

Abstract
INTRODUCTION
Bochdalek hernia is one of the most common congenital abnormalities manifested in infants. In the adult is a rarity, with a prevalence of 0.17–6% of all diaphragmatic hernias. Right-sided Bochdalek hernias containing colon are even more rare, with no case described in the literature with ileo-cecal appendix.
PRESENTATION OF CASE
The authors present a case of a right-sided Bochdalek hernia in an adult female of 49 years old, presented with severe respiratory failure. During laparotomy for hernia correction, were found in an intrathoracic position the cecum and ileo-cecal appendix, the right colon and the transverse colon.
DISCUSSION
Although useful in patient evaluation, clinical history and physical examination are not helpful in making diagnosis because of their nonspecific character. CT scan is the most accurate exam for making diagnosis. Most of the times there is no hernial sac. Surgery is the treatment of choice, and it is always indicated even if asymptomatic. In general suture of the defect is possible. Due to patient's weak respiratory function we chose laparotomy by Kocher incision.
CONCLUSION
Being the first case of a right-sided Bochdalek hernia in the adult with a herniated ileo-cecal appendix, we name it Almeida-Reis hernia.
Keywords: Bochdalek, Hernia, Diaphragm, Ileo-cecal appendix, Almeida-Reis
1. Background
Bochdalek hernia is one of the most common abnormalities presented in infants,1,2 with a reported incidence between 1 in 2000 and 1 in 5000 live births.1,3,4 Most are diagnosed antenatally or in the neonatal period,5,6 and only 5% are diagnosed after the neonatal period3. In the adult is a rarity, with a prevalence of 0.17–6%3,7 of all diaphragmatic hernias. Similarly, in a review of 940 consecutive CT scans held by Gale in 1984, the prevalence was 6%.8 Since 1853–1992 there were only 100 cases of symptomatic Bochdalek hernias in the adult found in the literature.2,3,9 Right-sided hernia containing colon is even more rare, with only 12 cases described worldwide.10 In 2002 there were only 7 cases in the literature of symptomatic right-sided Bochdalek hernias.3 This is the first case reported of a right-sided Bochdalek hernia in the adult containing the ileo-cecal appendix, and we name it Almeida-Reis hernia.
2. Case report
A 49-year-old female patient resorted to emergency room for cough and sputum with 15 days of evolution, dyspnea worsening the night before, without abdominal complaints, no previous surgical operations, no trauma or recent travel. On physical examination had multiple wheezing and rales in both pulmonary fields, and fever (38 °C). Blood gases with pO2 of 43 mmHg, pCO2 of 42 mmHg, pH of 7.45, no anemia or leukocytosis, PCR 20.5. Chest X-ray showed bilateral pulmonary opacities. Pneumonia with global respiratory failure was diagnosed, initiating piperacilin plus tazobactam, and was submitted to tracheal intubation for mechanical ventilation in Intensive Care Unit (ICU). In an attempt to right subclavian vein catheterization an iatrogenic pneumothorax occurred. However this complication highlighted in the X-ray an image suspected of being a right diaphragmatic hernia. A thoracic CT scan was made, which confirmed the presence of a right-sided postero-lateral diaphragmatic hernia along with pulmonary opacities (Fig. 1). As there was no trauma history, a congenital diaphragmatic hernia was most likely, so a diagnosis of a right-sided Bochdalek hernia in the adult was made. By the 8th day in the ICU she was extubated, and after that the hernia's volume increased in the chest film (Fig. 2).
Fig. 1.
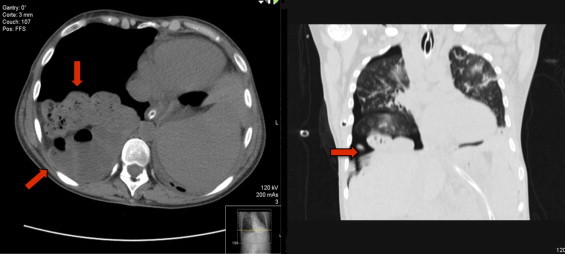
CT scan confirmed a right-sided Bochdalek hernia (red arrows). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Fig. 2.
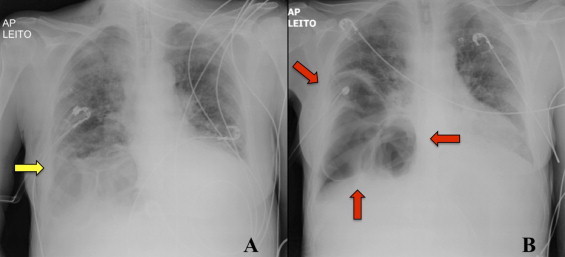
Right-sided diaphragmatic hernia in chest X-ray. (A) With mechanical ventilation the hernia is smaller (yellow arrow). (B) After extubation is noted an increase in hernia's volume (red arrows). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
The respiratory function was improving and surgical correction was performed. Laparotomy by a Kocher incision was chosen and a medial mobilization of the right lobe of the liver was necessary to approach the right-sided Bochdalek hernia. The hernia was brought back into the abdomen without difficulty, and it contained the cecum, ileo-cecal appendix, right colon, and proximal third of the transverse colon (Fig. 3). No hernial sac was found. The hernial defect had 6 × 3 cm (Fig. 4), and was closed without tension with a non-absorbable monofilament 0. No prosthesis was applied.
