

Abstract
Background:
There are contrary results about the role of CACNA1A gene in the causation of common migraine in different populations. However, migraine may be genetically heterogeneous and more studies in different families and populations are required for a definite conclusion. The aim of this study was to surveyed leukocyte genomic DNA mutation of CACNA1A in Iranian migraine patients with [MA] and without aura [MO] who has family history of migraine and we performed a narrative review of all studies that evaluated CACNA1A gene, non-hemiplegic migraine [MA and MO] and FHM [familial hemiplegic migraine].
Materials and Methods:
The 30 patients with family history of migraine were selected for mutations analysis for CACNA1A gene by PCR method. For review, we searched MEDLINE-PUBMED, ISI, Scopus and Cochrane databases up to December 2012.
Results:
Mutation analysis of the 4 exons of the CACNA1A gene in these patients revealed no mutations in this gene. Direct sequencing revealed a polymorphism previously reported G to A transition in the exon 16 [nt2369, G→A] in 9 patients. In review, the correlation of FHM loci [CACNA1A gene] with MA and MO has been showed in different population and only small population from Caucasians presented this correlation.
Conclusion:
CACNA1A is most likely not a major susceptibility gene for common migraine in Iranian maigrainous. It's essential to study more on larger series and covering all 47 exons of the CACNA1A gene to confirm this hypothesis.
Keywords: CACNA1A gene, linkage, migraine, mutation
INTRODUCTION
Migraine is a prevalent neurological disturbance with the incidence of 16% of general population and impact roughly 20% of adults,[1,2,3,4] that involves women more than men by the percent of up to 12% of men and 24% of women in the general population.[5] Migraine without aura [MO] and migraine with aura [MA] in which headache is started with supplemen tary neurological symptoms, are two principal pattern of migraine disease.[6,7]
Studies on twin and family have substantiated that migraine comprises a main genetic component that MA has more than MO. The disease is genetically elaborate because many genes and environmental factors play a part in this disorder[5,7] and half of the patients have an affected first degree relative that it manifests the strong familial aggregation.[6]
Although some clinical heterogeneity are shown in the MA and MO subtypes, Mochi et al.[8] with segregation analysis proposed that there may be a common genetic etiology for MA and MO.[9]
Familiar hemiplegic migraine [FHM] is one of the most powerful congenital migraine sort of headache which is a rare autosomal dominantly inherited subtype of migraine with aura[5] that many studies revealed association this kind of migraine with mutations in the CACNA1A gene in different ethnic groups. Ophoff et al.[10] characterized the CACNA1A gene in preparation for a mutation search in neurologic disorders that map to 19p13. They found that the gene covers 300 kb with 47 exons.[11]
On the other hand, several reports[5,12,13] suggest the possible involvement of CACNA1A in non-hemiplegic migraine, but the other studies show contradictory results.[5,8,14,15]
Another studies showed the role of CACNA1A gene in the causation of common migraine,[12,13] however, some others in East Asia[16] did not show any correlation role. There is no study from Middle East and west of Asia to show the prevalence and correlation of this gene.
On the other hand migraine may genetically heterogeneous,[4] and more studies in different families and populations are required for a definite conclusion.
Therefore, the aim of this study was to surveyed leukocyte genomic DNA mutation of CACNA1A in Iranian migraine patients with and without aura who have family history of migraine.
