

Abstract
Dissemination of knowledge in genetics to be applied in medicine has created a growing need for capacity building in health care workers. The CAPABILITY ARGENTINA outreach project protocol was designed as a model to introduce genetics in areas without genetic services. Our aim was for genetic health care to become part of primary care in an Argentine province lacking genetic services. The program was innovative as professionals from the referral center (Garrahan Hospital S.A.M.I.C.) traveled to remote areas to train professionals through problem-based education. A logical framework was designed for a local needs assessment. Teaching materials (Powerpoint presentations, printed syllabus, and CD) and a web page were developed. A demonstration project was carried out in the Province of Chaco, Argentina. A total of 485 health workers were trained. The number of consultations increased significantly in participating areas comparing before and after the training period. To support this increase, a complementary project was set up from a public hospital sponsored from within Argentina to build a cytogenetic laboratory in the capital of the Province of Chaco. The model was improved for reproduction in other areas in Argentina. CAPABILITY ARGENTINA is a capacity building model for training of primary care professionals in genetics that may be applied to other medical specialties. The outcomes of the programme have a direct impact on clinical practice.
Keywords: Genetics in primary care, Genetics education, CAPABILITY, Capacity building, CHACO-Argentina
Introduction
The rapid advances of genetic knowledge and technologies have created a growing need for capacity building in genetic service delivery infrastructures. This includes health workforce training in order to further the dissemination of genetics to be applied in medicine and to improve both patient care and health outcomes. Capacity building should be aimed at the development of competency in the field of genetics allowing health care workers to familiarise with new technologies and concepts and to help them integrate genetic knowledge into their practice. The development of a national capacity building network is advocated to stimulate the design of new capacity building programmes in public health to promote better health care and disease prevention in underserved areas. Presented here is the CAPABILITY ARGENTINA outreach demonstration project that was initiated in 2007 by a task team formed by the authors under the auspices of the Hospital de Pediatriá S.A.M.I.C. “Juan Pedro Garrahan” (Garrahan Hospital) Buenos Aires, and funded by the European Union (EU) CAPABILITY project. The Garrahan Hospital has a tradition of providing outreach services. Garrahan Hospital outreach communication services are geared to offering remote health care support and services in different provinces of the Argentine Republic, providing access to specialised healthcare to cover distant and difficult-to-access areas (Carniglia et al. 1999).
Presented here are the relevant steps taken during the CAPABILITY ARGENTINA outreach project between January 2007 and December 2009 in the Province of Chaco, Argentina (Fig. 1). The overall aim of the CAPABILITY ARGENTINA outreach project was for genetic health care to become part of primary care in the Argentine Province of Chaco through capacity building in genetics.
Fig. 1.

Chaco Province, Argentina marked in pink; the arrow indicates the distance between Chaco and the Garrahan Hospital in Buenos Aires
Medical genetic services are not universally available in Argentina, services being mostly urban centred, mainly in the city of Buenos Aires and its suburban surroundings. This is similar to almost all middle income developing countries. These services are heterogeneous and most provide only fragmented diagnostic services, are understaffed, usually having only one geneticist or one laboratory, generally for cytogenetics. These fragmented, understaffed services in the public domain necessitate the setting of service standards and best practice. The integration of laboratories into a collaborative network of services is fundamental and imperative.
Objectives of the Chaco outreach project
The overall objectives to be achieved by the Chaco project were:
To develop capacity in genetics applicable to primary care and to familiarise primary health care professionals with new technologies and concepts according to the nature of their socio-economic environment.
To formulate, plan, and evaluate policies and strategies addressing continuous development of knowledge in genetics and the attainment of excellence in these activities.
To be a national leader in the development and implementation of educational programmes combining the effective use of technology and application of clinical disciplines to improve quality of care and follow-up of patients in their place of origin through the training of personnel for teaching and patient care.
To establish long-term goals beyond the initial CAPABILITY ARGENTINA project funding period, evaluate the socio-economic environment in the target area, and adapt to specifications and plans of interested sectors to achieve a common vision.
To analyse preliminary results and improve and modify them in the course of the project (Continuous Process Improvement).
Design and implement a model of local delivery ( outreach demonstration project CAPABILITY ARGENTINA) taking into account the characteristics of the selected area to correlate with the recommendations of the Needs Assessment Argentina report (Barreiro 2010)
Specific objectives were:
To design a strategic framework for the organisation of a demonstration project taking into account the needs assessment report’s recommendations for Argentina and specific features of the province to be selected using the health care team as a tool to train professionals.
To design a ‘logical framework’ for planning and implementation of genetic services in underserved areas.
To present the ‘logical framework’ to national and provincial health care policy makers so as to obtain agreement to implement the CAPABILITY ARGENTINA capacity building protocol and involve them in the management process of the project.
To start the CAPABILITY ARGENTINA outreach demonstration project in the Province of Chaco so as to generate the capacity for the development of genetic health care in a province that lacked the service.
To integrate the following stakeholders in the demonstration project: members of the health care team who work in primary care, geneticists, university teachers, health institutions of different levels of complexity, parent associations, the media, political and sanitary authorities.
To progressively integrate the community in objectives and design of capacity building activities.