Fig. 3.

Hernia contained the ileo-cecal appendix, cecum, right colon, and proximal third of the transverse colon.
Fig. 4.

Postero-lateral defect in the right diaphragm.
In the post-op period the patient remained without cough, sputum or dyspnea, no pain, and doing respiratory training in the General Surgery Department. Thirteen days after surgery, chest X-ray was normal and she was discharged.
After 2 years of follow-up the patient is asymptomatic and without recurrence.
3. Discussion
The foramen of Bochdalek is a 2–3 cm opening in the postero-lateral aspect of the fetal diaphragm, through which there is communication between the pleural and peritoneal cavities.6 By the eighth week of embryonic life closure occurs by pleuroperitoneal membranes that grow ventrally and fuse with the septum transversum.2 Failure or incomplete fusion between the lateral (costal) and posterior (crural) components leads to hernia development. This closure failure was first described in 1848 by Bochdalek.3,9 In infants its manifestation can be severe, with respiratory stress and cyanosis, which requires urgent surgery.1–3 In adults Bochdalek hernia is usually an asymptomatic condition and an incidental finding.3,6 If symptomatic, clinical presentation can be varied but focused in the gastrointestinal and respiratory systems, causing chest pain, respiratory stress, abdominal pain, nausea, vomiting, intestinal incarceration and obstruction, and gastrointestinal perforation.2,5,7,9,10 Aside from vague and nonspecific, symptoms can be intermittent, since the viscera can return to abdomen spontaneously.7 Presentation with severe symptoms has been reported in 46% of cases, with 32% of mortality because of visceral strangulation7 and sudden death due to intrathoracic complications. Because the left defect closes later, 85% of Bochdalek hernias are left-sided. Stomach, ileum, colon and spleen are the organs that are more often herniated, but the liver and kidney can be found in conjunction with intestinal loops in right-sided hernias.8
Although useful in patient evaluation, clinical history and physical examination are not helpful in making diagnosis because of their nonspecific character.2 The most common presentation is thoracic and abdominal pain, respiratory stress, bowel obstruction, and a normal chest film does not rule out the presence of a Bochdalek hernia.2 These points were present in the case reported, whose clinical presentation was dominated by severe respiratory failure, and the initial chest film did not reveal the hernia.
CT scan is the most accurate exam for making diagnosis,1,2,7,9,10 and with its increasing use more asymptomatic cases are being diagnosed. Without CT almost 38% of adults are misdiagnosed with pleural effusion, empyema and pneumothorax.7 Ultrasonography plays a role in antenatal period, as it can diagnose a congenital diaphragmatic hernia in utero.9 MRI can also be useful in showing the relationships of the thoracic mass to the diaphragm.2 In the case reported only the chest X-ray after the iatrogenic pneumothorax highlighted an image suspected of hernia, and was the CT scan the exam that confirmed the diagnosis. It is also important to emphasize the effect of mechanical ventilation in hernia's volume reduction, which may have played a role in the fast respiratory function recovery, as after extubation it is evident the increase of its volume in the chest film.
Surgery is the treatment of choice, with a mortality rate of less than 4% for elective surgery2 and 32% for emergency surgery.3 There is usually no recurrence, and patients remain free of symptoms.9 Surgery is always indicated even if asymptomatic, because of possible serious complications from contents strangulation.2,7 In general suture of the defect is possible, and in a small number of cases prosthesis is needed.2 In fact the few cases of recurrence have been reported with the use of prosthesis,1 which may be related to the greater extent of the defect in those patients. Most of the times there is no hernial sac, although it can be present in 10% to 38% of Bochdalek hernias.3,7 Thoracoscopy, laparoscopy, thoracotomy and laparotomy are all valid approaches, being the late the most common choice. Authors who advise for thoracotomy refer to the greater ease in separating adhesions between the thoracic viscera and the hernial sac,11 however the presence of sac is not the rule. Those who favor laparotomy believe the abdominal approach is superior in recognition and management of a concomitant malrotation, and in the treatment of possible viscera incarceration and/or obstruction.3,12 Oliveira et al. advise a combined approach (laparotomy plus thoracotomy) for right-sided hernias, for greater ease in overtaking the liver mass effect.3,13 Minimally invasive surgery has been described in the correction of Bochdalek hernias, but should only be considered in adults because success increases with the age.3,14,15
In this case there was no sac, the hernia was right-sided, and contained colon, which makes it even more rare, as hernias containing colon are usually left-sided.3,7 In a 2009 Medline review there were 32 cases of Bochdalek hernia containing colon in children and adults, 11 of those in the right, one with appendicitis because of transverse colon obstruction, but none containing the ileo-cecal appendix.3 The authors reviewed 26 cases of Bochdalek hernia containing colon in the adult, and in none the ileo-cecal appendix appears herniated in the thorax (Table 1). This is the first case of a right-sided Bochdalek hernia in the adult containing the ileo-cecal appendix and we name it Almeida-Reis hernia, as a variant of Bochdalek hernia.