MATERIALS AND METHODS
Patient selection
MA and MO subtype of migraine were detected by expert clinical neurologist, according to the International Headache Society criteria [Headache Classification Committee of the International Headache Society [IHS] [MA = criteria 1.2.1 and MO = criteria 1.1].[17]
Mutation analysis
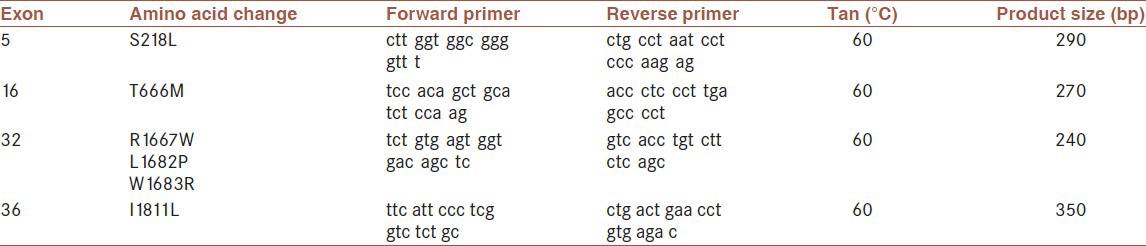
Then turning to genetic studies [found mutated in FHM[10] ] were studied in 30 patients who had family history of migraine with or without aura in first degree relatives. Genomic DNA was isolated from peripheral EDTA-treated blood cells by Qiagene DNA Mini kit [cat No: 51304]. DNA of each patient was subjected to PCR amplification of the Exon 5, 16, 32 and 36 of CACNA1A gene. Our study focused on 4 of the 47 exons of the CACNA1A gene. Exons 5, 16, 32 and 36 were studied because missense mutations [S218L, T666M, R1667W, L1682P, W1683R and I1811L, 2] have been found in FHM families.[10,18,19,20]
Twenty five-mL PCR reactions were carried out using 50 μL containing 100-200 ng total DNA from the patient, 10 pmol of each primers [Table 1], 2.5 mM MgCl2, 200 mM each of dNTP and 1 U Taq DNA polymerase [Roche Diagnostics, Mannheim, Germany]. The reaction mixture was amplified under following condition: 94°C for 30s, 60°C for 30s and 72°C for 45s for 35 cycles followed by one cycle of 72°C for 7 minutes, after initial denaturation 95°C for 6 minutes. The amplification products were detected on 2% agarose gel, run in 0.5X TBE at 110 V for 50 minutes and visualized under UV upon staining with 0.002 mg/mL ethidium bromide. Good quality PCR products were sequenced using the Big Dye Terminator sequencing kit [Applied Biosystems] and an ABI 3130 Genetic Analyzer [Applied Biosystems]. Sequence results were compared with the published sequence [GenBank no.X99897] by using Chromas and DNAMAN software. The primers sequences have been reported in Table 1.
Table 1.
Primer pair sequences are those used by ophoff et al.[10]
Review
Additionally, we performed a narrative review of all studies that evaluated CACNA1A gene, non-hemiplegic migraine [MA and MO] and FHM. Key words were classic migraine, migraine with aura, migraine without aura, common migraine and familial hemiplegic migraine and CACNA1A gene, gene mapping, gene screening and polymorphism. We searched MEDLINE-PUBMED, ISI, Scopus and Cochrane databases up to December 2012. We searched references lists from articles identified by search as well as a key review article to identify additional articles. We indentified case control, case series.
RESULT
Mutation analysis of the 4 exons of the CACNA1A gene in these patients revealed one polymorphism, but no mutations were identified in this gene. Direct sequencing revealed a polymorphism previously reported polymorphism[10,21] G to A transition in the exon 16 [nt2369, G→A] in 9 patients. In review, the correlation of FHM loci [CACNA1A gene] with MA and MO has been showed in different population and only small population from Caucasians presented this correlation.
DISCUSSION
In this study we found no CACNA1A gene mutations in Iranian patients. In accordance with our study, many researches had been reported such result. Table 2 showed all familial hemiplegic migraine [FHM] loci previously reported as candidate loci in migraine with typical aura [MA] and migraine without aura [MO] in different population. All of studies with linkage analysis [microsatellite marker in 19p13], mutations analysis on CACNA1A gene and related polymorphism were included in this table. Similar to our study, most of studies in western countries[9,14,22,23,24,25,26,27,28,29,30] and east of Asia[16] showed no correlation with FHM loci and MA and MO. Only a few studies in Netherlands and Finland[5,12] and a small subset of patients and families[31,32] explained this correlation. It appears the correlation of FHM loci with MA and MO is not depended to specific ethnic and only small population from Caucasians showed this correlation.
Table 2.
