

Abstract
Background An international review of the Cambodian Expanded Programme on Immunization (EPI) in 2010 and other data show that despite immunization coverage increases and vaccine preventable diseases incidence reductions, inequities in access to immunization services exist. Utilizing immunization and health systems literature, analysis of global health databases and the EPI review findings, this paper examines the characteristics of immunization access and outcome inequities, and describes proposed longer-term strategic and operational responses to these problems.
Findings The national programme has evolved from earlier central and provincial level planning to strengthening routine immunization coverage through the District level ‘Reaching Every District Strategy’. However, despite remarkable improvements, the review found over 20% of children surveyed were not fully immunized, primarily from communities where inequities of both access and impact persist. These inequities relate mainly to socio-economic exposures including wealth and education level, population mobility and ethnicity. To address these problems, a shift in strategic and operational response is proposed that will include (a) a re-focus of planning on facility level to detect disadvantaged communities, (b) establishment of monitoring systems to provide detailed information on community access and utilization, (c) development of communication strategies and health networks that enable providers to adjust service delivery according to the needs of vulnerable populations, and (d) securing financial, management and political commitment for ‘reaching every community’.
Conclusions For Cambodia to achieve its immunization equity objectives and disease reduction goals, a shift of emphasis to health centre and community is needed. This approach will maximize the benefits of new vaccine introduction in the coming ‘Decade of Vaccines’, plus potentially extend the reach of other life-saving maternal and child health interventions to the socially disadvantaged, both in Cambodia and in other countries with a similar level of development.
Keywords: Immunization, health equity, reaching every district, reaching every community
Introduction
The issue of equity in immunization
As international studies and reviews point increasingly to stagnation or at the very most only slight improvements in disparities in health access and health outcomes between social groups within countries, more attention is now being given to the problem of health equity and the related analytic standpoint of the social determinants of health. Studies are identifying that inequities in access to immunization and other maternal and child care services are largely related to social exposures of wealth and maternal education status (Mitchell et al. 2009; Semali 2010), urban vs rural location, and gender (Pande and Yazbeck 2003). A recent review of studies from 54 countries has established that there are major gaps in coverage for key maternal and child health care, and there are no signs that these coverage gaps are significantly narrowing (Boerma et al. 2008).
In terms of immunization strategy, both campaigns (Bonu et al. 2003; Vijayaraghavan et al. 2007) and routine strategies have demonstrated some pro-equity effects. The Reaching Every District (RED) Strategy, launched by World Health Organization (WHO) and United Nations Children's Fund (UNICEF) in 2002, was designed to scale up coverage above 80% through application of five operational strategies, including re-establishing health outreach, supportive supervision, linking services with communities, monitoring and use of data for action, and planning and management of resources (WHO 2010a). Implementation in settings in Africa (Vandelaer et al. 2008; Ryman et al. 2009) and Asia (Soeung and Grundy 2006) has reported the capacity of the strategy to improve coverage, and to detect previously un-reached populations (Enkhtuya et al. 2009). At the same time, campaign delivery strategies have reached whole populations, which has been sufficient to interrupt transmission of polio and measles in many countries where regular access to health services is very low.
Equity and immunization in Cambodia
In 2011, Cambodia entered its 25th year of implementation of the national immunization programme. Following successful polio eradication efforts (the country’s last polio case was reported in 1997), and reduction in the incidence of other vaccine preventable diseases, Cambodia (population 13.4 million) became an early adopter of the RED strategy in order to sustain coverage above 80% for routine antigens in every district. In 2003, local guidelines were adopted and applied under the banner of ‘coverage improvement planning’ (Soeung and Grundy 2006).
The implementation of locally-based guidelines for RED in Cambodia (referred to as coverage improvement planning) indicated that the effects of contracting, micro-planning, social mobilization, supervision and a secure finance for outreach operations demonstrated an overall 16% rise in diphtheria-tetanus-pertussis (DPT3) coverage across 10 low-performing districts in a single year in 2003 (Soeung et al. 2006). Independent evaluations have highlighted important coverage improvement effects of performance-based remuneration through the immunization services strengthening (ISS) and health system strengthening windows of Global Alliance for Vaccines and Immunization (GAVI) (Abt Associated 2004; HLSP 2009). However, what is less clear are the social determinants of non-access to immunization, and, more importantly what needs to be done to narrow the disparities based on an understanding of these determinants. That is, although every district has been reached in Cambodia, not every community has.
Just who are these communities, where are they located, what are the reasons they remain un-immunized, and what needs to be done to reach them?
Utilizing information from recent Demographic and Health Surveys, published literature and the recent findings of an international immunization review, this case study will describe and analyse the past and current successes and challenges in relation to improving equity of access to immunization in Cambodia. On the basis of these findings, this paper will review and propose a strategic and operational way forward for Cambodia and for countries with similar levels of development in order to address the persisting challenge of inequity in immunization access.
Methods
Sources of data
The principal source of data for analysis of the evolution of the national programme was through the published literature on immunization in Cambodia. The literature review was conducted through PubMed database using search terms “health equity” and “immunization equity” and “immunization Cambodia”.