Table 1.
Cases of right-sided Bochdalek hernia containing colon but none with ileo-cecal appendix.
| Authors | Number of cases | Age | Side | Content | Ileo-cecal appendix |
|---|---|---|---|---|---|
| Kavanagh et al., Acta Chir Belg 2008; 108(5):604–606. | 1 | 76y | Right | Transverse colon | No |
| Kumar et al., World Journal of Emergency Surgery, 2009; 4:16. | 1 | 46y | Left | Transverse colon | No |
| Luciano et al., Chir Itl 2008, 60(4):583–586. | 1 | 45y | Right | Colon loop | No |
| Losanoff et al., Hernia 2004; 8(1):83–85. | 1 | 29y | Left | Transverse colon, omentum | No |
| Esmer et al., Hernia 2008; 12(3):307–309. | 1 | 42y | Left | Left colon | No |
| Rout et al., Hernia 2007; 11(4):359–362. | 1 | 35y | Right | Transverse colon (blind loop) | No |
| Laaksonen et al., J Med Case Reports 2009; 3:9291. | 1 | 38y | Right | Flexure hepatica of the colon, right lobe of the liver | No |
| Kocakusak et al., Hernia 2005; 9:284–287. | 1 | 21y | Left | Transverse colon | No |
| Chai et al., J Thorac Cardiovasc Surg 2005; 130(6):1729–1730. | 1 | 46y | Left | Colon | No |
| Terzi et al., Asian Cardiovasc Thorac Ann 2008; 16:42–44. | 1 | 70y | Right | Colon, omentum | No |
| Hamoudi et al., Int J Obstet Anesth 2004; 13(4):284–286. | 1 | 41y | Left | Stomach, transverse colon, spleen | No |
| Court et al., Int Surg 2003; 88:9–11. | 1 | 40y | Right | Colon, liver | No |
| Kanazawa et al., Surg Today 2002; 32:812–815. | 1 | 63y | Right | Transverse colon | No |
| Harinath et al., Surg Laparosc Endosc Percutan Tech 2002; 12(3):180–183. | 1 | Adult | Left | Stomach, colon | No |
| Iiai et al., Kyobu Geka 1997; 50(11):968–970. | 1 | 38y | Left | Transverse colon | No |
| Ohura et al., Kyobu Geka 1996; 49(5):420–423. | 1 | 35y | Left | Small bowel, colon | No |
| Kashima et al., Kyobu Geka 1993; 46(9):819–822. | 1 | 70y | Left | Colon | No |
| Sinha et al., Thorax 1989; 44(9):762–763. | 1 | 70y | Right | Right colon, transverse colon | No |
| Slesser et al., J R Soc Med Sh Rep 2011; 2:1–5. | 1 | 37y | Right | Right colon | No |
| Rimpilainen et al., Eur J Surg 2002; 168:646–647. | 1 | 22y | Right | Liver, gallblader, right colon, ileum, right ovary | No |
| Granier et al., Case Rep in Med 2010; 1–4. | 1 | 54y | Right | Ileum, cecum, right colon | No |
| Gymovsky et al., J Reprod Med 1983; 28:156–158. | 1 | 20y | Right | Colon | No |
| Fraser et al., Surg Laparosc Endosc Percutan Tech 2009; 19:5–7. | 1 | 75y | Right | Colon, small bowel right kidney | No |
| Zenda et al., Abdom Imaging 2000; 25:394–396. | 1 | 69y | Right | Ileum, transverse colon, gallblader | No |
| Wg Cdr A Alam et al., MJAFI 2005; 61: 284–286. | 1 | 35y | Right | Stomach, small bowel, colon, right lobe of the liver | No |
| Mohammadhosseini et al., L Coll Physicians Surg Pak 2008; 18(4):239–241. | 1 | Adult | Left | Colon | No |
Due to the patient's weak respiratory function we chose laparotomy by Kocher incision, avoiding pneumoperitoneum of laparoscopy, the largest morbidity of thoracotomy, and the possible greater difficulty in reduction a right-sided hernia by thoracic approach. The defect was easily sutured with a non-absorbable monofilament without tension, and because of that prosthesis was not applied. Patient remained asymptomatic and without recurrence in the 2 years of follow-up, matching other case reports data.