Familial hemiplegic migraine loci previously reported as candidate loci in migraine with typical aura and migraine without aura in different population
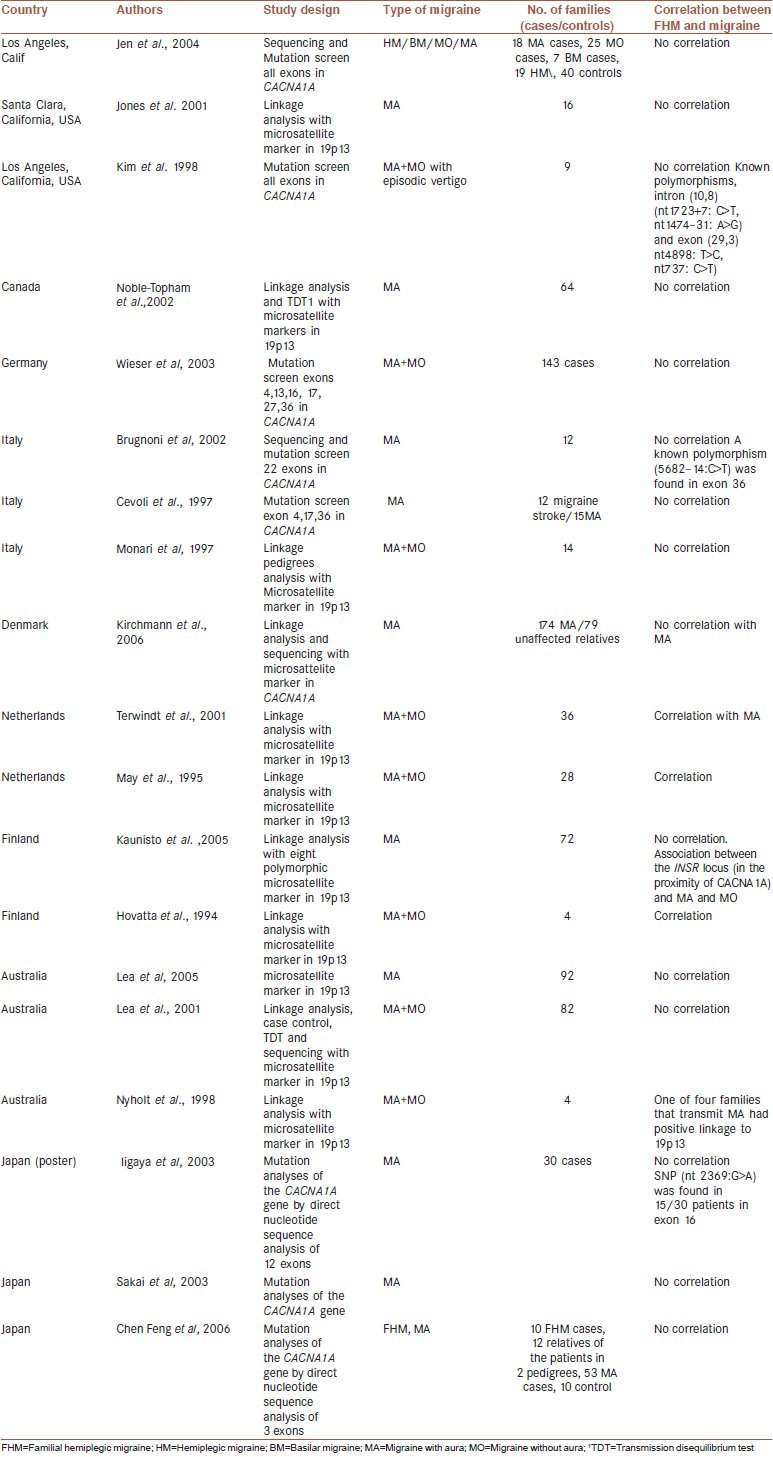
Hence, CACNA1A is not probable responsible gene for types of migraine. Other genes or loci that are involved are more suitable alternative genes for MA and MO migraine,[7] for example in a study it was found that a responsible gene for migraine was the insulin receptor gene INSR, which lies in a Chr19p13 region near CACNA1A. Five single-nucleotide polymorphisms within the insulin receptor gene were significantly associated with migraine. Five single-nucleotide polymorphisms within the insulin receptor gene were considerably related with migraine, but there are no practical outcomes of this polymorphism.[33]
However, it seems, there is possible limitation for unobtaining any mutation in the CACNA1A gene. At least 18 CACNA1A gene mutations in 47 exons have been identified in people with FHM1.[19,20] In our studies and some others[22] only limited mutations of FHM loci in limited exons were analyzed. Therefore, more studies with larger sample size and covering all 47 exons of the CACNA1A gene are necessary to confirm this hypothesis. We found a known polymorphism (nt 2369 G A) in exon 16 in 9 patients. Many studies identified other polymorphisms in the coding region of FHM loci in the patients with migraine, a number of them with significant difference[14,30,34] and some others without significant differences compare with control.[35,36]
CONCLUSION
As a result, CACNA1A is most likely not a major susceptibility gene for types of migraine in Iranian migraines. It is essential to study more on larger series of MA patients and covering all 47 exons of the CACNA1A gene to surely include or exclude whether migraine and FHM share common genetic defects.