Equity data analysis was through Demographic Health Surveys (DHS) data, which enabled analysis of immunization coverage and mortality according to background characteristics of populations (wealth, education, location, gender) (Macro International Inc. 2011). DHS data are published by the National Institute of Public Health and National Institute of Statistics and made available publicly through the World Wide Web (Macro International Inc. 2011). This data enables analysis of immunization coverage by background characteristics of socio-economic status (wealth quintiles), education level (no education, primary education, secondary or higher), gender and location (urban and rural and provincial level statistics). The global immunization database of WHO provided data on immunization coverage and the incidence of vaccine-preventable diseases (WHO 2010b).
New data were provided by a review of the immunization programme in November 2010 which focused on an evaluation of equity in immunization (Ministry of Health 2010). Using a semi-structured questionnaire for district and health centre, and house-to-house community-level data collection formats, seven teams collected information from 100 villages, 56 health centres in 28 districts, in 19 provinces. The review focused specifically on collection and analysis of data on locations and reasons for under-immunized status of women and children. The sampling method was therefore purposeful, with active search by reviewers and key informants of under-immunized households. When arriving at a district, high-risk health centres and villages were identified based on analysis of district coverage data. When arriving at high-risk villages, assistance was obtained from the local village health volunteer and other key informants to identify households with under-immunized children. In addition to the semi-structured questionnaire data on immunization status, the opportunity was also taken by reviewers to obtain from families more in-depth qualitative information regarding the reasons for ‘under immunized’ status. ‘Under immunized’ in the context of this review was defined as no vaccination at all or missing scheduled doses according to age.
Framework for analysis
In terms of framework of analysis, equity is conceptualized as a ‘measure of difference’ in outcomes or impacts based on social or economic exposures such as wealth and education status, location and gender. Equity as a measure of difference can be contrasted with efficiency, which refers to the ‘average level of health’ in a society (Arokiasamy and Pradhan 2010). Although measures of both averages and disparities of health are important in public health impact assessment and should be measured simultaneously (Delamonica et al. 2005), the analysis in this paper will largely focus on the measures of difference, the reasons for the difference and what to do about it. ‘Measures of difference’ also infers a rationale for pursuing the concept of ‘fairness’ in public policy making. That is, while both inequality and inequity refer to differences, equity discourses suggest that these differences are fundamentally unjust (PAHO 1999). This concept of fairness will be applied in the final discussion section of this paper to justify why the authors consider that a health equity objective is an objective in its own right, in addition to being a strategy for enhancing disease control objectives.
Limitations of method
The authors would like to note here certain limitations of methods of data collection and analysis. Firstly, although the association of various social and economic exposures with immunization status does not necessarily reflect causal links between outcomes and exposures, the matching of qualitative findings of the programme review with these findings has reinforced our observation of the high probability of causal links between socio-economic disadvantage and immunization coverage in the Cambodian setting.
Secondly, in reference to the specific years of the DHS data, we recognize the limitation of comparison of data across countries from different years. Although this is a methods limitation, we reiterate that the main intent is to compare differences within countries and not across them. The value of the comparison across countries is limited in this analysis to the observation that inequities within countries are a major health policy challenge in the region.
Thirdly, with respect to the other main source of data (the immunization programme review) the reviewers adopted a purposeful sampling approach through active search for under-immunized populations. That is, the aim was to better understand the socio-economic barriers to immunization and health care access that were indicated by the DHS findings. The statistical findings from the review are therefore not intended to be representative of a cross-section of the general population, but rather of a specific sub-population (the under-immunized).
Findings
The evolution of strategy in the national programme
The immunization programme commenced in 1986, when security was a major constraint in the delivery of the programme in many parts of the country, necessitating more central and provincial campaign service delivery strategies. In 1993, United Nations (UN)-sponsored elections concluded a period of sustained armed conflict, followed by the launch of a health sector reform era in 1996. A network of 76 operational health districts and over 960 health centres was completed by the end of 2007 (Ministry of Health 2007), greatly extending the reach of public health services to the more than 13 000 villages of Cambodia.
Health equity is a major policy concern of the Ministry of Health, which has successfully scaled up an initiative of hospital equity funds nationally, resulting in increased utilization of hospital services by the socially disadvantaged (Noirhomme et al. 2007; Bigdeli and Annear 2009). This equity focus of the MOH has also been evident in the strengthening of a ‘district’ focus for health system development. These health system initiatives, coupled with lessons learned from campaign strategies (particularly in relation to micro-planning, workforce remuneration, supervision and partnerships) and the implementation of RED from 2003, have resulted in DPT3 coverage being scaled up nationally from 69% in 2003 to 94% in 2009. In early 2010 pentavalent DTP-HepB-Hib vaccine was introduced, and is now available in every health facility. A strategy to increase the utilization of fixed-site services for immunization has also demonstrated successes, with the rate of immunization provided at the health centres increasing from 20% in 2007 to 37% in 2009 (Ministry of Health 2009). But concerns were being expressed by managers and advisers regarding populations who have limited capacity to access these services due to socio-economic or distance constraints.