To start the demonstration project by a pilot study and analyse the results of the pilot study (pilot study area: Sanitary Zone V: Las Breñas, Chaco).
To make necessary modifications based on the pilot study outcome to improve implementation of the demonstration project in the remaining sanitary zones of Chaco (results management, continuous process improvement).
To continue activities in each of the remaining sanitary zones by: (a) a survey of human and institutional resources and previous knowledge; (b) capacity training in seminars (beginners training level); (c) an update of the project web page/site (continuous update training level); and (d) a programme of training of teachers (amplification training level)
To write a procedures manual.
To disseminate the results of the CAPABILITY ARGENTINA project to the national and international scientific community.
To sustain the accomplished structure in the province and to amplify the initial effect so as to continue the work once the CAPABILITY demonstration project protocol is completed.
To encourage complementary projects financed in Argentina, to reproduce the CAPABILITY ARGENTINA capacity building model in other areas in the country, and to continue the work in Chaco.
About Chaco
The Province of Chaco lies in the Gran Chaco plains, also known as the “Green Hell” for its extreme weather conditions. Frequent droughts in some areas have created deserts and torrential rains and occasional floods in other areas have given rise to rainforests.
Differences in vegetation show the unequal distribution of precipitation: An impenetrable dense dry forest ("El Impenetrable") lies in the west, with precipitations of around 600 mm per year (Fig. 2), and the “Selva Chaqueña”, a jungle with no dry season and 1,100 mm annual precipitation, is found in the east. (Fig. 3)
Fig. 2.

The “Impenetrable” Forest, an area in Chaco that is very difficult to access
Fig. 3.

“Parque National Chaco” the “Selva Chaqueña”, a jungle with no dry season and 1,100 mm precipitation
In 2008, per capita health expenditure in Chaco was around 197 USD. (Per capita health expenditure is total health expenditure for each province divided by the number of inhabitants). (Ministerio de Economica y Finanzus Públicas 2008). Besides financial barriers, geographical barriers affect access to health care as some areas in the province are very difficult to access, such as the “Impenetrable” forest which is located in Sanitary Zone VI. Infant mortality in Chaco is estimated to be 19.7‰, and the share of population in Chaco with unmet basic needs is higher than 30 % (Verner 2006).
Agricultural development is linked to the quebracho wood, and the cotton production, which currently accounts for 60 % of the national production. Other crops are soy, sorghum, and maize. Sugar cane is cultivated in the South, as well as rice and tobacco in lesser proportion. The agricultural sector has suffered from recurrent droughts over the past decade. Cattle consists of mixed races of Argentine cows with zebu, which adapt better to the high temperatures, grass shortage, and occasional flooding.
Industry contributes modestly to the economy (about 10 %) and includes textiles (produced from local cotton), oil mills, and coal production, as well as sugar, alcohol, and paper (all produced from sugar cane).
There are clearly defined ethnic communities: The native communities (about 50,000 inhabitants belong to Qom, Wichi, and Mocoví communities. They account for 7.96 % of the population of the province, while in the whole country, they represent 4.21 % of the population) and descendants of European immigrants distributed over 8,300 communities (Corach et al. 2008 and INDEC 2005).
Chaco is one of the ten provinces in Argentina lacking genetic services ( Liascovich et al. 2006). The province is located in the north-east of Argentina and has 1,053,466 inhabitants (INDEC 2010). The province is located at a distance of 1,130 km from the City of Buenos Aires, the home of the Garrahan Hospital (Fig. 1).
Rationale for choosing Chaco as project site
Chaco was chosen as the location for carrying out the CAPABILITY ARGENTINA project for the following reasons:
Absence of genetic services
Geographic and social conditions make endogamy a likely risk factor
Presence and distribution of outreach communication offices: Until the first semester of 2009, Chaco was divided into six Sanitary Areas, and each sanitary area has an outreach communication office (OCO) established in 2006. The OCO connects health care professionals of Chaco with the Garrahan Hospital. The OCO is an excellent tool to strengthen ties between Chaco and a tertiary care centre for the diffusion of educational material, the technical organisation of courses with the attendance of, and consultation and referral of patients. The strategic distribution of the OCOs allows for a better approach and coverage of the whole province. Recently, Zone VI has been subdivided into two. Today, the province has seven sanitary zones, and in each sanitary zone there are different districts (Fig. 4).
There are 400 well-staffed health care facilities in the entire province. This health care network is structured on the basis of a zoning plan which considers: accessibility and coverage based on health needs; the natural reference population, the phasing in of complex levels of services, and the provincial road network. Three of the facilities are provincial referral centres (tertiary care) belonging to Sanitary Areas I and II, and 104 are secondary care facilities. The remaining facilities are either primary care centres staffed with physicians (on duty) or nurses (active duty) or small primary care centres located in remote places, staffed by nurses and with scheduled visits by medical professionals (Table 1).
Technicians, medical doctors, and other health care professionals from Chaco are usually trained at the “Universidad del Nordeste”, in the Province of Corrientes (bordering with Chaco) The availability of locally trained professionals was considered a favourable asset for starting CAPABILITY ARGENTINA in Chaco.
Fig. 4.

Distribution of the seven sanitary zones in the Province of Chaco
Table 1.