ACKNOWLEDGMENT
This work was founded by Grant No. 290028 from the deputy for Research, University of Medical Sciences and Isfahan, Iran. We would like to thank.
Footnotes
Source of Support: This work was founded by Grant No. 290028 from the deputy for Research, University of Medical Sciences and Isfahan, Iran
Conflict of Interest: None declared.
REFERENCES
- 1.Sonbolestan SA, Heshmat K, Haghjooy Javanmard S, Saadatnia M. Efficacy of enelapril in migraine prophilaxis: A randomized, double blind, placebo-controlled trial. IJPM. 2013;4:72–7. [PMC free article] [PubMed] [Google Scholar]
- 2.Javanmard SH, Sonbolestan SA, Heshmat-Ghahdarijani K, Saadatnia M, Sonbolestan SA. Enalapril improves endothelial function in patients with migraine: A randomized, double-blind, placebo-controlled trial. J Res Med Sci. 2011;16:26–32. [PMC free article] [PubMed] [Google Scholar]
- 3.Saadatnia M, Zare M, Haghighi S, Tajmirriahi M, Hovsepian S. High frequency of IgM antiphospholipid antibodies in young Iranian patients with stroke. Neurosciences. 2007;12:124–6. [PubMed] [Google Scholar]
- 4.Gardner KL. Genetics of Migraine: An Update. Headache. 2006;46:S19–24. doi: 10.1111/j.1526-4610.2006.00486.x. [DOI] [PubMed] [Google Scholar]
- 5.Terwindt GM, Ophoff RA, van Eijk R, Vergouwe MN, Haan J, Frants RR, et al. Involvement of the CACNA1A gene containing region on 19p13 in migraine with and without aura. Neurology. 2001;56:1028–32. doi: 10.1212/wnl.56.8.1028. [DOI] [PubMed] [Google Scholar]
- 6.Jones KW, Ehm MG, Pericak-Vance MA, Haines JL, Boyd PR, Peroutka SJ. Migraine with Aura Susceptibility Locus on Chromosome 19p13 Is Distinct from the Familial Hemiplegic Migraine Locus. Genomics. 2001;78:150–4. doi: 10.1006/geno.2001.6665. [DOI] [PubMed] [Google Scholar]
- 7.de Vries B, Frants RR, Ferrari MD, van den Maagdenberg AM. Molecular genetics of migraine. Hum Genet. 2009;126:115–32. doi: 10.1007/s00439-009-0684-z. [DOI] [PubMed] [Google Scholar]
- 8.Mochi M, Sangiorgi S, Cortelli P, Carelli V, Scapoli C, Crisci M, et al. Testing models for genetic determination in migraine. Cephalalgia. 1993;13:389–94. doi: 10.1046/j.1468-2982.1993.1306389.x. [DOI] [PubMed] [Google Scholar]
- 9.Lea RA, Shepherd AG, Curtain RP, Nyholt DR, Quinlan S, Brimage PJ, et al. A typical migraine susceptibility region localizes to chromosome 1q31. Neurogenetics. 2002;1:17–22. doi: 10.1007/s10048-001-0125-1. [DOI] [PubMed] [Google Scholar]
- 10.Ophoff RA, Terwindt GM, Vergouwe MN, van Eijk R, Oefner PJ, Hoffman SM, et al. Familial Hemiplegic Migraine and Episodic Ataxia Type-2 Are Caused by Mutations in the Ca2+Channel Gene CACNL1A4. Cell. 1996;87:543–52. doi: 10.1016/s0092-8674(00)81373-2. [DOI] [PubMed] [Google Scholar]
- 11.Takahashi T, Igarashi S, Kimura T, Hozumi I, Kawachi I, Onodera O, et al. Japanese cases of familial hemiplegic migraine with cerebellar ataxia carrying a T666M mutation in the CACNA1A gene. J Neurol Neurosurg Psychiatry. 2002;72:675–80. doi: 10.1136/jnnp.72.5.676-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.May A, Ophoff RA, Terwindt GM, Urban C, van Eijk R, Haan J, et al. Familial hemiplegic migraine locus on 19p13 is involved in the common forms of migraine with and without aura. Hum Genet. 1995;5:604–8. doi: 10.1007/BF00197420. [DOI] [PubMed] [Google Scholar]