Immunization coverage in Cambodia
Figure 1 summarizes gains in immunization coverage and numbers immunized with DPT3 between 2000 and 2009 in Cambodia.
Figure 1.

Immunization coverage (DPT3) and immunization numbers, 2000–09, Cambodia Source: WHO (2010b).
Even with newly adjusted population figures in 2005, and again with census figures in 2008, DPT3 immunization numbers have continued to grow from 290 104 in 2000 to 339 196 in 2009. In one global review of data quality, Cambodia is reported to have been one of three countries that is utilizing immunization system strengthening funds from GAVI (for RED in this case), but not overestimating DPT3 numbers (based on comparisons with survey data) (Lim 2008), and this is also the reason why WHO/UNICEF official estimates are consistent with reported estimates between 2003 and 2009.
But despite these gains, vaccine preventable diseases persist in 2009, with 95 laboratory confirmed measles cases, and 27 neonatal tetanus cases. In the same year, from an estimated cohort of 359 071 births, 19 875 children under the age of 1 were not vaccinated with DPT3.
However, the fact these cases are still occurring provides the rationale for a more focused pro-equity planning strategy. So what evidence is there from Cambodia on the background characteristics of these un-immunized children and their mothers?
Equity analysis of immunization in Cambodia
Coverage equity
Utilizing the most recent data from countries that conducted DHS between 2002 and 2010, Figure 2 contrasts immunization coverage for DPT3 by wealth index.1 This data demonstrates that in seven out of eight countries the percentage gap in coverage between the two groups exceeds 20%. In Cambodia this gap is 21%.
Figure 2.

Comparative percentage difference in measles immunization coverage according to wealth index in last DHS Source: Macro International Inc. (2011).
Figure 3 compares and contrasts the percentage difference in measles coverage across the region (including global median) between the lowest and highest levels (for wealth index and education level) and between urban and rural locations.
Figure 3.
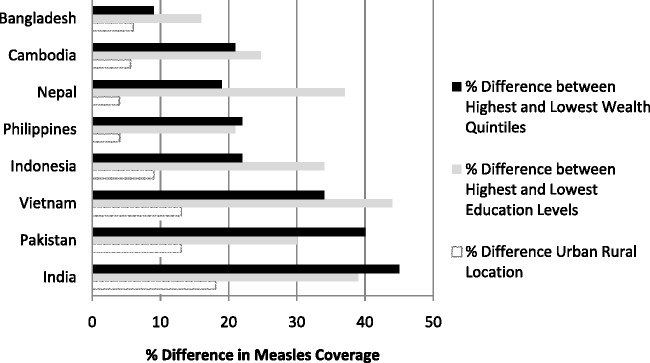
Comparative percentage difference in measles immunization coverage according to wealth index, education level and location (urban rural) in last DHS Source: WHO Global Observatory (2010).
In terms of the regional perspective and the global median, Cambodia rates reasonably well in this immunization equity analysis. With the exception of India, Pakistan and Nepal, where wealth status demonstrates the largest differences in coverage, the most significant differences in coverage in Cambodia relate to the education level exposure (24.7% difference in DPT3 coverage between highest and lowest education level, and 21% difference for highest and lowest wealth index). This is the reverse finding for that of maternal health (delivery by trained staff) where wealth status is the most significant exposure contributing to coverage disparity (Macro International 2010). This is reinforced by DHS data regarding trends in immunization equity.
Table 1 demonstrates narrowing of differences for measurable socio-economic exposures between the year 2000 and the year 2010 DHS. It is important to note, however, that these reductions in inequities of coverage have levelled out between 2005 and 2010.
Table 1.
Narrowing of immunization equity gaps in Cambodia 2000–2010
| Equity measures: wealth, education, location, gender | Percentage DPT3 DHS 2000 | Percentage DPT3 DHS 2005 | Percentage DPT3 DHS 2010 | % gaps 2000 | % gaps 2005 | % gaps 2010 |
|---|---|---|---|---|---|---|
| Highest household wealth | 74.7 | 84.0 | 92.6 | 35.7 | 18.4 | 19.1 |
| Lowest household wealth | 39.0 | 65.6 | 73.5 | |||
| Highest education level | 68.7 | 93.6 | 92.2 | 31.8 | 27.4 | 25.5 |
| Lowest education level | 36.9 | 66.2 | 66.7 | |||
| Urban location | 53.5 | 76.8 | 90.4 | 5.7 | −1.7 | 6.7 |
| Rural location | 47.8 | 78.5 | 83.7 | |||
| Male gender | 50.0 | 81.6 | 84.6 | 3.0 | 6.8 | -0.5 |
| Female gender | 47.0 | 74.8 | 85.1 |
Source: Macro International Inc. (2011).
Although absolute gaps in coverage between highest and lowest wealth quintiles (21%) and highest and lowest education levels (24.7%) in particular are still highly significant, the narrowing of the wealth gaps between 2000 and 2005 demonstrated an important trend (Hong 2010). However, the most recent DHS data released in October 2011 demonstrate that the equity gap for socio-economic exposures has not narrowed since 2005. In terms of other equity parameters, both urban/rural and gender disparities are negligible, and education level gaps in coverage have narrowed slightly (see Table 1).
