

Abstract
Sarcoidosis is a multisystem, inflammatory disorder characterized by the presence of noncaseating epithelioid granulomas. Sarcoidosis can involve the genitourinary system by affecting the kidney and genitals. Most characteristic genital lesions proceed to granuloma and can comprise the epididymis, testis, and vas deferens. Few case reports have been published on this rare entity. We report a case in which a man presented with bilateral epididymal sarcoidosis and severe oligospermia. Corticosteroid treatment, which was applied in gradually decreasing doses for 6 months, dissolved the testicular granuloma. Consequently, semen analysis demonstrated a significant increase in the sperm count to within normal limits.
Keywords: Infertility, Testicular diseases, Sperm count, Spermatogenesis
INTRODUCTION
Sarcoidosis is a chronic, multisystem granulomatous disorder that is relatively common and is characterized histologically by the presence of noncaseating epithelioid cell granulomas in affected tissues with unclear etiology [1]. The possible presentations are diverse, with respiratory, ophthalmological, dermatological, endocrine, and reproductive complications. The frequency of genitourinary sarcoidosis in men is <0.2% in clinically diagnosed cases and 5% in autopsy studies [2]. Initial presentation can include an asymptomatic, painless mass in the scrotum, acute epididymo-orchitis, and testicular swelling. Previous cases of bilateral testicular sarcoidosis presented with azoospermia or oligospermia and hypogonadism, and high-dose corticosteroid therapy resulted in partial or no recovery of spermatogenesis and gonadal function [2-4]. The effect of genitourinary sarcoidosis on fertility has not been studied much, but it is rational to assume that the fibrosis and occlusion of the ductus epididymis seen in this disease could cause oligospermia and infertility [1,5].
CASE REPORT
We report on the case of a 25-year-old Caucasian man who presented to the outpatient clinic complaining of right scrotal stiffness for 1 year and new left scrotal pain and tenderness. He had been diagnosed with sarcoidosis by a mediastinal lymph node biopsy owing to a hilar lymphadenopathy 2 years previously after presenting with an acute onset and progressive course of fatigue and cough. The physical examination revealed multiple, painless subcutaneous nodules on his arms and upper thighs in addition to large, bilateral epididymal masses. The consistency and size of the testes were normal and there were no signs of varicocele on the physical examination. Laboratory investigations revealed a normal blood sugar concentration and normal liver and kidney functions with a slightly elevated erythrocyte sedimentation rate (14 mm/h). Moreover, serum α-fetoprotein and β-human chorionic gonadotropin were within the normal range. The urine was negative for acid-fast bacilli by Ziehl-Neelsen stain, which was repeated three times. Biochemical analysis revealed normal serum testosterone (15.85 nmol/L; normal range, 10.07 to 38.76 nmol/L) and luteinizing hormone levels (3 IU/L; normal range, 0.9 to 7.0 IU/L) and elevated serum follicle-stimulating hormone levels (15.4 IU/L; normal range, 1.5 to 12.4 IU/L). Semen analysis showed severe oligospermia (2×106/mL, Table 1).
TABLE 1.
Response of follicle-stimulating hormone (FSH), luteinizing hormone (LH), testosterone, and sperm count to prednisone therapy

T1-weighted post-contrast magnetic resonance imaging (MRI) revealed an enlarged and enhanced epididymis on both sides (Fig. 1). The sizes of the lesions in the right and left epididymis were 3.1 cm and 1.3 cm, respectively.
FIG. 1.

Magnetic resonance imaging showing T1 sagittal postcontrast-enhanced lesions on the (A) left and (B) right epididymides.
The patient underwent inguinal exploration to differentiate the scrotal malignancy. Exploration revealed enlargement of both epididymides with increased bilateral vascularity and firm consistency of the mass. The masses extended from the epididymis through the testis with thick adherent coverings. Incision of the tunica albuginea demonstrated normal seminiferous tubules with no mass in the testis. A biopsy sample was obtained from the epididymal mass for frozen section analysis. The sample revealed multiple noncaseating epithelioid granulomas (Fig. 2). Because the patient had been diagnosed with pulmonary sarcoidosis 2 years ago, malignancy of the testis and epididymis was ruled out easily and medical treatment considered.