- 13.Hovatta I, Kallela M, Färkkilä M, Peltonen L. Familial Migraine: Exclusion of the Susceptibility Gene from the Reported Locus of Familial Hemiplegic Migraine on 19p. Genomics. 1994;23:707–9. doi: 10.1006/geno.1994.1563. [DOI] [PubMed] [Google Scholar]
- 14.Kim JS, Yue Q, Jen JC, Nelson SF, Baloh RW. Familial migraine with vertigo: No mutations found in CACNA1A. Am J Med Genet. 1998;79:148–51. doi: 10.1002/(sici)1096-8628(19980901)79:2<148::aid-ajmg11>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 15.von Brevern M, Ta N, Shankar A, Wiste A, Siegel A, Radtke A, et al. Migrainous Vertigo: Mutation Analysis of the Candidate Genes CACNA1A, ATP1A2, SCN1A, and CACNB4. Headache. 2006;46:1136–41. doi: 10.1111/j.1526-4610.2006.00504.x. [DOI] [PubMed] [Google Scholar]
- 16.Feng CH Y-nF, Hai-rong L, Xue-ji ng W. Association of CACNA1A gene polymorphism with familial hemiplegic migraine in southern Chinese. Chin J Clin Rehabil. 2006;10:170–2. [Google Scholar]
- 17.Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain. Cephalalgia. 1988;8:1–96. [PubMed] [Google Scholar]
- 18.Burgunder JM, Finsterer J, Szolnoki Z, Fontaine B, Baets J, Van Broeckhoven C, et al. EFNS guidelines on the molecular diagnosis of channelopathies, epilepsies, migraine, stroke, and dementias. Eur J Neurol. 2010;17:641–8. doi: 10.1111/j.1468-1331.2010.02985.x. [DOI] [PubMed] [Google Scholar]
- 19.De Vries B, Haan J, Frants RR, Van den Maagdenberg AM, Ferrari MD. Genetic Biomarkers for Migraine. Headache. 2006;46:1059–68. doi: 10.1111/j.1526-4610.2006.00499.x. [DOI] [PubMed] [Google Scholar]
- 20.Haan J, Kors EE, van den Maagdenberg AM, Vanmolkot KR, Terwindt GM, Frants RR, et al. Toward a molecular genetic classification of familial hemiplegic migraine. Curr Pain Headache Rep. 2004;3:238–43. doi: 10.1007/s11916-004-0058-0. [DOI] [PubMed] [Google Scholar]
- 21.Haan J, Kors EE, Terwindt GM, Vermeulen FL, Vergouwe MN, van den Maagdenberg AM, et al. Alternating hemiplegia of childhood: No mutations in the familial hemiplegic migraine CACNA1A gene. Cephalalgia. 2000;20:696–700. doi: 10.1046/j.0333-1024.2000.00095.x. [DOI] [PubMed] [Google Scholar]
- 22.Brugnoni R, Leone M, Rigamonti A, Moranduzzo E, Cornelio F, Mantegazza R, et al. Is the CACNA1A gene involved in familial migraine with aura? Neurol Sci. 2002;23:1–5. doi: 10.1007/s100720200015. [DOI] [PubMed] [Google Scholar]
- 23.Jen JC, Kim GW, Dudding KA, Baloh RW. No Mutations in CACNA1A and ATP1A2 in proban ds with common types of migraine. Arch Neurol. 2004;61:926–8. doi: 10.1001/archneur.61.6.926. [DOI] [PubMed] [Google Scholar]
- 24.Noble-Topham SE, Dyment DA, Cader MZ, Ganapathy R, Brown JD, Rice GP, et al. Migraine with aura is not linked to the FHM gene CACNA1A or the chromosomal region, 19p13. Neurology. 2002;7:1099–101. doi: 10.1212/wnl.59.7.1099. [DOI] [PubMed] [Google Scholar]