Health care facilities in Chaco by level of service
| Facility | Number |
|---|---|
| Primary Care Centre “B“ (rural) | 264 |
| Primary Care Centre ”A” | 29 |
| General Hospital | 36 |
| Zonal Hospital | 5 |
| Interzone Hospital | 1 |
| Provincial Hospital | 2 |
| Urban Health Care Centre | 63 |
| Total | 400 |
Logical framework for capacity building in Chaco
Between 2006 and 2007, a multicentre project for the assessment of the capacity of genetic services in different areas of Argentina was being carried out by fellows from different hospitals in other provinces.(Barreiro 2010) This project was used as a basis for the start of the current programme for the construction of the Network for Genetics of the National Ministry of Health and for the design of the ‘logical framework’ CAPABILITY ARGENTINA.
Within the logical framework for the planning of capacity building processes, the following specific work strategies were applied:
Classes and educational material were designed for distance education focused on capacity building in centres where the work is intensive (hospitals/health care centres) and where hands-on experience is the starting point of learning (Burke et al. 2009; Calefato, et al. 2008; Carroll et al. 2009; Cooley 2008; Emery and Hayflick 2001; Harris et al. 2006; Trinidad et al. 2008).
A working network was set up based on hierarchical responsibilities facilitating consultations with specialists and avoiding isolated work patterns. (Many institutions like islands = paradigm of the archipelago).
Follow-up educational programmes were developed to allow for continuous education and permanent training as a tool for the improvement of primary care and fast dissemination of knowledge in this area. An amplification effect was achieved by the training of new teachers.
Participation of different social entities was sought among national and local authorities (National Ministry of Health and Ministry of Health in Chaco) as well as national and local health care workers. It is important to emphasise that the CAPABILITY ARGENTINA outreach project employed a community-oriented approach, taking into account and encouraging local, native knowledge, language diversity, and the perception of the local communities that provided cultural factors and basic knowledge for the implementation and development of the capacity building programme. The announcement in the local media of the CAPABILITY ARGENTINA outreach project in the Province of Chaco gave rise to high expectations in the local health care teams (political effect).
Possibilities for specialization and post-graduate education in Chaco depend on access to residency programmes and the availability of departments of research and development in the provincial hospitals. Post-graduate courses are usually held in Buenos Aires (at a distance of 1,130 km), nearby provinces (Corrientes and Córdoba), or in the capital of the Province of Chaco.
Taking into account these limitations, it was decided that the training courses/workshops would not be held in the capital of Chaco, Resistencia, but were started in the interior of the province (Sanitary Zone V Las Breñas), and afterwards continued in Sanitary Zone I, Sanitary Zone II, and finally in Sanitary Zone VI so as to cover different areas throughout the province. Table 2 provides an overview over the distribution of the locations where CAPABILITY training workshops were held.
Table 2.
Medical training resources in Chaco and CAPABILITY training programmes 2008–2009
| Sanitary zone number of health facilities (HF) | Main hospitals | Department of Research and Development | Residency programmes | CAPABILITY training programme done |
|---|---|---|---|---|
| Zone I (93 HF) | Hospital Pediátrico | Yes | All specialties | Yes |
| Dr. Avelino L. Castelán | ||||
| Hospital | Yes | All specialties | Yes | |
| Dr. Julio C. Perrando | ||||
| Zone II (77 HF) | Hospital 4 de Junio | Yes | Paediatrics | Yes |
| Dr. Ramón Carrillo | ||||
| Zone III (29 HF) | Hospital | No | General Medicine | No |
| Salvador Mazza | ||||
| Zone IV (41 HF) | Hospital | No | General Medicine | No |
| Félix A. Pertile | ||||
| Zone V (39 HF) | Hospital 9 de Julio | No | General Medicine | Yes |
| Rural Medicine | ||||
| Zones VI & VII (121 HF) | Hospitals Gral, Güemes (Sanitary Zone VI) | No | Rural Medicine | Yes |
CAPABILITY team Argentina
During the implementation of these first stages of the project, a working group was set up. The team was subdivided into a source or national team (Garrahan Hospital team) and a local team.
Before the CAPABILITY ARGENTINA outreach project, the Garrahan Hospital team had worked with a group of highly trained professionals in Chaco. Thus, in 2007, the team contacted these professionals working in the main paediatric hospital of the capital of the Province of Chaco (Resistencia City, in Sanitary Zone I, Avelino Castellans Hospital) and incorporated human resources from the town of Resistencia in order to set up the local team (paediatricians, a communication technician, and a management technician). This local working group has worked in Chaco in coordination with the source team. Each team worked in specific areas as well as joint capacity building areas.
When the working group was set up, the motivation was the existence of a common problem and the possibility of systematically working together in the organisation of activities. The initial asymmetry in training/information of the members of the team was compensated by the creation of a common vision through the joint construction and empowerment of the model by which the members became agents of change.
Developing capacity building tools: designing teaching resources
For the project special teaching material was designed (Bidondo and Barreiro 2008). A syllabus was prepared taking into account the different members of the health team. Level A was designed for all members of the health care team working in primary care, including: clinicians, general practitioners, gynaecologists, neonatologists, paediatricians, as well as non-medical personnel, nurses, physical therapists, clinical psychologists, health care agents, and midwives.