More recently published preliminary data from the 2010 DHS confirm these trends of overall improved access of the broader population to immunization services but persisting equity gaps between socio-economic groupings. In the 2000 DHS in Cambodia, there was a 29.7% gap in coverage for fully immunized child status between population groups who had secondary education and higher and those who had no education at all. In the 2010 preliminary DHS findings, the gap remains at 29.2%. This is despite the fact that overall coverage (as measured by DHS in 2000 and 2010) had increased from 40% for fully immunized child status in 2000 to 78.8% in 2010 (National Institute of Statistics 2010).
What this analysis confirms is that it is socio-economic equity parameters (wealth and education level) that are the most strongly associated with lower access to immunization services in Cambodia and other regional countries, rather than other equity parameters including gender or location (see Figure 3).
Equity impacts
Improvements in efficiency (average health) and equity (narrowing of differences) can also be inferred from the sharp reductions in vaccine preventable diseases from the pre-vaccine era. In 1985, there were 44 557 measles cases, 1169 tetanus cases and 931 polio cases. In the vaccine era in the last 25 years, the last case of polio was reported in 1997, followed by regional polio elimination in 2000, and measles and tetanus cases have been reduced to 4779 and 24 cases, respectively, in 2009 (WHO 2010b).
But despite these gains, there is also evidence to indicate that the incidence of vaccine-preventable diseases is correlated to the socio-economic background characteristics of populations. Of the 229 confirmed neonatal tetanus cases between 2005 and 2009, 89% delivered at home and 77% were delivered by a traditional birth attendant (TBA) (Ministry of Health 2009). Given that 89% of all cases of neonatal tetanus occur with home deliveries and 77% under the care of a TBA, there is clearly a higher risk of transmission of neonatal tetanus in this context, when it is considered that only 11% of cases occurred in a facility setting. This is also consistent with international reviews of tetanus elimination strategies, which state that cases are most frequently clustered in ‘poor, remote, and disenfranchised communities where unhygienic obstetric and postnatal practices prevail’ (Roper et al. 2007: 10).
Analysis of child mortality data in Cambodia and regionally demonstrates a similar linking of outcomes to social variables of wealth status, education level and location. Figure 4 provides a comparative regional analysis of mortality rates in relation to wealth status.
Figure 4.

Comparative analysis of under-5 mortality rates by wealth index 2002–10 Source: Macro International Inc. (2011).
Cambodia demonstrates a 300% difference in under-5 mortality between the highest and lowest socio-economic groupings (mortality rate of 90/1000 for lowest wealth index, and 30/1000 for highest wealth index). Although the increase in immunization coverage in Cambodia would have contributed to child mortality reduction, the persistence of socio-economic and education level exposures as determinants of equity of access to immunization as demonstrated in Figures 2 and 3 indicates that these mortality gains have not been evenly spread across the social gradient.
Inequity exposures uncovered by the 2010 immunization review
Findings from the national EPI review in 2010 confirm the findings of the DHS data analyses, and have uncovered additional social exposures for un-immunized status that remain undetected from previous surveys.
In the review, the immunization status of children under 2 years was assessed by card only. Of 782 children that were interviewed across 28 districts, 652 (83%) had cards, 487 (75%) were adequately immunized for their age and 130 (20%) were partially immunized. There were 82 children who had not received any immunization and therefore held no cards. The main reasons provided by carers for their childrens’ under-immunized status was that the carer was ‘too busy’ (28%) and ‘mobile’ (23%).
In focusing on the main review objective which was to indentify women and children who have not received immunization services (and the reasons for not being immunized), the reviewers observed that traditional indicators of risk based on geography, though still important, can in some circumstances be less helpful in understanding access barriers than socio-economic categories of risk. Specific categories associated with under-immunization in the EPI review included mobile populations and migrant workers (48%), ethnic minorities (24%), urban poor (10%) and rural hard to reach (18%). The main point we are making here is that socially disadvantaged groups are overly represented in the under-immunized population. For example, minorities constitute no more than 7% of the general population (ADB 2002), but were frequently encountered in the sample of under-immunized population located by the review.
Thus ‘social distance’ rather than geographical distance predominated as the main determinant of immunization access. Social distance in this context can be described as the sense of distance that clients experience from health facilities and providers, as determined by the level of acceptability or affordability of their access to health care. In fact, the concept of social distance takes into account the fact that inequitable social conditions can be as powerful as remote geographical location in shaping the frequency and quality of health provider and community contacts (Tarlier et al. 2007). These qualitative observations match the DHS data findings which demonstrate narrowing of urban–rural differences in immunization access between 2000 and 2010, but persistence of socio-economic disparities in the same period.
The review also found that there were links between poverty and mobility. For families on very low incomes, daily mobility is required in order to meet the daily subsistence requirements for the family, which often results in children remaining in houses with grandmother or elder sibling care. Secondly, in order to meet the demand of a new economy, populations are shifting to new locations around garment factories or construction sites springing up around the capital city and provincial town locations. The fact that many of these mobile or migrant workers that have emerged with the new economy may not be recorded in health centre or local authority registers increases the risks that these populations will not be included in routine health system reporting.
