

Abstract
Background:
Experimental studies provide evidence of a relationship between stroke and mineral intake but this information in human are still limited and inconsistent. The purpose of this study was to investigate sodium, calcium and iron intake and stroke in Iranian patient and control population.
Materials and Methods:
In a case-control study with 46 stroke men (aged 56 ± 18 years) and stroke women (aged 52 ± 7 years) and 60 healthy people, we investigated the sodium, calcium and iron intake inthe patients.
Results:
After adjustment for age, sex and cardiovascular disease we found that a high sodium intake was associated with a statistically significant higher risk of stroke (P < 0/05). We saw a significant association between iron intakes in men (P < 0/05). And calcium was not significant associated with risk of stroke (P for trend >0/05).
Conclusion:
These findings in men and women suggest that a low sodium intake may play a role in primary prevention of stroke.
Keywords: Calcium, diet, epidemiology, iron, minerals, sodium, stroke
INTRODUCTION
Stroke is one of the leading causes of disability and mortality in many developed countries.[1] It was estimated that 15 million new cases of stroke accrue worldwide annually.[1] Approximately 10% of the deaths in the world are related to stroke[1,2] and it is estimated that the incidence of stroke will increase during the next 20 years.[1,3] Dietary factors are associated with the risk of stroke,[1,4] for example, by the impact on blood pressure, resistance to insulin, systematic inflammation, thrombosis, and oxidation.[2,5] A diet rich in calcium, magnesium, and potassium may decrease the risk of stroke, whereas increasing intake of sodium can lead to higher blood pressure and risk of stroke,[1,6,7] but the effect of the intake of iron is not completely clear.[1,8] Due to the fact that minerals are essential elements for human body, some researchers have investigated the association between stroke and dietary intake of minerals, but the results are inconsistent.[1,9,10] So, we aimed to investigate the effect of dietary intake of minerals in patients with stroke.
MATERIALS AND METHODS
Surveys for this case control study were performed in the Alzahra Hospital in Iran from April 2010 through March 2011 We recruited subjects from two wards of this hospital; the incident stroke patients were referred from the inpatient wards of the neurology department and the control group from the normal population. The control group had neither history nor clinical evidence indicating a previous stroke, and their treatment at the outpatient department was not related to any cardiovascular disease, malignant tumor, or diabetes. We also excluded patients who had been on long-term modification of diet for medical reasons.
Finally, 46 men (aged 56 ± 18 years) and 23 women (aged 52 ± 7 years) with stroke were included in this study. Information on typical consumption of food and demographic and lifestyle characteristics was collected in the interview. The information also included age, sex, weight, and height. When patients were unable to answer, we asked for their next of kin to obtain answers.
We used a food frequency questionnaire (19) that included 168 items covering foods commonly consumed in Iran. The reference recall period was set at one year before the incidence of stroke. We obtained the quantity of minerals for each food item from the food composition table. We used the software of FPII to assay collected information and t-test for comparison between groups.