The syllabus was constructed to be a resource for risk factors and detection of affected status in individuals, families, and populations, and to assist the recording and registration of data to facilitate patient care (diagnosis, consultation, referral, treatment, and follow-up). The syllabus comprised explanation of genetic risk factors, examples of how to draw up a family tree, information on taking a clinical history using a systematic registration sheet with exercises and an answer key. The syllabus also contained a glossary of clinical features and dysmorphisms with anonymised photographic material to aid recognition, accompanied by a description of a physical examination.
Level B of the syllabus was aimed at all medical professionals working in primary care. It was designed to be a tool to assist in the diagnosis, counselling, and follow-up of children with common congenital defects who may present in primary care.
Information includes identification and appropriate referral of patients to a clinical geneticist and how to request genetic studies/tests that may be relevant for diagnosis. The syllabus gives a list of the criteria for referral and consultation at genetic services and indicates how to identify emergency situations in clinical genetics. A chapter on dysmorphology describes the major and minor anomalies and variations of normality and explains the clinical importance of detection. Also included are the etiopathogenic mechanisms of congenital defects and mode of inheritance. The types of genetic/studies/tests are listed together with testing criteria and sensitivity and specificity for tests. Details are given about sample taking and shipment. The syllable concludes with self-administered exercises and an answer key.
The syllabus was validated in two stages. A preliminary version was used with the participants of a pilot symposium in sanitary Zone V. During the symposium, the attendees used a printed version of the syllabus to resolve interactive activities that were administered to them as clinical cases and for teaching activities that took place in the consulting rooms. The participants resolved problems using the material, and completed a questionnaire about the syllabus design, value, and applicability. The results were very satisfactory. A second validation was performed by three external reviewers that were not related to the project.
PowerPoint presentations are used as an audiovisual support for general courses as well as orientation classes. Validation of these presentations was carried out in the Garrahan Hospital, before giving the lectures in Sanitary Zone V. Medical residents attended the classes as pupils and staff physicians were observers and assessed the teachers.
This first evaluation was very satisfactory, and only minor formatting changes were made before it was used in Chaco. A web page with password access was designed for health care professionals. The aims were to provide medium- and long-term capacity building and as an update of genetics in primary care for health care professionals anywhere in the country. This enables fast links with geneticists for consultation. The web page also offers registration for the general public on the homepage. Congress and meeting announcements and options for Continuous Education (File library of PowerPoint presentations in PDF, interviews with experts, results of teleconferences, links with databases) are listed on the site. News about CAPABILITY ARGENTINA broadcast in the media and a discussion forum for health care professionals to consult with specialists is also to be found on the website. The training programme is addressed to health care professionals and community health workers.
Brochures were designed for the general population, to facilitate the active participation of the local community, i.e. involve the community in the definition, implementation, development, and continuity of the project over time
Implementation phase
The implementation phase was divided into three stages:
Assessment of the local situation: institutional and professional resources (Survey)
Initial training: distribution of digital and printed material, workshops in Chaco for health care professionals/continuous learning: Web page;
Amplification effect: training new teachers
1. Assessing the local situation
A survey was conducted in health care facilities to assess human resources.
Another survey was sent to health care professionals in the different Sanitary Zones, to register:
Level of education
Place of education and year of graduation
Whether there was any training in genetics at their place of education
Current job title, time in area, and age range of patients
Reasons for most frequent consults (infectious disease/multifactorial disease)
If any of the consults had a genetic component
Is there a mechanism in the institution for referral or consultation for clinical cases which require further specialist input?
Which is the preferred way to receive the educational material (printed, CD-DVD, website, other)
The survey showed that in 2007/2008 all health care facilities in the Sanitary Zone V: Las Breñas, where the CAPABILITY pilot demonstration project started and where the training programmes were to be developed, completely lacked internet access. Figure 5 compares the availability of communication means in the area of the provincial capital (Sanatory Zone I) and in Las Breñas. Web page access was limited to the home of only a few professionals in Las Breñas, and only 47 % of the local health facilities had a computer, whereas in Zone I, more than 80 % of the health care facilities had a computer, and 53 % had access to the internet. As a consequence, education materials (syllabus) were printed for each CAPABILITY training participant who also received a CD. This implied higher costs.
Fig. 5.

Comparison of available means of communication in two different sanitary zones in Chaco
2. Initial training
The initial training programme was aimed at health care personnel working in hospitals, first-aid centres, peripheral health care centres, including clinicians, general practitioners, neonatologists, paediatricians, obstetricians, nurses, midwives, and clinical psychologists. The objective of the initial training programme was to incorporate basic concepts of medical genetics and to give the participants tools to implement this knowledge in their own daily practice (perinatology, paediatrics, adult medicine). The participants were taught to screen for and record genetic risk factors and to identify patients that required referral to a specialist in genetics. Secondary aims were to encourage interdisciplinary work and cooperation among different members of the health care team to improve the care for individuals with genetic problems, to help other members of the team in the diagnosis, management, counselling, and follow-up of common congenital defects, and to set up communication links to facilitate ongoing updates (continuous education).
Teaching classes were divided into two parts, initially addressing knowledge in genetics with interactive time for teacher participant exchanges. Classes on basic knowledge in genetics were given to all participants followed by classes with a specific orientation relevant to professionals’ sphere of interest and expertise, but open to all participants.
