Google Scholar]
- Bianco FJ, Scardino PT, Eastham JA. Radical prostatectomy: long-term cancer control and recovery of sexual and urinary function (‘trifecta') Urology. 2005;66:83–94. doi: 10.1016/j.urology.2005.06.116. [DOI] [PubMed] [Google Scholar]
- Sooriakumaran P, Haendler L, Nyberg T, Gronberg H, Nilsson A, et al. Biochemical recurrence after robot-assisted radical prostatectomy in a European single-centre cohort with a minimum follow-up time of 5 years. Eur Urol. 2012;62:768–74. doi: 10.1016/j.eururo.2012.05.024. [DOI] [PubMed] [Google Scholar]
- Menon M, Bhandari M, Gupta N, Lane Z, Peabody JO, et al. Biochemical recurrence following robot-assisted radical prostatectomy: analysis of 1384 patients with a median 5-year follow-up. Eur Urol. 2010;58:838–46. doi: 10.1016/j.eururo.2010.09.010. [DOI] [PubMed] [Google Scholar]
- Suardi N, Ficarra V, Willemsen P, de Wil P, Gallina A, et al. Long-term biochemical recurrence rates after robot-assisted radical prostatectomy: analysis of a single-center series of patients with a minimum follow-up of 5 years. Urology. 2012;79:133–8. doi: 10.1016/j.urology.2011.08.045. [DOI] [PubMed] [Google Scholar]
- Jeong W, Araki M, Park SY, Lee YH, Kumon H, et al. Robot-assisted laparoscopic radical prostatectomy in the Asian population: modified port configuration and ultradissection. Int J Urol. 2010;17:297–300. doi: 10.1111/j.1442-2042.2010.02480.x. [DOI] [PubMed] [Google Scholar]
- Kim SC, Song C, Kim W, Kang T, Park J, et al. Factors determining functional outcomes after radical prostatectomy: robot-assisted versus retropubic. Eur Urol. 2011;60:413–9. doi: 10.1016/j.eururo.2011.05.011. [DOI] [PubMed] [Google Scholar]
- Chung JS, Kim WT, Ham WS, Yu HS, Chae Y, et al. Comparison of oncological results, functional outcomes, and complications for transperitoneal versus extraperitoneal robot-assisted radical prostatectomy: a single surgeon's experience. J Endourol. 2011;25:787–92. doi: 10.1089/end.2010.0222. [DOI] [PubMed] [Google Scholar]
- D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74. doi: 10.1001/jama.280.11.969. [DOI] [PubMed] [Google Scholar]
- Menon M, Shrivastava A, Kaul S, Badani K, Fumo M, et al. Vattikuti Institute prostatectomy: contemporary technique and analysis of results. Eur Urol. 2007;51:648–57. doi: 10.1016/j.eururo.2006.10.055. [DOI] [PubMed] [Google Scholar]
- Murphy DG, Kerger M, Crowe H, Peters JS, Costello AJ. Operative details and oncological and functional outcome of robotic-assisted laparoscopic radical prostatectomy: 400 cases with a minimum of 12 months follow-up. Eur Urol. 2009;55:1358–66. doi: 10.1016/j.eururo.2008.12.035. [DOI] [PubMed] [Google Scholar]
- Badani K, Kaul S, Menon M. Evolution of robotic radical prostatectomy: assessment after 2766 procedures. Cancer. 2007;110:1951–8. doi: 10.1002/cncr.23027. [DOI] [PubMed] [Google Scholar]
- Kim SC, Jeong I, Song C, Hong JH, Kim C, et al. Biochemical recurrence-free and cancer-specific survival after radical prostatectomy at a single institution. Korean J Urol. 2010;51:836–42. doi: 10.4111/kju.2010.51.12.836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Song C, Seo S, Ahn H, Byun S, Cho JS, et al. Percent tumor volume predicts biochemical recurrence after radical prostatectomy: multi-institutional data analysis. Int J Clin Oncol. 2012;17:355–60. doi: 10.1007/s10147-011-0295-2. [DOI] [PubMed] [Google Scholar]