RESULTS
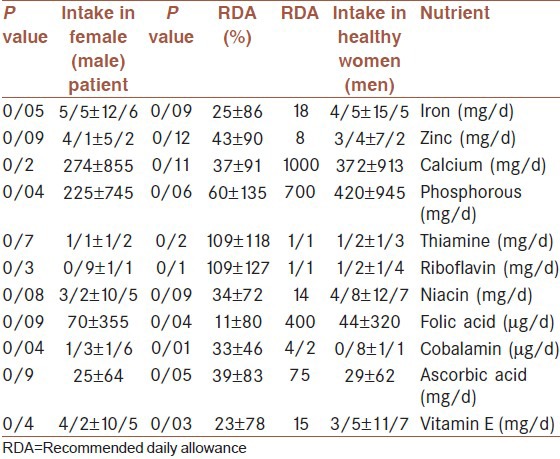
The study population consisted of 129 subjects, 69 patients with acute stroke, 46 men (aged 56 ± 18 years) and 23 women (aged 52 ± 7 years) and 60 controls (30 men and 30 women, 45 ± 5 years of age). The anthropometric measurements of the stroke subjects are reported in Table 1. Intake of energy and micronutrients in stroke subjects and controls are shown in Table 2. Intake of sodium in male and female patient with stroke was significantly higher than the control group. (P < 0.05, P < 0.001 in men and female respectively). Comparison of mean intake of vitamins and minerals in the study subjects with the recommended dietary allowance (RDA) are shown in Tables 3 and 4. In male patients, intake of iron was 21/5 ± 7/5 mg/day and in healthy men, intake of iron was 14/5 ± 8/5 mg/day, whereas RDA is 8 mg/day; therefore, intake of iron in the case group was significantly higher than the control group (P < 0/05), but intake of iron in case and control women was not significantly different. Intake of zinc in men with stroke was 17/2 ± 8/5 mg/day and in healthy men was 13/3 ± 7/3, and RDA for zinc was 11 mg/day; so, intake of zinc in men with stroke was significantly higher than healthy men (P < 0/05). But intake of zinc in women with stroke was 7/2 ± 3/4 mg/day and RDA is 8 mg/day, but intake of zinc in healthy women was 5/2 ± 4/1 mg/day; so, this difference was not significant. However, intake of calcium in male patients was 1352 ± 440 mg/day and RDA is 1000 mg/day; whereas intake of calcium in healthy men was 972 ± 335 mg/day; so, this difference was not significant. Intake of calcium in the two groups of women was also not significantly different.
Table 1.
Mean of anthropometric measurements in patients with stroke

Table 2.
Measurement of consumption of energy and micronutrients in stroke patients

Table 3.
Comparison of mean consumption of vitamins and minerals in male stroke patients and RDA
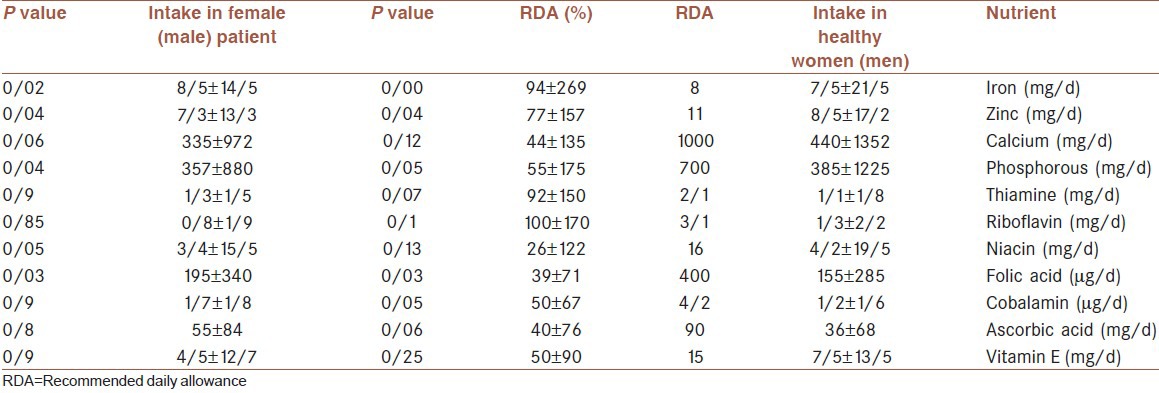
Table 4.