FIG. 2.
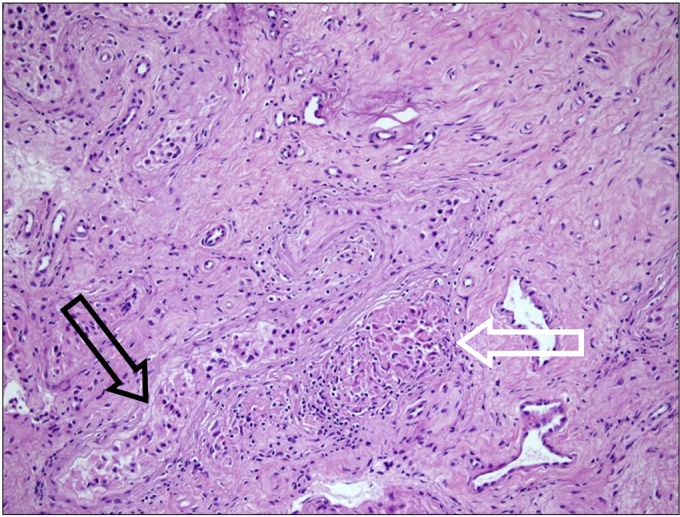
Epithelioid granuloma (white arrow) beside the epididymal duct (black arrow) (H&E, ×100).
The patient was given 40 mg of prednisone/d for 1.5 months. Subsequently, the dosage was reduced to 20 mg/d, which was administered for another 1.5 months. After the first 3 months, the prednisone dose was tapered every month and the patient received the drug as 10-mg, 5-mg, and 2.5-mg tablets during the fourth, fifth, and sixth months, respectively. As a result, the prednisone was gradually reduced to a maintenance dose of 2.5 mg/d at the end of 6 months (Table 1). The patient discontinued the medicine 1 month after the maintenance dose was achieved. During the follow-up period, the patient underwent physical examination with repeated semen and biochemical analysis every 3 months (Table 1). The results of the semen analysis at the end of therapy showed a dramatically increased sperm count of 34.7×106/mL with normal follicle-stimulating hormone and testosterone levels.
DISCUSSION
Sarcoidosis is a multisystem granulomatous disorder with a prevalence of 1 to 64 in 100,000 individuals [3,6]. The etiology of sarcoidosis remains unclear, although it was documented as a disease of activated T lymphocytes [1]. Onset is most commonly between the ages of 20 and 40 years, although the disease is occasionally reported in childhood and in the elderly. Although rare, sarcoid granulomas can be found in the genitourinary system in order of decreasing frequency in the epididymis, testis, and prostate gland, with only rare involvement of the spermatic cord, scrotum, and penis [6,7]. In MRI, these lesions exhibit enhancement on contrast-enhanced T1-weighted images and low signal intensity on T2-weighted images [8]. Open testicular biopsy is performed to exclude malignancy, because sarcoidosis is diagnosed concomitantly in 31% of cases with all types of testicular tumors [9].
Testicular and epididymal sarcoidosis must be differentiated from other causes of granulomatous disease that affect these tissues, including tuberculosis, syphilis, filariasis, lymphogranuloma venereum, granuloma inguinale, blastomycosis, coccidioidomycosis, actinomycosis, schistosomiasis, and Wegener's granulomatosis. Histopathology of the biopsy should demonstrate noncaseating microorganism-negative granulomas with epithelioid cells and large, multinucleated giant cells [2,3].
The goal of therapy in sarcoidosis is to prevent or minimize inflammation and granuloma formation (i.e., disease activity) leading to organ system dysfunction, which may ultimately cause end-stage organ destruction through the development of hyaline fibrosis. Corticosteroids remain the therapy of choice for sarcoidosis patients with multi-system involvement [4,6]. However, the role of corticosteroids in treating epididymal involvement is controversial and there are so few studies on this issue [4]. In the past, Ryan et al. [5] expressed that symptomatic epididymal sarcoidosis may require excisional biopsy in addition to steroid treatment for cessation of pain.
