

Abstract
A case report is presented of a class III malocclusion with a class III skeletal pattern and maxillary retrusion. Patient, a 10-year-old boy was treated with an orthopedic face mask in conjunction with rapid maxillary expansion and standard pre-adjusted edgewise appliance. Treatment was completed after 3 years and proved to be stable following the active treatment.
KEY WORDS: Class III malocclusion, face mask, rapid maxillary expansion
Treatment of class III malocclusion in growing subjects is a challenging part of contemporary orthodontic practice. Many treatment approaches can be found in the literature regarding orthopedic and orthodontic treatment in class III malocclusion, including intraoral and extraoral appliances such as a facial mask (FM),[1] functional regulator-3 appliance of Frankel[2] removable mandibular retractor,[3] chincup,[4] splints, class III elastics and chincup[5] and mandibular cervical headgear.[6,7]
Many of the class III malocclusions are the result of mandibular prognathism; however, some class III malocclusions are the result of a deficient maxilla and the treatment plan of choice would be to protract the maxilla downward and forward.[6,8,9]
Successful orthopedic correction through growth modification has increased the nonsurgical correction of the growing class III patient. In addition, maxillary expansion is frequently needed in the treatment of class III malocclusions to increase the transverse width of the maxilla.
According to McNamara[10] and Turley,[11] rapid maxillary expansion (RME) may enhance the protraction effect of the face mask by disrupting the maxillary suture system and it is widely accepted among the orthodontic community that the mid-face deficient class III patients should be treated before 7-8 years of age.[12]
RME and FM therapy is the most common orthopedic treatment protocol for class III malocclusion.[13] The dentoskeletal changes induced by therapy consist of a combined effect of the protocol on both maxillary and mandibular components. Optimal timing for the orthopedic approach to class III malocclusion is related to early treatment, at either a prepubertal or a pubertal phase of development.[14]
Features of class III malocclusion are:
Class III molar relationship
Edge to edge incisor relationship or anterior cross bite
Upper arch is narrow and short while lower arch is broad. Thus, posterior cross bites are a common feature of class III malocclusion
Pseudo class III malocclusion is characterized by the presence of occlusal prematurities resulting in a habitual forward positioning of the mandible. These patients may exhibit a forward path of closure.
Sketelal features of class III malocclusion:
A short or retrognathic maxilla
A long or prognathic mandible
A combination of the above.
Etiology of class III malocclusion:
Class III has strong hereditary components
Anteriorly positioned tongue
Abnormal incisal guidance (pseudo class III).
Indications and contraindications of early class III treatment.[15]
The goals of early interceptive treatment may be:
Preventing progressive, irreversible, soft-tissue or bony changes
Improving occlusal function
Improving skeletal discrepancies
Simplifying phase II comprehensive treatment and minimizing the need for orthognathic surgery
Providing more pleasing facial esthetics; thus, improving the psychosocial development of a child.
Case Report
A 10-year-old boy came with a complaint of anterior cross bite to our department. The patient had no relevant past dental or medical history and no habits. On extra-oral examination [Figure 1], patient had a dolico-cephalic head shape, lepto-prosobic facial form, concave profile, anterior divergence and acute nasolabial angle. All functional examination was normal.
Figure 1.

Pre-treatment extraoral photographs
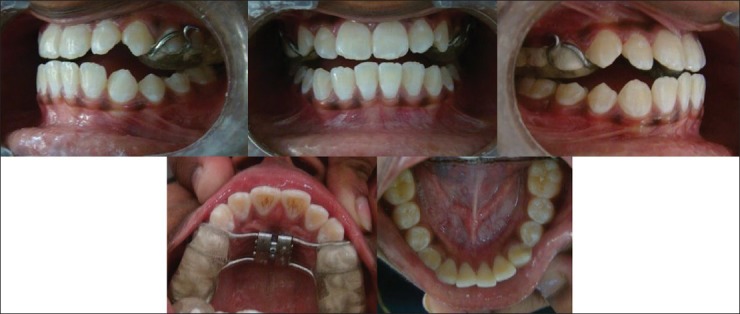
On intraoral examination [Figure 2], all soft-tissues and hard tissues were normal. Maxillary arch was constricted while mandibular arch was broad. Molar, canine and incisor relationship were class III on the both right and left side and there was a reverse overjet of 2 mm and overbite of 5 mm and anterior cross bite. The patient had class III skeletal base with retrognathic maxilla and prognathic mandible having average growth pattern with labially tipped mandibular incisors. The objective of the treatment was (1) to intrude and proclined the upper incisors, (2) to retroclined the lower incisors. (3) obtaining class I canine relation. (4) obtaining ideal overjet and overbite. (5) obtaining ideal esthetics.
Figure 2.