Comparison of mean consumption of vitamins and minerals in female stroke patients with RDA
DISCUSSION
In this study, we found that men and women with stroke had a diet higher in sodium, the positive association between the intake of sodium and stroke was independent of the intake of potassium, and this was observed similarly for nonoverweight and overweight persons. Findings from previous studies that have examined the relationship between the intake of sodium and risk of stroke have been inconsistent.[11] Our findings were supported by results of some previous studies; two studies of Americans[11,12] and Japanese[11,13] researchers reported that the intake of sodium was related to an increased risk of stroke and mortality and it was reported that about a daily intake of 100 mmol sodium maybe associated with 32% higher incidence of stroke among overweight Americans.[11,12] Japanese men with an intake of 306 mmol sodium had a twof old increased risk of stroke compared with people with a daily sodium intake of 174 mmol.[11,14] Mitsumasa et al. reported that a daily intake of 100 mmol sodium was related to 83% higher mortality from stroke. In addition, they found a strong positive association between intake of sodium and mortality from stroke for persons with either a body mass index (BMI) <25 or a BMI ≥ 25.[11]
Overweight may increase salt sensitivity for blood pressure.[11,15] However, Susana et al. reported that sodium was not significantly associated with risk of any stroke subtypes after potential confounders were controlled for.[15] A prospective study from Finland[16,17] and another from Japan[16,18] showed no significant association between intake of sodium and incidence of stroke. However, another Japanese study reported a significant association among men and women with a high intake of sodium (median daily intake of 7194 mg among men and 6478 mg among women).[16,19] In addition, the National Health and Nutrition Examination Survey epidemiologic follow-up reported a positive association among overweight persons.[16,20] High intake of sodium has been related to high blood pressure.[1,21] In this study, we reported that men with stroke had a high-iron diet and we supposed that high intake of iron can increase blood pressure as a main cause of stroke, but we did not find this result in women. In a previous study, researchers reported that increased intake of iron may elevate the risk of stroke.[1] They hypothesize that high intake of iron could increase the risk of atherosclerotic cardiovascular disease.[1,22] In contrast, a previous cross-sectional study involving four countries showed a significant inverse association between intake of iron and blood pressure,[1,23] whereas a recent study that was a randomized clinical trial did not observe any effect of reducing iron stores among phlebotomy on the risk of stroke and myocardial infraction after six years of intervention.[1,24] So, more investigation is needed to diagnose the effect of iron on risk of stroke. In our study, we observed no association between intake of calcium and stroke. Susanna et al. reported that intake of calcium was not significantly associated with risk of stroke after potential confounders were controlled for.[15] In addition, the Health Professionals Follow-up Study observed no association between intake of calcium and stroke.[25] The Nurses’ Health Study reported an inverse association between intake of calcium, especially dairy calcium, and risk of stroke.[26] Likewise, in a cohort of Japanese men and women, intake of dairy calcium was inversely associated with stroke mortality.[27] In a previous study that was a randomized trial including 36,282 postmenopausal women, intake of calcium and vitamin D supplementation neither decreased nor increased the risk of stroke over a seven-year period.[28] Intake of calcium was positively associated with the risk of intracerebral hemorrhage[2] in eight prospective studies of calcium intake in relation to stroke incidence or mortality;[29,30,31] four reported an inverse association between stroke and intake of dairy calcium but not nondairy calcium,[3,21,22,23] and no association was found for total intake of calcium from both dairy and nondairy foods.[5,13] The reason for the inconsistent results for the association of calcium intake with stroke maybe due to the difference in the range of exposure or the lack of adjustment for potential confounders.