4. Conclusion
The lack of awareness for this pathology along with its nonspecific symptoms, often lead to an incorrect diagnosis.2 A low threshold of suspicion is extremely important in order to make a timely diagnosis and treatment.
Being the first case reported of a right-sided Bochadalek hernia in the adult containing the ileo-cecal appendix, we call this Almeida-Reis hernia, as a variant of Bochdalek hernia.
Conflict of interest
All authors declare no conflict of interest.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Data collection, manuscript writing and manuscript review done by CECA. Also, LSR and CMCA done the manuscript review.
References
- 1.Capizzani T., Hirschi R.B., Cilley R.E. Greenfield's Surgery. fifth ed. Lippincott William & Wilkins; 2011. The pediatric chest; pp. 1853–1883. [Google Scholar]
- 2.Seenhui L.H., Tjan A., Tham R.T.O., Smeenk F.W.J.N. Bochdalek hernia: a rare cause of pleural empyema. European Respiratory Journal. 1994;7:204–206. [PubMed] [Google Scholar]
- 3.Kumar A., Maheshwari V., Ramakrishnan T.S., Sahu S. Caecal perforation with faecal peritonitis unusual presentation of Bochdalek hérnia in an adult: a case report and review of literature. World Journal of Emergency Surgery. 2009;4:16. doi: 10.1186/1749-7922-4-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Terzi A., Tedeschi U., Lonardoni A., Furia S., Benato C., Calabrò F. A rare cause of dyspnea in adult: a right Bochdalek's hernia-containing colon. Asian Cardiovascular and Thoracic Annals. 2008;16:42–44. doi: 10.1177/021849230801600523. [DOI] [PubMed] [Google Scholar]
- 5.Kavanagh D.O., Ryan R.S., Waldron R. Acute dyspnoea due to an incarcerated right-sided Bochdalek's hernia. Acta Chirurgica Belgica. 2008;108(5):604–606. doi: 10.1080/00015458.2008.11680298. [DOI] [PubMed] [Google Scholar]
- 6.Granier V., Coche E., Hantson P., Thoma M. Intrathoracic caecal perforation presenting as dyspnea. Case Reports in Medicine. 2010:1–4. doi: 10.1155/2010/296730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gedik E., Tuncer M.C., Avci A., Tacyildiz I., Bac A. A review of Morgagni and Bochdalek hérnias in adults. Folia Morphologica. 2011;70:1. [PubMed] [Google Scholar]
- 8.Gale M.E. Bochdalek hernia: prevalence and CT characteristics. Radiology. 1985;156:449–452. doi: 10.1148/radiology.156.2.4011909. [DOI] [PubMed] [Google Scholar]
- 9.Wg Cdr A. Alam, Gp Capt B.N. Chander. Adult Bochdalek hernia. Medical Journal Armed Forces India. 2005;61:284–286. doi: 10.1016/S0377-1237(05)80177-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Slesser A.P., Ribbans H., Blunt D., Stanbridge R., Buchanan G.N. A spontaneous adult right-sided Bochdalek hernia containing perforated cólon. Journal of the Royal Society of Medicine Short Reports. 2011;2:1–5. doi: 10.1258/shorts.2011.011056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sugg W.L., Roper C.L., Carlsson E. Incarcerated Bochdalek hernias in the adult. Annals of Surgery. 1964;160:847–851. doi: 10.1097/00000658-196411000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fingerhut A., Baillet P., Oberlin P., Ronat R. More on congenital diaphragmatic hernia in adult (letter) International Journal of Surgery. 1984;69:182–183. [PubMed] [Google Scholar]
- 13.Oliveira F., Oliveira F.J. Congenital posterolateral diaphragmatic hérnia in the adult. Canadian Journal of Surgery. 1984;27:610–611. [PubMed] [Google Scholar]
- 14.Yamaguchi M., Kuwano H., Hashizume M., Sugio K., Sugimachi K., Hyoudou Y. Thoracoscopic treatment of Bochdalek hérnia in the adult: report of a case. Annals of Thoracic and Cardiovascular Surgery. 2002;8:106–108. [PubMed] [Google Scholar]
- 15.Wadhwa A., Surendra J.B.K., Sharma A., Khullar R., Soni V., Baijal M., Chowbey P.K. Laparoscopic repair of diaphragmatic hérnias: experience of six cases. The Asian Journal of Surgery. 2005;28:145–150. doi: 10.1016/S1015-9584(09)60281-5. [DOI] [PubMed] [Google Scholar]