Clinical cases using PowerPoint presentation formed the second part of the session with time for discussion. Based on these cases, exercises were given that could be solved using the syllabus.
The Teaching Consult: Participants were divided into groups, and under teacher direction, patients were seen guided by principles taught in the course: i.e. determining risk factors, how to draw a family tree, how to examine the patient, and how to describe the features and dysmorphisms, etc. Based on the strategy of problem-based teaching, local cases were presented and resolved step by step using the knowledge acquired in the classes and checking the syllabus. The pupils were also trained in the use of the web page.
At the end of the course, participants were presented with a clinical case to resolve according to different assignments and to send to our institution for evaluation through the web page or through the outreach communication office.
3. Amplification effect: training new teachers
A training course for teachers was designed with support from the Garrahan Hospital and the government for further amplification of the model once the financial support of the CAPABILITY ARGENTINA project had ended. The profile of the teachers was based on the human resources available in the region and their possible integration in planned projects. The search for teachers was focused on community workers from local indigenous communities who look for missed opportunities in prevention and paediatricians from the main hospitals of the province involved in resident training programmes, assessment, and referral of patients according to the level of complexity. The teachers were divided into the following two groups depending on their role in the work of amplification: Firstly, those undertaking management work for the planning, organization, and coordination among the different sectors and the tutoring of other teachers. Secondly, those providing innovation, research, the implementation of strategies for the workshops, supervision of the learning process, and strengthening of educational bodies.
Internal and external collaboration
To sustain the benefits of the project in time, internal and external interactions took place that enriched the project during its implementation stage. The CAPABILITY Consortium (including all international partners of the CAPABILITY project) laid the basis for the systematisation and administration of the project. During the workshops of the CAPABILITY Consortium, it became possible to bilaterally share the results and implement new ideas in the demonstration projects of the different partners.
We began to involve the community in the aims and activities of the CAPABILITY Argentina using ideas from the CAPABILITY partners:
The partner representing parent and patient organization (Genetic Alliance UK, formerly Genetic Interest Group) shared brochures and other materials for the community;
The partner from Egypt shared material for the training of community leaders;
The partner from South Africa taught us how to set up laboratories with faster technology at a lower cost for the screening of chromosomal anomalies in communities with a large low-income population.
Bilateral interactions with the health care professionals in the province of Chaco allowed us to adapt the logical framework to the characteristics of the area. The Garrahan Hospital provided the institutional framework and the expert health care team for the design and implementation of the model. These interactions made it possible to sustain the project and meet the objectives planned for 2007–2009.
Evaluation processes during the project and CAPABILITY ARGENTINA results
Evaluation processes during the project
A continuous evaluation process (SWOT analysis) was embedded in the CAPABILITY ARGENTINA demonstration project protocol. Different strengths, weaknesses, opportunities, and threats were identified during the project (Table 3). When possible, we tried to counter identified weaknesses and threats in order to meet the project’s objectives.
Table 3.
S.W.O.T. matrix analysis: Results Management (continuous process improvement)
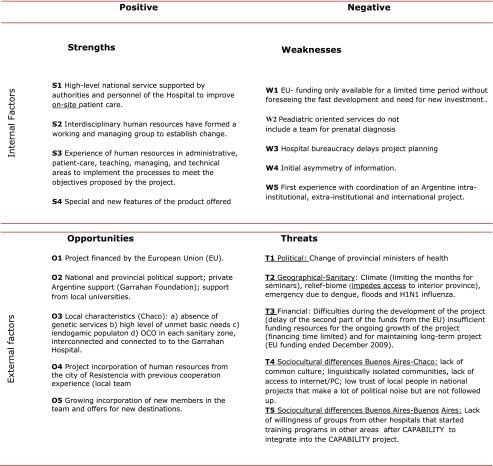
The strengths of the CAPABILITY ARGENTINA project were the availability of a tertiary care hospital with highly trained personnel and support from the authorities to improve on-site patient care. Both a managing group and an interdisciplinary team were developed to work on the project. Thus, experienced human resources in administration, patient care, teaching, management, and technical areas were available to implement the processes and meet the objectives proposed by the project. New areas of the project were developed offering ongoing training for the health care workers in Chaco.
EU financing of the project resulted in national and provincial political support. Further support was found in the private sector from the Garrahan Foundation and local universities.
Prior to the CAPABILITY ARGENTINA project, the system of OCOs had been implemented in each sanitary zone of Chaco and were interconnected and connected to our institution. From the outset, we were able to work with a local team with previous cooperation experience.
Lack of access to an internet connection and/or PC has been a limiting factor in the financial distribution and the allocation of resources for the development of the CAPABILITY project. Study materials were printed for all the pupils of each sanitary zone, and they also received a CD. It was decided to use financial resources prioritising printed material with high-quality images and contents to be applied in daily practice over digital material.
In a country where many areas lack genetic services and with high levels of unmet basic service needs, there are great opportunities for implementing the CAPABILITY ARGENTINA approach in other areas. However, difficulties were encountered because of the limited funding of the project that could not anticipate the fast development of the project and the need for new investment.