Azoospermia or oligospermia and therefore fertility problems may arise from sarcoidal involvement of the epididymis. The periductal distribution of the granulomas may cause extrinsic ductal compression or Leydig cell damage [4]. Svetec et al. [10] illustrated that a patient with normal fertility at the onset of the sarcoidosis diagnosis can progress to azoospermia. Because sarcoid granulomas of the epididymis and the resultant ductal obstruction can result in spontaneous exacerbations and remissions, Svetec and associates offered the use of sperm banking for possible future assisted reproductive techniques.
Rees et al. [4] reported a case of bilateral testicular sarcoidosis with azoospermia and hypogonadism. Rees et al. [4] showed partial recovery of spermatogenesis (sperm count, 1.2×106) and gonadal function in a patient treated with high-dose steroids. Recently, Hassan et al. [3] applied 12-month steroid treatment for a patient who had bilateral testicular sarcoidosis and azoospermia. Although the size of the lesions decreased, his semen analysis remained as azoospermic.
We showed complete recovery of spermatogenesis and gonadal function in a patient with bilateral testicular sarcoidosis treated with high-dose corticosteroids. To our knowledge, this is one of the first reports in which spermatogenesis and gonadal function were studied prospectively and in which normal results on semen analysis were achieved. Our case shows that steroid therapy may assist with the suppression of sarcoidal lesions in the epididymis and restore patency.
Footnotes
The authors have nothing to disclose.
References
- 1.Porter N, Beynon HL, Randeva HS. Endocrine and reproductive manifestations of sarcoidosis. QJM. 2003;96:553–561. doi: 10.1093/qjmed/hcg103. [DOI] [PubMed] [Google Scholar]
- 2.Turk CO, Schacht M, Ross L. Diagnosis and management of testicular sarcoidosis. J Urol. 1986;135:380–381. doi: 10.1016/s0022-5347(17)45648-5. [DOI] [PubMed] [Google Scholar]
- 3.Hassan A, El-Mogy S, Zalata K, Mostafa T. Bilateral epididymal sarcoidosis. Fertil Steril. 2009;91:1957. doi: 10.1016/j.fertnstert.2008.12.091. [DOI] [PubMed] [Google Scholar]
- 4.Rees DA, Dodds AL, Rathbone N, Davies JS, Scanlon MF. Azoospermia in testicular sarcoidosis is an indication for corticosteroid therapy. Fertil Steril. 2004;82:1672–1674. doi: 10.1016/j.fertnstert.2004.07.950. [DOI] [PubMed] [Google Scholar]
- 5.Ryan DM, Lesser BA, Crumley LA, Cartwright HA, Peron S, Haas GP, et al. Epididymal sarcoidosis. J Urol. 1993;149:134–136. doi: 10.1016/s0022-5347(17)36023-8. [DOI] [PubMed] [Google Scholar]
- 6.Handa T, Nagai S, Hamada K, Ito I, Hoshino Y, Shigematsu M, et al. Sarcoidosis with bilateral epididymal and testicular lesions. Intern Med. 2003;42:92–97. doi: 10.2169/internalmedicine.42.92. [DOI] [PubMed] [Google Scholar]
- 7.Rudin L, Megalli M, Mesa-Tejada R. Genital sarcoidosis. Urology. 1974;3:750–754. doi: 10.1016/s0090-4295(74)80218-9. [DOI] [PubMed] [Google Scholar]
- 8.Woodward PJ, Sohaey R, O'Donoghue MJ, Green DE. From the archives of the AFIP: tumors and tumorlike lesions of the testis: radiologic-pathologic correlation. Radiographics. 2002;22:189–216. doi: 10.1148/radiographics.22.1.g02ja14189. [DOI] [PubMed] [Google Scholar]
- 9.Paparel P, Devonec M, Perrin P, Ruffion A, Decaussin-Petrucci M, Akin O, et al. Association between sarcoidosis and testicular carcinoma: a diagnostic pitfall. Sarcoidosis Vasc Diffuse Lung Dis. 2007;24:95–101. [PubMed] [Google Scholar]
- 10.Svetec DA, Waguespack RL, Sabanegh ES., Jr Intermittent azoospermia associated with epididymal sarcoidosis. Fertil Steril. 1998;70:777–779. doi: 10.1016/s0015-0282(98)00272-6. [DOI] [PubMed] [Google Scholar]