Ethnicity and migration were also noted to be factors associated with low immunization status. These included Vietnamese floating villages, remote indigenous minorities and resident Cham (Muslim) villages. In these communities, communication barriers, mobility and lack of trust between these sub-communities and the health system were all presented in the review as barriers to access. Additionally, the review noted that urban slum populations were also at risk of lower immunization access.
Thus the review found that ‘social distance’ of communities from health systems is the main barrier to access, and measures associated with geographical access, though necessary, remain insufficient for taking actions towards ‘narrowing the difference’. The social and local area context for health access also led reviewers to conclude that sole reliance on district-focused approaches and tools, while still useful, has limited applicability in assisting to scale up coverage in the context of social disadvantage in local area communities.
Discussion and conclusions: future directions in immunization strategy
Equity analysis: what do we now know about immunization inequity?
The narrowing of differences demonstrated in the DHS data, the reductions in child mortality and the steady improvements in immunization coverage and numbers (in a country with an international track record for high data quality) are all promising trends. This optimism is supported by the findings of a review of 54 countries targeting MDG goals in 2015, where Cambodia was one of only three countries in the global sample that consistently measured more than an annual 2% improvement in coverage for key maternal and child health interventions since 1995 (Boerma et al. 2008). Moreover, in a range of international reviews, immunization has been identified as a programme that can achieve higher levels of equity in advance of other maternal and child health initiatives (Houweling et al. 2007; Boerma et al. 2008).
But nevertheless, there are also grounds for expressing caution in regards to inequity reductions. Although in many regards Cambodia has progressed far in conquering the challenge of narrowing the impacts of geographic distance through the RED strategy and related health system strengthening initiatives, the challenge remains on how to narrow the differences associated with social distance, particularly given the fact that the ongoing social and economic transition, with its patterns of migration, urbanization and marginalization, is a moving policy and practice target.
This is further borne out by the reports of a vaccine-derived polio case in the centre of Phnom Penh in 2005 (Okonko et al. 2009), the association of low education level, poverty and ethnic minority status with low immunization coverage rates in the RED analysis in 2003 (Soeung et al. 2006), and reports of lack of access to health services by slum dwellers in 2009 (UNICEF 2010). The ongoing social and economic transition, with associated high workforce mobility and internal migration, is likely to exert continuing pressures on health systems to adapt to social and economic change. This finding has also been noted in the contexts of Mongolia (Hindle and Khulan 2006) and China (Shaokang et al. 2002), where the impact of economic and social transition is resulting in the need to ‘rethink and redesign’ programmes and systems to specifically target disadvantaged social groups.
So what are the implications of these equity analyses for immunization and health system strategy in Cambodia and elsewhere?
Strategy implications: what needs to be done to promote equity in immunization?
Operationally, the findings in this paper show that a shift in planning focus is needed from a district-wide perspective down to a facility- and community-level system of analysis and operations. The district, as an operational unit, is less well placed to undertake social analysis and action at community level than the primary care facility and community-level networks that reside near disadvantaged groups. It is by the very fact that these communities are often more ‘hidden’ or ‘mobile’ that alternative and more sensitive community planning approaches will be required in order to recognize them and bring them back into the range of modern health and social services.
Box 1, based on the findings of the Cambodian EPI review, outlines in more detail the expected area of operational focus that would be applied to a ‘reaching every community approach’.
Box 1 Reaching Every Community strategies.
Re-focus planning systems: Developing facility- and community-level health planning systems in order to better understand and respond to the needs of vulnerable communities. This will involve not only mapping geographic risk, but also social risk. Who are the at-risk communities, where are they, what are the current reasons for non-access, and what special activities are required to improve access?
Building community-based monitoring systems: Building measurement of equity into health services practice (active search or ‘village-level monitoring’) in order to strengthen service access for vulnerable social groups. Such a system would quantify the level of services and access or lack thereof. It could also better monitor the equity impacts of immunization and related maternal and child health programmes. This means not only monitoring coverage and responding to disease outbreaks, but also active search in vulnerable communities for the un-immunized.
Special communication strategy: This will enable providers to adjust service delivery according to the special needs of special population groups. This will involve developing capacity for strengthening community-level health networks with non-governmental organizations, local authorities and women’s associations, in order to extend the communication and health monitoring links with vulnerable communities. Other main actions will include development of communication systems for early detection and registering (with health services or with local authorities) of mobile populations who are entering new health service population catchments.
Equitable service delivery: Modelling service delivery strategy on community needs and characteristics (fixed strategy, outreach strategy, health posts, community health education), implementing outreach service packages with immunization, and strengthening demand for fixed-site services, in order to maximize efforts for health access and poverty alleviation in vulnerable communities.