- 25.Wieser T, Mueller C, Evers S, Zierz S, Deufel T. Absence of known familial hemiplegic migraine [FHM] mutations in the CACNA1A gene in patients with common migraine: Implications for genetic testing. Clin Chem Lab Med. 2003;3:272–5. doi: 10.1515/CCLM.2003.042. [DOI] [PubMed] [Google Scholar]
- 26.Monari L, Mochi M, Valentino M, Arnaldi C, Cortelli P, Monte A, et al. Searching for migraine genes: Exclusion of 290 cM out of the whole human genome. Ital J Neurol Sci. 1997;18:277–82. doi: 10.1007/BF02083304. [DOI] [PubMed] [Google Scholar]
- 27.Kirchmann M, Thomsen LL, Olesen J. The CACNA1A and ATP1A2 genes are not involved in dominantly inherited migraine with aura. Am J Med Genet B Neuropsychiatr Genet. 2006;141B:250–6. doi: 10.1002/ajmg.b.30277. [DOI] [PubMed] [Google Scholar]
- 28.Kaunisto MA, Tikka PJ, Kallela M, Leal SM, Papp JC, Korhonen A, et al. Chromosome 19p13 loci in Finnish migraine with aura families. Am J Med Genet Part B Neuropsychiatr Genet. 2005;132B:85–9. doi: 10.1002/ajmg.b.30082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lea RA, Nyholt DR, Curtain RP, Ovcaric M, Sciascia R, Bellis C, et al. A genome-wide scan provides evidence for loci influencing a severe heritable form of common migraine. Neurogenetics. 2005;6:67–72. doi: 10.1007/s10048-005-0215-6. [DOI] [PubMed] [Google Scholar]
- 30.Cevoli S, Valentino MI, Mochi M. Molecular analysis on migraine patients: Exclusion of mutations in CACNA1A4 gene. Ital J Neurol Sci. 1997;4:59. [Google Scholar]
- 31.Nyholt DR, Lea RA, Goadsby PJ, Brimage PJ, Griffiths LR. Familial typical migraine: Linkage to chromosome 19p13 and evidence for genetic heterogeneity. Neurology. 1998;5:1428–32. doi: 10.1212/wnl.50.5.1428. [DOI] [PubMed] [Google Scholar]
- 32.Terwindt G, Kors EE, Haan J, Vermeulen F, van den Maagdenberg A, Frants R, et al. Mutation analysis of the CACNA1A calcium channel subunit gene in 27 patients with sporadic hemiplegic migraine. Arch Neurol. 2002;59:1016–8. doi: 10.1001/archneur.59.6.1016. [DOI] [PubMed] [Google Scholar]
- 33.McCarthy LC, Hosford DA, Riley JH, Bird MI, White NJ, Hewett DR, et al. Single-nucleotide polymorphism alleles in the insulin receptor gene are associated with typical migraine. Genomics. 2001;78:135–49. doi: 10.1006/geno.2001.6647. [DOI] [PubMed] [Google Scholar]
- 34.Yabe I, Sasaki H, Yamashita I, Tashiro K, Takei A, Suzuki Y, et al. Predisposing chromosome for spinocerebellar ataxia type 6 [SCA6] in Japanese. J Med Genet. 2001;38:328–33. doi: 10.1136/jmg.38.5.328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.D’Onofrio M, Ambrosini A, Di Mambro A, Arisi I, Santorelli FM, Grieco GS, et al. The interplay of two single nucleotide polymorphisms in the CACNA1A gene may contribute to migraine susceptibility. Neurosci Lett. 2009;453:12–5. doi: 10.1016/j.neulet.2009.01.081. [DOI] [PubMed] [Google Scholar]
- 36.Gerola S, Battistini S, Stenirri S, Nicolodi M, Arnetoli G, Canova S, et al. CACNA1A gene non-synonymous single nucleotide polymorphisms and common migraine in Italy: A case-control association study with a micro-array technology. Clin Chem Lab Med. 2009;6:783–5. doi: 10.1515/CCLM.2009.161. [DOI] [PubMed] [Google Scholar]