CONCLUSION
In this study, a high intake of sodium was associated with a significantly increased risk of stroke and findings from this study did not report a protective effect of calcium on risk for stroke.
The limitations of the present study are first, the estimated intake of sodium from the present questionnaire study was ≈50% lower than that estimated from dietary records.[13] Second, we estimated intake of sodium with the food frequency questionnaire, whereas urinary measurement is a better tool than a food frequency questionnaire. Third, the diet was associated with a self-administered questionnaire that may have led to some errors in the measurement of dietary intake.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Liang W, Lee AH, Binns CW. Dietary Intake of Minerals and the Risk of Ischemic Stroke in Guangdong Province, China, 2007-2008. Prev Chronic Dis. 2011;8:A38. [PMC free article] [PubMed] [Google Scholar]
- 2.Mackay J, Mensah G. Geneva (CH): World Health Organization; 2004. Atlas of heart disease and stroke. [Google Scholar]
- 3.Meairs S, Wahlgren N, Dirnagl U, Lindvall O, Rothwell P, Baron JC, et al. Stroke research priorities for the next decade: A representative view of the European scientific community. Cerebrovasc Dis. 2006;22:75–82. doi: 10.1159/000093098. [DOI] [PubMed] [Google Scholar]
- 4.Liang W, Huang R, Lee AH, Hu D, Binns CW. Hospitalizations for incident stroke in Shunde District, Foshan, South China. Neuroepidemiology. 2008;30:101–4. doi: 10.1159/000120022. [DOI] [PubMed] [Google Scholar]
- 5.Susanna CL, Jarmo V, Alicja W. Potassium, calcium, and magnesium intakes and risk of stroke in women. Am J Epidemiol. 2011;174:35–43. doi: 10.1093/aje/kwr051. [DOI] [PubMed] [Google Scholar]
- 6.Ding EL, Mozaffarian D. Optimal dietary habits for the prevention of stroke. Semin Neurol. 2006;26:11–23. doi: 10.1055/s-2006-933305. [DOI] [PubMed] [Google Scholar]
- 7.Krauss RM, Eckel RH, Howard B, Appel LJ, Daniels SR, Deckelbaum RJ, et al. AHA dietary guidelines: Revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Stroke. 2000;31:2751–66. doi: 10.1161/01.str.31.11.2751. [DOI] [PubMed] [Google Scholar]
- 8.Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001;344:3–10. doi: 10.1056/NEJM200101043440101. [DOI] [PubMed] [Google Scholar]
- 9.Marniemi J, Alanen E, Impivaara O, Seppänen R, Hakala P, Rajala T, et al. Dietary and serum vitamins and minerals as predictors of myocardial infarction and stroke in elderly subjects. Nutr Metab Cardiovasc Dis. 2005;15:188–97. doi: 10.1016/j.numecd.2005.01.001. [DOI] [PubMed] [Google Scholar]
- 10.Umesawa M, Iso H, Date C, Yamamoto A, Toyoshima H, Watanabe Y, et al. Relations between dietary sodium and potassium intakes and mortality from cardiovascular disease: The Japan Collaborative Cohort Study for Evaluation of Cancer Risks. Am J Clin Nutr. 2008;88:195–202. doi: 10.1093/ajcn/88.1.195. [DOI] [PubMed] [Google Scholar]
- 11.Mitsumasa U, Hiroyasu I, Chigusa D, Akio Y, Hideaki T, Yoshiyuki W, et al. Relations between dietary sodium and potassium intakes and mortality from cardiovascular disease: The Japan Collaborative Cohort Study for Evaluation of Cancer Risks. Am J Clin Nutr. 2008;88:195–202. doi: 10.1093/ajcn/88.1.195. [DOI] [PubMed] [Google Scholar]
- 12.He J, Ogden LG, Vupputuri S, Bazzano LA, Loria C, Whelton PK. Dietary sodium intake and subsequent risk of cardiovascular disease in overweight adults. JAMA. 1999;282:2027–34. doi: 10.1001/jama.282.21.2027. [DOI] [PubMed] [Google Scholar]
- 13.Nagata C, Takatsuka N, Shimizu N, Shimizu H. Sodium intake and risk of death from stroke in Japanese men and women. Stroke. 2004;35:1543–7. doi: 10.1161/01.STR.0000130425.50441.b0. [DOI] [PubMed] [Google Scholar]
- 14.Rocchini AP, Key J, Bondie D, Chico R, Moorehead C, Katch V, et al. The effect of weight loss on the sensitivity of blood pressure to sodium in obese adolescents. N Engl J Med. 1989;321:580–5. doi: 10.1056/NEJM198908313210905. [DOI] [PubMed] [Google Scholar]