- Byun S, Lee S, Lee E, Seo SI, Lee HM, et al. Recent changes in the clinicopathologic features of Korean men with prostate cancer: a comparison with Western populations. Yonsei Med J. 2012;53:543–9. doi: 10.3349/ymj.2012.53.3.543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Song C, Ro JY, Lee M, Hong S, Chung B, et al. Prostate cancer in Korean men exhibits poor differentiation and is adversely related to prognosis after radical prostatectomy. Urology. 2006;68:820–4. doi: 10.1016/j.urology.2006.04.029. [DOI] [PubMed] [Google Scholar]
- Li X, Zhang D, Cui X, Xu D, Hong Y, et al. Evaluating the oncologic outcomes in 152 patients undergoing extraperitoneal laparoscopic radical prostatectomy. Chin Med J. 2012;125:1529–35. [PubMed] [Google Scholar]
- Egawa S, Suyama K, Arai Y, Tsukayama C, Matsumoto K, et al. Treatment outcome by risk group after radical prostatectomy in Japanese men. Int J Urol. 2001;8:295–300. doi: 10.1046/j.1442-2042.2001.00301.x. [DOI] [PubMed] [Google Scholar]
- Man A, Pickles T, Chi KN. Asian race and impact on outcomes after radical radiotherapy for localized prostate cancer. J Urol. 2003;170:901–4. doi: 10.1097/01.ju.0000081423.37043.b4. [DOI] [PubMed] [Google Scholar]
- Hull GW, Rabbani F, Abbas F, Wheeler TM, Kattan MW, et al. Cancer control with radical prostatectomy alone in 1,000 consecutive patients. J Urol. 2002;167:528–34. doi: 10.1016/S0022-5347(01)69079-7. [DOI] [PubMed] [Google Scholar]
- Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. 2004;172:910–4. doi: 10.1097/01.ju.0000134888.22332.bb. [DOI] [PubMed] [Google Scholar]
- Dorin RP, Daneshmand S, Lassoff MA, Cai J, Skinner DG, et al. Long-term outcomes of open radical retropubic prostatectomy for clinically localized prostate cancer in the prostate-specific antigen era. Urology. 2012;79:626–31. doi: 10.1016/j.urology.2011.09.051. [DOI] [PubMed] [Google Scholar]
- Jeong CW, Jeong SJ, Hong SK, Lee SB, Ku JH, et al. Nomograms to predict the pathological stage of clinically localized prostate cancer in Korean men: comparison with western predictive tools using decision curve analysis. Int J Urol. 2012;19:846–52. doi: 10.1111/j.1442-2042.2012.03040.x. [DOI] [PubMed] [Google Scholar]
- Hashimoto K, Masumori N, Takei F, Fukuta F, Takahashi A, et al. Prognostic value of surgical margin status for biochemical recurrence following radical prostatectomy. Jpn J Clin Oncol. 2008;38:31–5. doi: 10.1093/jjco/hym135. [DOI] [PubMed] [Google Scholar]
- Marchetti PE, Shikanov S, Razmaria A, Zagaja GP, Shalhav AL. Impact of prostate weight on probability of positive surgical margins in patients with low-risk prostate cancer after robotic-assisted laparoscopic radical prostatectomy. Urology. 2011;77:677–81. doi: 10.1016/j.urology.2010.07.512. [DOI] [PubMed] [Google Scholar]
- Ferlay J, Shin H, Bray F, Forman D, Mathers C, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- Sim HG, Cheng CW. Changing demography of prostate cancer in Asia. Eur J Cancer. 2005;41:834–45. doi: 10.1016/j.ejca.2004.12.033. [DOI] [PubMed] [Google Scholar]
- Yip KH, Yee C, Ng C, Lam N, Ho K, et al. Robot-assisted radical prostatectomy in Hong Kong: a review of 235 cases. J Endourol. 2012;26:258–63. doi: 10.1089/end.2011.0303. [DOI] [PubMed] [Google Scholar]