Pre-treatment intraoral photographs
Treatment progress
Patient was treated with a combination of face mask and RME [Figures 3-5] until 2 mm positive overjet was achieved. The expansion screw was activated one to three turns (0.25 mm/turn) at weekly visits until the desired amount of expansion had been achieved. The face mask was adjusted to rest on the forehead and the chin of the patient. Elastics (5/16 inch by 14 ounces) were worn from hooks located 2-3 cm in front of the lips to the intraoral attachments located on the expansion appliance, approximately at the gingival level of the canine. The force generated by the elastics was 600-800 g bilaterally.
Figure 3.

Rapid maxillary expansion appliance
Figure 5.
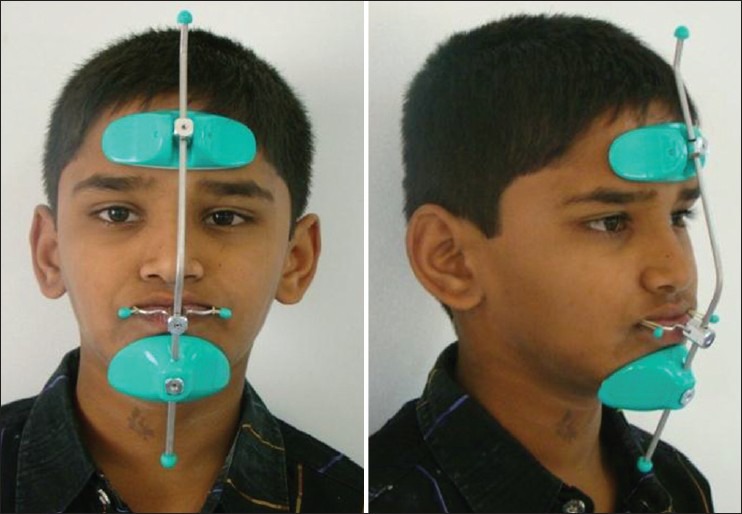
The face mask applaince
Figure 4.
Rapid maxillary expansion appliance
After duration of 9 months of orthopedic correction, then the pre-adjusted edgewise appliance was fixed with extraction of lower 1st premolar and treatment was continued for 12 months.
Treatment results
Maxillomandibular relations [Figures 6 and 7] showed significant improvements during the treatment period, with changes due primarily to the increase in the Sella –nasion- point A angle (SNA) angle. The Sella-nasion-point B (SNB) angle showed no significant changes during protraction. The dental measurements showed a tendency for the upper incisors to flare during treatment; the lower incisors were uprighted significantly. Upper or lower molar angulations did not change during treatment.
Figure 6.

Post-treatment intraoral photographs
Figure 7.