- 15.Susanna CL, Mikko JV, Monica M, Satu M, Pirjo P, Demetrius A, et al. Magnesium, Calcium, Potassium, and Sodium Intakes and Risk of Stroke in Male Smokers. Arch Intern Med. 2008;168:459–65. doi: 10.1001/archinte.168.5.459. [DOI] [PubMed] [Google Scholar]
- 16.Tuomilehto J, Jousilahti P, Rastenyte D, Moltchanov V, Tanskanen A, Pietinen P, et al. Urinary sodium excretion and cardiovascular mortality in Finland: A prospective study. Lancet. 2001;357:848–51. doi: 10.1016/S0140-6736(00)04199-4. [DOI] [PubMed] [Google Scholar]
- 17.Kagan A, Popper JS, Rhoads GG, Yano K. Dietary and other risk factors for stroke in Hawaiian Japanese men. Stroke. 1985;16:390–6. doi: 10.1161/01.str.16.3.390. [DOI] [PubMed] [Google Scholar]
- 18.Nagata C, Takatsuka N, Shimizu N, Shimizu H. Sodium intake and risk of death from stroke in Japanese men and women. Stroke. 2004;35:1543–7. doi: 10.1161/01.STR.0000130425.50441.b0. [DOI] [PubMed] [Google Scholar]
- 19.He J, Ogden LG, Vupputuri S, Bazzano LA, Loria C, Whelton PK. Dietary sodium intake and subsequent risk of cardiovascular disease in overweight adults. JAMA. 1999;282:2027–34. doi: 10.1001/jama.282.21.2027. [DOI] [PubMed] [Google Scholar]
- 20.Appel LJ, Brands MW, Daniels SR, Karanja N, Elmer PJ, Sacks FM. Dietary approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension. 2006;47:296–308. doi: 10.1161/01.HYP.0000202568.01167.B6. [DOI] [PubMed] [Google Scholar]
- 21.Sullivan JL. Iron and the sex difference in heart disease risk. Lancet. 1981;1:1293–4. doi: 10.1016/s0140-6736(81)92463-6. [DOI] [PubMed] [Google Scholar]
- 22.Tzoulaki I, Brown IJ, Chan Q, Van Horn L, Ueshima H, Zhao L, et al. Relation of iron and red meat intake to blood pressure: Cross-sectional epidemiological study. BMJ. 2008;337:a258. doi: 10.1136/bmj.a258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zacharski LR, Chow BK, Howes PS, Shamayeva G, Baron JA, Dalman RL, et al. Reduction of iron stores and cardiovascular outcomes in patients with peripheral arterial disease: A randomized controlled trial. JAMA. 2007;297:603–10. doi: 10.1001/jama.297.6.603. [DOI] [PubMed] [Google Scholar]
- 24.Ekblom k, Hultdin I, Stegmayr B, Johansson I, Van Guelpen B, Hallmans G, et al. Iron stores and HFE genotypes are not related to increased risk of ischemic strok. A prospective nested case-referent study. Cerebrovasc Dis. 2007;24(5):405–11. doi: 10.1159/000108429. [DOI] [PubMed] [Google Scholar]
- 25.Iso H, Stampfer MJ, Manson JE, Rexrode K, Hennekens CH, Colditz GA, et al. Prospective study of calcium, potassium, and magnesium intake and risk of stroke in women. Stroke. 1999;30:1772–9. doi: 10.1161/01.str.30.9.1772. [DOI] [PubMed] [Google Scholar]
- 26.Umesawa M, Iso H, Date C, Yamamoto A, Toyoshima H, Watanabe Y, et al. Dietary intake of calcium in relation to mortality from cardiovascular disease: The JACC Study. Stroke. 2006;37:20–6. doi: 10.1161/01.STR.0000195155.21143.38. [DOI] [PubMed] [Google Scholar]
- 27.Hsia J, Heiss G, Ren H, Allison M, Dolan NC, Greenland P, et al. Calcium/vitamin D supplementation and cardiovascular events. Circulation. 2007;115:846–54. doi: 10.1161/CIRCULATIONAHA.106.673491. [DOI] [PubMed] [Google Scholar]
- 28.Ascherio A, Rimm EB, Herna’n MA, et al. Intake of potassium, magnesium, calcium, and fiber and risk of stroke among US men. Circulation. 1998;98:1198–204. doi: 10.1161/01.cir.98.12.1198. [DOI] [PubMed] [Google Scholar]
- 29.Larsson SC, Virtanen MJ, Mars M, et al. Magnesium, calcium, potassium and sodium intake and risk of stroke in male smokers. Arch Intake Med. 2008;168(5):459–46. doi: 10.1001/archinte.168.5.459. [DOI] [PubMed] [Google Scholar]
- 30.Bergstro¨m L, Kylberg E, Hagman U, et al. The food composition database KOST: The National Administration's information system for nutritive values of food. Va°r Fo¨da. 1991;43:439–47. [Google Scholar]
- 31.Date C, Fukui M, Yamamoto A, Wakai K, Ozeki A, Motohashi Y, et al. Reproducibility and validity of a self-administered food frequency questionnaire used in JACC Study. J Epidemiol. 2005;15:S9–23. doi: 10.2188/jea.15.S9. [DOI] [PMC free article] [PubMed] [Google Scholar]