Additionally, because of the paediatric orientation of the core hospital (Garrahan Hospital) this did not include expertise in prenatal diagnosis. The bureaucracy of the public hospital delayed project planning. There was an initial asymmetry of information.
Inexperience with coordination of an Argentine intra-institutional, extra-institutional, and international project was another factor that hindered smooth operation of the project. Other obstacles were met in political, geographical, health-related, financial, social, and cultural areas.
In the political area, the most severe problem encountered was the change of Provincial Health Ministers and the lack of continuation of their policies. Geographical and health-related obstacles were the climate, which limited the months that were available for seminars as access to interior province is especially difficult during the summer months, and health emergencies due to dengue fever, floods, and H1N1 influenza.
In order to continue and expand the project in the long term, new sponsors had to be found after funding by the EU ended in December 2009. Finally, socio-cultural differences between the city of Buenos Aires and Chaco played an important part. Although part of the same country, the areas are diverse and lack common culture. Within the Province of Chaco, there are linguistically isolated communities without access to internet/PC. In the province, local people are sceptical about national projects that create political noise but are not followed up. People from the provinces traditionally distrust policy makers from the capital.
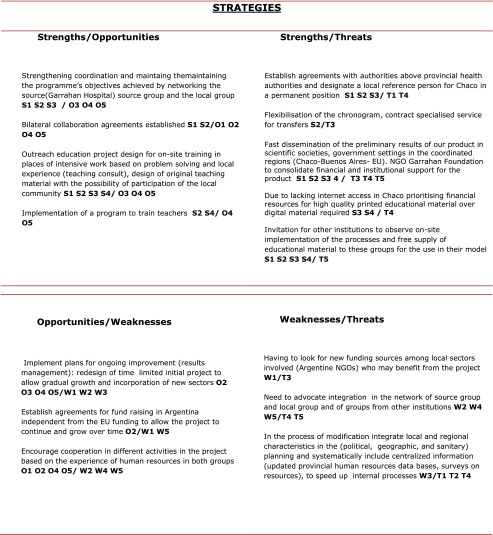
In Buenos Aires, groups from other hospitals independently started training programs in different areas but were unwilling to integrate in our project. One of the strategies used to meet the proposed objectives was to strengthen the coordination and maintain the aims achieved through the integration of the source group and the local group through a network establishing agreements of bilateral collaboration.
A model of outreach education was designed for on-site training in problem solving and local experience (teaching consult) in places where people work extremely hard with relatively few resources and little time to spare. Original teaching material was designed focussing on dysmorphisms and genetic diseases common to the Argentine population to increase the participation of the local community.
Another teaching programme was designed to train teachers who could further educate local teachers and community health workers. Other strategies were to implement plans for ongoing improvement (results management). The initial limited project with predetermined funding deadline was redesigned to allow progressive growth and incorporation of new sectors.
New agreements were made with different stakeholders to allow fund raising in Argentina independently from the funding by the EU. We specially looked for local sectors involved (Argentine NGOs) that would benefit from the project.
Cooperation was encouraged in different activities within the project based on the experience of human resources in both groups. Attempts were made to integrate groups from other institutions in the network.
In the process of implementation of the model, we tried to integrate local and regional characteristics (political, geographic, and health-related) in the planning and systematically include centralising information (updated provincial human resources databases, surveys on resources, etc.), to accelerate carrying out internal processes. In order to anticipate problems due to political instability and change of political players, agreements were made with authorities on a higher level than provincial health authorities, and a local reference person for Chaco was designated in a permanent position.
The chronogram was made more flexible to be able to better adapt to needs and times of the local team. Fast dissemination of the preliminary results of our project in scientific societies, government settings in the coordinated regions (Chaco-Buenos Aires-EU), and the NGO Garrahan Foundation was organised to consolidate financial and institutional support for the project. Other institutions were invited to observe on-site implementation of the processes, and free educational material was supplied to these groups for the use in their own model.
CAPABILITY ARGENTINA results
Training took place in five sanitary zones (I, II, III, V, and VI) covering around 836,163 inhabitants (79 % of the population of the province total 1,053,466 inhabitants, INDEC 2010); two zones did not enter the programme. A total of 485 health care workers have been trained in Chaco up to 2010 (51 in Sanitary Zone V; 179 in Sanitary Zone I; 81 in Sanitary Zone II; and 102 in Sanitary Zone VI and 72 in Sanitary zone III; Fig. 6).
Fig. 6.

Participants in the CAPABILITY training workshops in each sanitary zone
In 2008 and 2009, the total number of consultations in the four sanitary zones that participated at that time in the programme was 268. The consultation rate increased significantly (3.5 times) in those areas comparing before and after the training period, and, notably, all patients consulted had a congenital or genetic disorder. The diagnoses made in these patients did not require referral to a tertiary centre; only the clinical chart, pictures, and blood samples needed to be sent. As a consequence, the need for laboratory examinations, especially cytogenetic tests, increased.
The most difficult region to access, “El Impenetrable”, was included in the study, and this led to a dual result: capacity building in genetics was possible in this extremely poor area and capacity building in management provided a training model (on-site dissemination) for future change. At the final Chaco Capability Workshop, members of the Ministry of Health, authorities of the Garrahan Hospital, and teams from other institutions were invited for an on-site demonstration of how the project was managed and the participants were trained.