Mobilizing resources for disadvantaged populations: Securing political commitment for the narrowing of equity gaps, through targeted financing of communication and service delivery operations specifically for vulnerable groups, and agreeing on health equity targets in national and sub-national health plans. Based on findings in Cambodia, specific and targeted funding for service provision for vulnerable populations (with adequate performance-based remuneration packages for health workers) would be an essential part of a Reaching Every Community strategy.
KEY MESSAGES.
Although remarkable progress has been made in Cambodia with immunization coverage, the remaining unreached populations are characterized by specific exposures of social and economic disadvantage.
Current health system and immunization strategies are oriented towards a district-level focus for planning and operations.
The main lesson learned for countries in similar contexts is that, in order to reach every community, more sensitive local area planning instruments and operational strategies will be required at a sub-district level in order to promote and sustain equity in health services access and outcomes.
Such an approach is of increasing relevance as Cambodia and other developing countries take up opportunities enabled through GAVI to introduce new and underutilized vaccines. The most recent burden of disease data for Haemophilus influenzae type b (Hib) (annual expected case load of 39 567 pneumonia cases) and Streptococcus pneumoniae (annual expected case load of 66 056 pneumonia cases) illustrates the extent to which new and underutilized vaccine programmes have the potential to have further impact on child mortality reductions (WHO 2009c).
But the available data presented in this paper on the association between vaccination coverage and socio-economic status (income and education levels in particular as demonstrated in Figure 3) would seem to suggest that these new vaccines and technologies in Cambodia and regionally are not reaching the poorest children in the developing world at acceptable coverage rates.
The wide gaps in coverage between socio-economic classes as demonstrated in Figure 2, most notably in high population countries such as India and Indonesia, demonstrate the fact that, without targeted and well-financed operational strategies to reach out to the poorest and those with least access to education, inequities in access to life-saving interventions such as new vaccines are likely to persist, exacerbating already existing wide health and social gaps within countries. While it is recognized that pro-equity strategies in relation to immunization can support disease elimination and control objectives (particularly for measles elimination), equity objectives have value in their own right, in so far as they contribute to the level of fairness and well being in society. That is, the pursuit of equity in health has wider health benefits for the society as a whole, and not only for the groups with highest risk (WHO 2009a).
The findings in this case study are consistent with the literature on health equity analysis internationally, which demonstrates two main findings. Firstly, it is the gaps within countries that are equally as instructive for health policy making as are the gaps between countries (Braveman and Tarimo 2002). Secondly, in the rush for universal coverage, it is often the most difficult to access that are left to last in order to achieve the most impressive population-level coverage in the shortest time frames (Gwatkin 2000; Gwatkin and Ergo 2011). In the interests of justice and fairness in health programming, both of these findings demonstrate the need for more rigorous and focused operational strategies to reach every community. That is, operational strategies should not only be guided by the drive for higher coverage, but also by the drive for more equitable coverage across the social gradient.
Conclusion
The proposed approach of ‘reaching every community’ in Cambodia is consistent with global health goals as elucidated in recent World Health Assembly resolutions, which call on ministries of health to measure and take action on the social determinants of health (WHO 2009a; WHO 2009b). Immunization programmes internationally are strongly placed to be a ‘front runner’ in this endeavour, given that immunization programmes have demonstrated the capacity to lower equity gaps more quickly than other maternal and child health interventions (Boerma et al. 2008). This also presents the possibility for immunization programmes to demonstrate impacts on wider health system strengthening, by acting where possible as a platform for delivery of a wider range of health delivery service packages for the socially disadvantaged, particularly in countries with immunization levels at 80% or above (Wallace 2009).
The Global Immunization Vision and Strategy (2006–15) expresses the vision of WHO, UNICEF and other partners to achieve equity in a world where every child, adolescent and adult has equal access to immunization by 2015 (WHO 2006). This includes ensuring that new and underutilized vaccines are available to all, especially in the poorest countries of the world. The data presented in this paper, both in Cambodia and regionally, demonstrate that the benefits of these new vaccines and technologies are not being distributed equitably enough across the social gradient.
Based on these findings, a shift in planning and operational emphasis is proposed here. By building on the experience of RED, this shift in operational emphasis from the district to the local community area will improve equity and maximize the benefits of new vaccine introduction both in Cambodia and other countries. Making a difference in the Decade of Vaccines will increasingly require planners to focus on ‘narrowing the social difference’. In doing so, it will be possible to measure and take action on the social determinants of health, in what is proving to be in matters of child health and survival, a persistently very unequal world.
Funding
The review of literature, data analysis and writing of this paper was made possible through a grant provided by the World Health Organization in Cambodia in 2011.
Conflict of interest
None declared.
Endnote
Footnotes
1 The years of the last DHS were as follows: last DHS conducted in Cambodia in 2010, India in 2005, Indonesia in 2007, Vietnam in 2002, The Philippines in 2008, Nepal in 2006, and Pakistan in 2007.
References
- Abt Associates. Evaluation of GAVI Immunization Services Support Funding Review of Immunization Services Strengthening Cambodia Case Study. 2004. Online at: http://www.gavialliance.org/resources/Evaluation_of_ISS_Funding_Aug04.pdf, accessed January 2010.