Post-treatment extra-oral photographs
Discussion
This case report showed the results of the treatment of patients with class III malocclusion at an early stage with an efficient orthodontic therapy of RME plus maxillary protraction.
Class III combination therapy is a comprehensive non-surgical treatment strategy designed for developing skeletal class III malocclusions by incorporating orthodontic and orthopedic mechanics to effectively improve the patient's occlusion and profile. In properly selected cases, this modality of treatment can be a successful alternative that satisfies a patient's request to avoid surgery or premolar extraction.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Masucci C, Franchi L, Defraia E, Mucedero M, Cozza P, Baccetti T. Stability of rapid maxillary expansion and facemask therapy: A long-term controlled study. Am J Orthod Dentofacial Orthop. 2011;140:493–500. doi: 10.1016/j.ajodo.2010.09.031. [DOI] [PubMed] [Google Scholar]
- 2.Gianelly AA, Brosnan P, Martignoni M, Bernstein L. Mandibular growth, condyle position and Fränkel appliance therapy. Angle Orthod. 1983;53:131–42. doi: 10.1043/0003-3219(1983)053<0131:MGCPAF>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Tollaro I, Baccetti T, Franchi L. Mandibular skeletal changes induced by early functional treatment of class III malocclusion: A superimposition study. Am J Orthod Dentofacial Orthop. 1995;108:525–32. doi: 10.1016/s0889-5406(95)70053-6. [DOI] [PubMed] [Google Scholar]
- 4.Graber LW. Chin cup therapy for mandibular prognathism. Am J Orthod. 1977;72:23–41. doi: 10.1016/0002-9416(77)90122-1. [DOI] [PubMed] [Google Scholar]
- 5.Ferro A, Nucci LP, Ferro F, Gallo C. Long-term stability of skeletal class III patients treated with splints, class III elastics, and chincup. Am J Orthod Dentofacial Orthop. 2003;123:423–34. doi: 10.1067/mod.2003.70. [DOI] [PubMed] [Google Scholar]
- 6.Cozzani G. Extraoral traction and class III treatment. Am J Orthod. 1981;80:638–50. doi: 10.1016/0002-9416(81)90266-9. [DOI] [PubMed] [Google Scholar]
- 7.Rey D, Angel D, Oberti G, Baccetti T. Treatment and posttreatment effects of mandibular cervical headgear followed by fixed appliances in Class III malocclusion. Am J Orthod Dentofacial Orthop. 2008;133:371–8. doi: 10.1016/j.ajodo.2006.04.043. [DOI] [PubMed] [Google Scholar]
- 8.Irie M, Nakamura S. Orthopedic approach to severe skeletal class III malocclusion. Am J Orthod. 1975;67:377–92. doi: 10.1016/0002-9416(75)90020-2. [DOI] [PubMed] [Google Scholar]
- 9.Mermigos J, Full CA, Andreasen G. Protraction of the maxillofacial complex. Am J Orthod Dentofacial Orthop. 1990;98:47–55. doi: 10.1016/0889-5406(90)70031-7. [DOI] [PubMed] [Google Scholar]
- 10.McNamara JA., Jr An orthopedic approach to the treatment of class III malocclusion in young patients. J Clin Orthod. 1987;21:598–60. [PubMed] [Google Scholar]
- 11.Turley PK. Orthopedic correction of Class III malocclusion with palatal expansion and custom protraction headgear. J Clin Orthod. 1988;22:314–25. [PubMed] [Google Scholar]
- 12.Takada K, Petdachai S, Sakuda M. Changes in dentofacial morphology in skeletal class III children treated by a modified maxillary protraction headgear and a chin cup: A longitudinal cephalometric appraisal. Eur J Orthod. 1993;15:211–21. doi: 10.1093/ejo/15.3.211. [DOI] [PubMed] [Google Scholar]
- 13.Keim RG, Gottlieb EL, Nelson AH, Vogels DS., 3rd 2008 JCO study of orthodontic diagnosis and treatment procedures, part 1: Results and trends. J Clin Orthod. 2008;42:625–40. [PubMed] [Google Scholar]
- 14.Franchi L, Baccetti T, McNamara JA. Postpubertal assessment of treatment timing for maxillary expansion and protraction therapy followed by fixed appliances. Am J Orthod Dentofacial Orthop. 2004;126:555–68. doi: 10.1016/j.ajodo.2003.10.036. [DOI] [PubMed] [Google Scholar]
- 15.Anbuselvan GJ, Karthi M. Management of class III malocclusion in early permanent dentition. J Indian Dent Assoc Tamilnadu. 2010;2:68–70. [Google Scholar]