At the Garrahan Hospital, a complementary project was approved in 2008 with financial support from within Argentina to build a cytogenetic laboratory in the capital of the Province of Chaco, for G banding analysis in peripheral blood, chorionic villus sampling, high-resolution cytogenetic studies in peripheral blood, and diepoxybutane analysis in peripheral blood. Training of the technicians for this laboratory was also sponsored.
By June 2008, two projects had been started in the Province of Chaco: CAPACITY BUILDING of health care workers (CAPABILITY ARGENTINA funded by the EU) and NETWORK PROTOCOL OF CYTOGENETIC LABORATORIES to build a cytogenetic laboratory in Chaco (Funded by S.A.M.I.C. Argentina; Fig. 7). Both projects have become a platform for the initiation of genetic health care in Chaco with the aim to refer only those patients and samples that cannot be resolved locally to the specialised referral centre in Buenos Aires (Hospital Garrahan) and to set up similar laboratories in two other provinces in Argentina.
Fig. 7.

Network of cytogenetic laboratories, location of labs in different provinces of Argentina
While this teaching and training was being undertaken, engagement of the community with the project and with children with congenital and genetic disorders was assisted by the media (newspapers, TV, radio, internet), plus open talks for the community and workshops for parents with children with congenital and genetic disorders.
During 2010 and beyond, we continued training in the remaining three sanitary zones in Chaco and supporting the development of local clinical and laboratory genetic services in Chaco. Other activities planned are: (a) quality control of genetic testing and (b) progressive optimisation of the laboratory network.
Sustaining CAPABILITY ARGENTINA
The CAPABILITY ARGENTINA project was not closed, but open to interaction with complementary projects. These interactions assured continuity of the project when the financial support by the EU had ended.
Installation of OCOs in Chaco in 2006 facilitated the interconnection of sanitary zones and the source institution for the initial planning and carrying out of the project. Currently, they assure the continuity of interaction among the zones where training has taken place thus strengthening the local network.
As a consequence of the results of the CAPABILITY ARGENTINA outreach project (increase of consultations through the OCOs) priority was given to Chaco to improve the communication team. The National Ministry of Health decided to implement a programme based on the CAPABILITY ARGENTINA project in Chaco in the other provinces in northeast Argentina.
The Garrahan Foundation was asked to sponsor the necessary improvement of the quality of the syllabus. It is currently being used by the Ministry of Health. Additionally, the Argentine Society of Paediatrics has distributed the syllabus among 8,000 paediatricians within the framework of the PRONAP, a continuous training course for paediatricians.
The training project in Chaco has exponentially increased the number of consultations and samples being analysed in the laboratory overwhelming the laboratory capacity and creating the need for the installation of additional laboratories in Chaco and other provinces of the country.
The Garrahan Foundation has proposed to continue sponsoring the training model for genetics in the provinces as well as the training of personnel for the new laboratories within the network of cytogenetic laboratories.
Shipment of samples for analyses that cannot be performed in the new laboratories has improved. In the new laboratories standard operating procedures are being supervised.
The current situation in Chaco
In the main hospital (tertiary hospital), a department of genetics with outpatient offices and a cytogenetic laboratory were created.
At the neonatology department of this hospital, a registry of congenital malformations was set up participating in the national registry (RENAC).
A comprehensive service for the care of paediatric patients with congenital diseases has been set up in Day Hospital of the Paediatric Hospital Castelán. This hospital has become the referral centre in the province receiving more complex cases from the main hospitals in the sanitary zones, where cases are referred from smaller hospitals and primary care centres throughout the area, thus creating a local network of genetics. Currently, only rare cases are consulted or examinations are performed at the Garrahan Hospital in Buenos Aires.
Biochemists and pediatricians are being trained in cytogenetics and clinical genetics at the Garrahan Hospital for further capacity building in the genetic services that have been established.
Monthly teleconferences take place for patient consultation and continuous education.
Continuous training seminars are held for the local health care workers.
In conclusion
The process of planning and carrying out the CAPABILITY ARGENTINA outreach project and the transference of technology and knowledge (for primary care in genetics in the Province of Chaco) worked as a CYCLE (Fig. 8).
Fig. 8.

CAPABILITY ARGENTINA Cycle
To sustain the cycle, positive feedback from new results and continuity in time are necessary. To the local cycle in Chaco, the proposal of replication–amplification of the model was gradually added. Replication is the establishment of the model in other provinces, and amplification is feedback of the model in Chaco both in the training areas and in the remaining zones.
The results of CAPABILITY ARGENTINA suggest that replication and amplification of the capacity building should be carried out by local human resources as the development of the model requires many hours of dedication by highly educated and expert personnel as well as funding for travel and accommodation of personnel due to the distance between the source institution (Garrahan Hospital) and the local area. This last point together with the results of the project identifies the following needs:
To work in a network with multiple and interconnected centres with different hierarchies.
To work together with complementary projects.
To design a procedures manual to use as a general guide for the replication of the model in other areas in the country.