- ADB. Indigenous peoples/ethnic minorities and poverty reduction in Cambodia. Environment and Social Safeguard Division Regional and Sustainable Development Department, Asian Development Bank, Manila, Philippines. 2002. Online at: http://www.adb.org/sites/default/files/pub/2002/indigenous_cam.pdf, accessed 30 March 2012.
- Arokiasamy P, Pradhan J. Measuring wealth-based health inequality among Indian children: the importance of equity vs efficiency. Health Policy and Planning. 2010;26:429–40. doi: 10.1093/heapol/czq075. [DOI] [PubMed] [Google Scholar]
- Bigdeli M, Annear P. Barriers to access and the purchasing function of Health Equity Funds. Bulletin of the World Health Organization. 2009;87:560–4. doi: 10.2471/BLT.08.053058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boerma JT, Bryce J, Kinfu Y, Axelson H, Victora CG. Mind the gap: equity and trends in coverage of maternal, newborn, and child health services in 54 Countdown countries. The Lancet. 2008;371:1259–67. doi: 10.1016/S0140-6736(08)60560-7. [DOI] [PubMed] [Google Scholar]
- Bonu S, Rani M, Baker TD. The impact of the national polio immunization campaign on levels and equity in immunization coverage: evidence from rural North India. Social Science & Medicine. 2003;57:1807–19. doi: 10.1016/s0277-9536(03)00056-x. [DOI] [PubMed] [Google Scholar]
- Braveman P, Tarimo E. Social inequalities in health within countries: not only an issue for affluent nations. Social Science & Medicine. 2002;54:1621–35. doi: 10.1016/s0277-9536(01)00331-8. [DOI] [PubMed] [Google Scholar]
- Delamonica E, Minujin A, Gulaid J. Monitoring equity in immunization coverage. Bulletin of the World Health Organization. 2005;83:384–91. [PMC free article] [PubMed] [Google Scholar]
- Enkhtuya B, Badamusuren T, Dondog N, et al. Reaching every district – development and testing of a health micro-planning strategy for reaching difficult to reach populations in Mongolia. Rural and Remote Health. 2009;9:1045. [PubMed] [Google Scholar]
- Gwatkin DR. Health inequalities and the health of the poor: what do we know? What can we do? Bulletin of the World Health Organization. 2000;78:3–18. [PMC free article] [PubMed] [Google Scholar]
- Gwatkin DR, Ergo A. Universal health coverage: friend or foe of health equity? The Lancet. 2011;377:2160–1. doi: 10.1016/S0140-6736(10)62058-2. [DOI] [PubMed] [Google Scholar]
- Hindle D, Khulan B. New payment model for rural health services in Mongolia. Rural and Remote Health. 2006;6:434. [PubMed] [Google Scholar]
- HLSP. GAVI Health System Strengthening Support Evaluation 2009. 2009. Online at: http://www.gavialliance.org/performance/country_results/index.php?countID=11, accessed January 2010.
- Hong R, Chhea V. Trend and inequality in immunization dropout among young children in Cambodia. Maternal and Child Health Journal. 2010;14:446–52. doi: 10.1007/s10995-009-0466-1. [DOI] [PubMed] [Google Scholar]
- Houweling TA, Ronsmans C, Campbell OM, Kunst AE. Huge poor–rich inequalities in maternity care: an international comparative study of maternity and child care in developing countries. Bulletin of the World Health Organization. 2007;85:745–54. doi: 10.2471/BLT.06.038588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macro International Inc. Measure DHS, STATcompiler. 2011 Online at: http://www.statcompiler.com/index.cfm, accessed December 2011. [Google Scholar]
- Ministry of Health. Department of Planning and Health Information Phnom Penh: Ministry of Health; 2007. Joint Annual Program Review. [Google Scholar]
- Ministry of Health. Phnom Penh: Ministry of Health; 2009. Annual Progress Report to GAVI 2009. [Google Scholar]
- Ministry of Health. Phnom Penh: Ministry of Health; 2009a. National Immunization Program 2009. [Google Scholar]
- Ministry of Health. Phnom Penh: Ministry of Health; 2009b. Joint Annual Program Review (JAPR) 2009. [Google Scholar]
- Ministry of Health. Phnom Penh: Ministry of Health; 2010. National Immunization EPI Review 2010. [Google Scholar]
- Mitchell S, Andersson N, Ansari NM, et al. Equity and vaccine uptake: a cross-sectional study of measles vaccination in Lasbela District, Pakistan. BMC International Health and Human Rights. 2009;9(Suppl. 1):S1–S7. doi: 10.1186/1472-698X-9-S1-S7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute of Statistics. Phnom Penh: National Institute of Statistics; 2010. Cambodia Demographic and Health Survey, Preliminary Report. [Google Scholar]
- Noirhomme M, Meessen B, Griffiths F, et al. Improving access to hospital care for the poor: comparative analysis of four health equity funds in Cambodia. Health Policy and Planning. 2007;22:246–62. doi: 10.1093/heapol/czm015. [DOI] [PubMed] [Google Scholar]