As of today, capacity building for genetics in primary care is continuing in Argentina. Four provinces are in the process of entering the programme, and we have started in Greater Buenos Aires a distance learning modality. A second syllabus that complements the first syllabus developed for CAPABILITY ARGENTINA has been written by authors from different institutions in Argentina. It addresses the care for adult patients and prenatal diagnosis. In spite of the time passed since the initial EU funding ended, we still call the ongoing capacity building programme CAPABILITY.
Acknowledgments
We would like to acknowledge the contributions of the following groups and individuals to collaborate in the development of the project:
At national level:
• Participants of Chaco, the authorities, head on the Garrahan Hospital, the Garrahan Foundation.
At international level:
• The participants of the CAPABILITY Consortium.
This project was part of the CAPABILITY Special Support Action funded by the EC 6th Framework Programme, contract number: LSSG-CT-2006-037275.
Footnotes
This article is part of the special issue "Capability/GenTEE"
References
- Barreiro C (2010) Needs Assessment CAPABILITY Argentina. Report to the Capability Project. Available at: http://www.capabilitynet.eu. Accessed 17 Jun 2013
- Bidondo MP, Barreiro C (2008) CAPABILITY Argentina Genética para la Práctica en Atención Primaria. Available at: http://www.garrahan.edu.ar/campus/file.php/37/documentos_varios/Genetica_para_la_Practica_en_Atencion_Primaria.pdf. Accessed 18 Jun 2013
- Burke S, Martyn M, Stone A, Bennett C, Thomas H, Farndon P. Developing a curriculum statement based on clinical practice: genetics in primary care. Br J Gen Pract. 2009;559:99–103. doi: 10.3399/bjgp09X395094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calefato JM, Nippert I, Harris HJ, Kristoffersson U, Schmidtke J, Ten Kate LP, Anionwu E, Benjamin C, Challen K, Plass AM, Harris R, Julian-Reynier C. Assessing educational priorities in genetics for general practitioners and specialists in five countries: factor structure of the Genetic-Educational Priorities (Gen-EP) scale. Genet Med. 2008;2:99–106. doi: 10.1097/GIM.0b013e3181614271. [DOI] [PubMed] [Google Scholar]
- Carniglia L, D’Onofrio MS, Elmeaudy P, González J, Torolla J, Castelli M (1999) Oficina de Comunicación a Distancia. Revista Medicina Infantil. Revista del Hospital de Pediatría Garrahan, Vol.VI Nro.2 Número especial: Pediatría ambulatoria 92–95. Buenos Aires
- Carroll JC, Rideout AL, Wilson BJ, Allanson JM, Blaine SM, Esplen MJ, Farrell SA, Graham GE, MacKenzie J, Meschino W, Miller F, Prakash P, Shuman C, Summers A, Taylor S. Genetic education for primary care providers: improving attitudes, knowledge, and confidence. Can Fam Physician. 2009;12:e92–e99. [PMC free article] [PubMed] [Google Scholar]
- Cooley C. Communicating genetics within primary care practice. InnovAiT. 2008;8:575–578. [Google Scholar]
- Corach D, Sala A and Marino M. (2008) Impacto de las contribuciones geneticas de los diversos-grupos etnicos en la póblacion actual del pais. cited in Barreiro C et.al(2010) al.: The CHACO Outreach Demonstration Project. Report to the Capability Project. Available at: http://www.capabilitynet.eu. Accessed 17 Jun 2013
- Emery J, Hayflick S. The challenge of integrating genetic medicine into primary care. BMJ. 2001;322(7293):1027–1030. doi: 10.1136/bmj.322.7293.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris R, Challen K, Benjamin C, Harris H. Genetic education for non-geneticist health professionals. Community Genet. 2006;9(4):224–226. doi: 10.1159/000094469. [DOI] [PubMed] [Google Scholar]
- INDEC 2005 Enquesta complementaria de pueblos indigenas (ECPI), 2004–2005 (Complementaria del Censo 2001)Primeros resultados provisionales Provincia de Chaco. Available at: http://www.mapasderecursos.org.ar/archivos_biblioteca/1246987927_Encuesta_Pueblos_Indigenas_(Chaco).pdf Accessed 16 Jun 2013
- INDEC 2010 Censo 2010 Argentina Resultados provisionales Provincia de Chaco. Available at http://www.censo2010.indec.gov.ar/preliminares/cuadro_chaco.asp. Accessed 18 Jun 2013
- Liascovich R, Rozental S, Barbero P, Alba L, Ortiz Z (2006) A census of medical genetics services in Argentina Rev Panam Salud Publica 19 (2) [DOI] [PubMed]
- Ministry de Economia y Finanzus Públicas (2008) Per capita health expenditure in Chaco, Available in Spanish from the corresponding author
- Trinidad SB, Fryer-Edwards K, Crest A, Kyler P, Lloyd-Puryear MA, Burke W. Educational needs in genetic medicine: primary care perspectives. Community Genet. 2008;11(3):160–165. doi: 10.1159/000113878. [DOI] [PubMed] [Google Scholar]
- Verner D (2006) Rural Poor in Rich Rural Areas Poverty in Rural Argentina World Bank Policy Research Working Paper 4096,Available at http://elibrary.worldbank.org/deliver/4096.pdf?itemId=/content/workingpaper/10.1596/1813-9450-4096&mimeType=pdf Accessed 17 Jun 2013