- Okonko O, Ogun AA, Adedeji AO, et al. Circulating vaccine-derived poliovirus and its implications for polio surveillance and eradication in Nigeria: a review of the literature. Scientific Research and Essay. 2009;4:398–418. [Google Scholar]
- Pande RP, Yazbeck AS. What’s in a country average? Wealth, gender, and regional inequalities in immunization in India. Social Science & Medicine. 2003;57:2075–88. doi: 10.1016/s0277-9536(03)00085-6. [DOI] [PubMed] [Google Scholar]
- Pan American Health Organization (PAHO) Methodological summaries: measuring inequity in health. Epidemiological Bulletin. 1999;20:11. [PubMed] [Google Scholar]
- Roper M, Vandelaer J, Gasse F. Maternal and neonatal tetanus. The Lancet. 2007;370:1947–59. doi: 10.1016/S0140-6736(07)61261-6. [DOI] [PubMed] [Google Scholar]
- Ryman T, Macauley R, Nshimirimana D, et al. Reaching every district (RED) approach to strengthen routine immunization services: evaluation in the African region. Journal of Public Health. 2009;32:18–25. doi: 10.1093/pubmed/fdp048. [DOI] [PubMed] [Google Scholar]
- Semali IA. Trends in immunization completion and disparities in the context of health reforms: the case study of Tanzania. BMC Health Services Research. 2010;10:299. doi: 10.1186/1472-6963-10-299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaokang Z, Zhenwei S, Blas E. Economic transition and maternal health care for internal migrants in Shanghai, China. Health Policy and Planning. 2002;17(Suppl.):47–55. doi: 10.1093/heapol/17.suppl_1.47. [DOI] [PubMed] [Google Scholar]
- Soeung S, Grundy J. Improving immunization coverage through budgeted micro-plans and sub-national performance agreements: early experience from Cambodia. Asia Pacific Journal of Public Health. 2006;18:8. doi: 10.1177/10105395060180010601. [DOI] [PubMed] [Google Scholar]
- Lim SS, Stein DB, Charrow A, Murray CJL. Tracking progress towards universal childhood immunisation and the impact of global initiatives: a systematic analysis of three-dose diphtheria, tetanus, and pertussis immunisation coverage. The Lancet. 2008;372:2031–46. doi: 10.1016/S0140-6736(08)61869-3. [DOI] [PubMed] [Google Scholar]
- Tarlier DS, Browne AJ, Johnson J. The influence of geographical and social distance on nursing practice and continuity of care in a remote First Nations community. Canadian Journal of Nursing Research. 2007;39:126–48. [PubMed] [Google Scholar]
- UNICEF. Health service access among poor communities in Phnom Penh. 2010. Online at: http://www.unicef.org/eapro/Health_Service_Access_Among_Poor_Communities_Phnom_Penh_Low.pdf, accessed January 2010.
- Vandelaer J, Bilous J, Nshimirimana D. Reaching Every District (RED) approach: a way to improve immunization performance. Bulletin of the World Health Organization. 2008;86:A–B. doi: 10.2471/BLT.07.042127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vijayaraghavan M, Martin RM, Sangrujee N, et al. Measles supplemental immunization activities improve measles vaccine coverage and equity: evidence from Kenya, 2002. Health Policy. 2007;83:27–36. doi: 10.1016/j.healthpol.2006.11.008. [DOI] [PubMed] [Google Scholar]
- Wallace A, Dietz V, Cairns L. Integration of immunization services with other health interventions in the developing world: what works and why? Systematic literature review. Tropical Medicine and International Health. 2009;14:11–19. doi: 10.1111/j.1365-3156.2008.02196.x. [DOI] [PubMed] [Google Scholar]
- WHO. Commission on Social Determinants of Health. Sixty-Second World Health. 2009a Assembly, A62/9, Provisional agenda item 12.5, 16 March 2009. [Google Scholar]
- WHO. Primary health care, including health system strengthening. 2009b Sixty-Second World Health Assembly, A62/8, Provisional agenda item 12.4, 9 April 2009. [Google Scholar]
- WHO. Geneva: World Health Organization; 2009c. Estimates of severe illness cases and deaths in children from one month to less than five years of age due to Haemophilus influenzae type b (Hib) and Streptococcus pneumoniae (Spn) in Cambodia Expanded program on Immunization. [Google Scholar]
- WHO. Geneva: World Health Organization; 2010a. Guidelines for Reaching Every District. [Google Scholar]
- WHO. Geneva: World Health Organization; 2010b. Immunization Database Vaccine Preventable Diseases. Online at: http://www.who.int/immunization_monitoring/data/en/index.html, accessed January 2010. [Google Scholar]
- WHO Global Health Observatory. Global Health Observatory Data Repository. 2010. Online at: http://apps.who.int/ghodata/, accessed January 2010.
- WHO, UNICEF. Geneva: World Health Organization; 2006. Global Immunization Vision and Strategy. Online at: http://www.who.int/vaccines-documents/DocsPDF05/GIVS_Final_EN.pdf (Accessed January 2010) [DOI] [PMC free article] [PubMed] [Google Scholar]