

Abstract
Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBL-LT) is a primary cutaneous B-cell lymphoma of intermediate behavior. The disease predominantly affects elderly patients. A 76-year old man presented with red to violaceous nodules in the anterior aspect of both tibias. Histology confirmed the diagnosis of PCDLBL-LT. A thorough clinical and laboratory investigation was negative for any systemic involvement. However, computed tomography of the thorax showed mediastinal lymphadenopathy. Both bone marrow aspiration and trephine did not show any evidence of bone marrow infiltration. Initially R-CHOP regimen (rituximab-cyclophosphamide, doxorubicin, vincristine, prednisone) achieved a total clearance of the lesions. Nevertheless, five months later patient presented with a relapse and was managed with palliative radiotherapy. The same treatment modality was applied for the second recurrence, as well. PCDLBL-LT affects mostly elderly patients. The consequent age related comorbidities and the frequent relapses require a strict follow up of the patients.
Keywords: B-cell cutaneous lymphoma, primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBL-LT), R-CHOP regimen
Introduction
Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) is one of the main types of primary cutaneous B-cell lymphoma with characteristic clinicopathological and immunohistochemical features1. It represents 1-4% of all cutaneous lymphomas2,3, approximately 10-20% of all PCBCLs2,3 and it seems that is increasing in frequency4.
Causative factors clearly related to the disease have not been found yet, but there is some speculation that it may represent a lymphoproliferative response to antigenic stimuli in the cutis3. Additionally, Human Herpes Virus (HHV)-6 and HHV-8 positivity in the neoplastic B-cells has been lately reported5. It has also been proposed that cutaneous B-cell lymphomas may arise from chronic stimulation of skin lymphoid tissue in response to Borrelia burgdorferi infection2,3.
The disease predominantly affects elderly patients (median age in the 70s), especially females, with the male to female ratio ranging from 1:2 to 1:43,6-8. Typically, patients present with rapidly growing, solitary or clustered, red or bluish-red nodules or tumors located on one or both legs, which can ulcerate7,9. However, in 10-20% of the patients, lesions arise at other body sites for the initial manifestation3,6,7. These lymphomas are mostly limited to the skin at presentation1. However, the most frequent extracutaneous sites that are spread are the lymph nodes, the bone marrow, and the central nervous system1,6. PCDLBCL-LT is an intermediate-grade B-cell lymphoma with 5-year survival rates ranging from only 41 % up to 73 %1-3,6,7,9. Therefore, appropriate treatment decisions are required.
We present an interesting case of PCDLBCL-LT, with multiple local relapses after first line chemotherapy and we discuss its management in the light of published data.
Description of case
A 76-year old man presented 24 months ago giving a 4-month history of gradually growing lesions, located on the distal extremity of both legs. The initial lesion involved the anterior aspect of his left lower leg and expanded gradually. The patient did not report any constitutional symptoms, such as fever, night sweats, weight loss or itching.
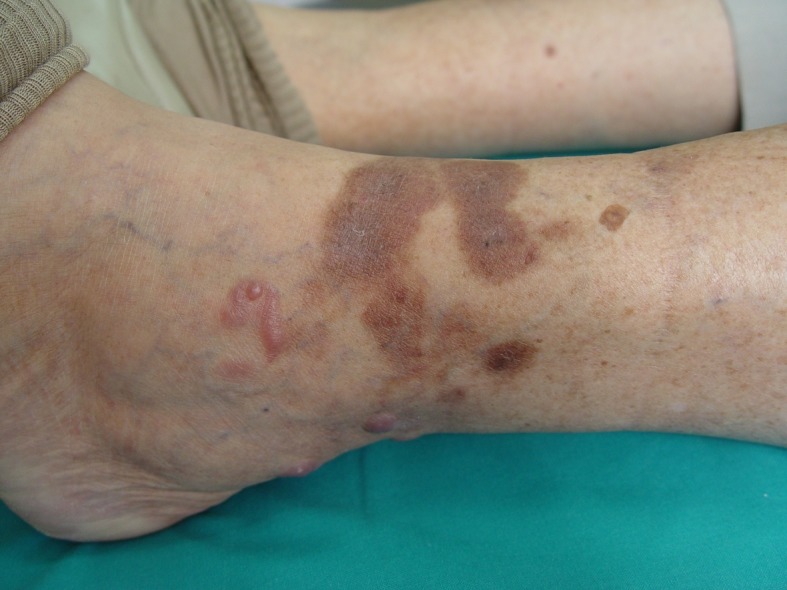
Physical examination showed slightly tender, erythematous, focally indurated plaques with irregular borders on the anterior aspect of both his lower legs, with multiple violaceous nodules on the surface of the plaques. The lesions on the left side were more extensive than those on the right side (Figure 1A). There were no palpable enlarged superficial lymph nodes.
Figure 1A. Multiple violaceous nodules on the left lower leg.

His past medical history included chronic atrial fibrillation, single-vessel coronary artery disease, diabetes mellitus type II and a recent syncoptic episode. Further down, an echocardiogram demonstrated impaired left ventricular function with an ejection fraction of 45%.
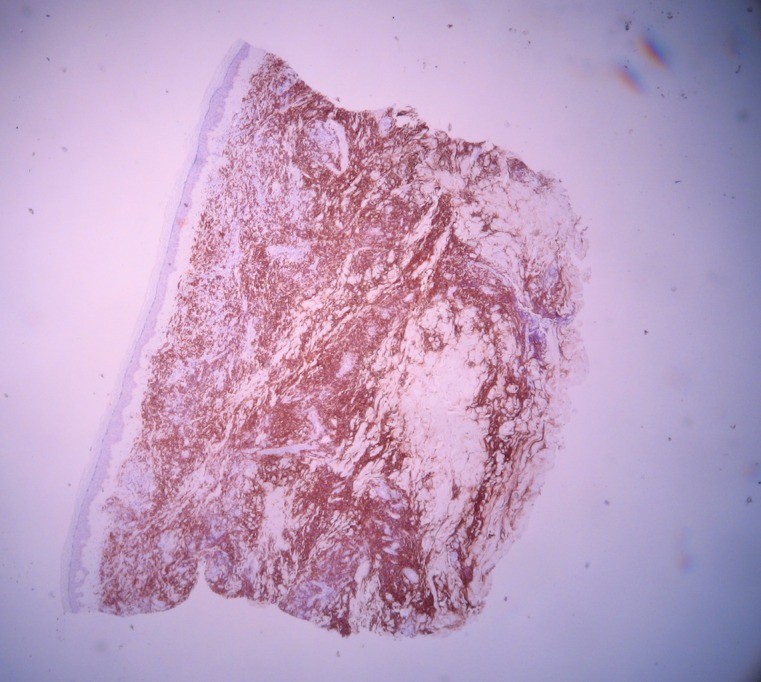
A skin biopsy of the lesion was performed. Histological findings revealed a dense infiltrate of large atypical lymphoid cells within the dermis and subcutaneous fat (Figure 2A). The infiltrate did not involve the papillary dermis. Most cells were large, non-cleaved centroblasts and immunoblasts and showed oval to round nuclei with prominent nucleoli. Mitotic figures were numerous. The epidermis appeared to be atrophic. Immunohistochemical stains showed that the infiltrating cells were strongly positive for CD20 (Figure 2B), Bcl-2 and partly positive for CD79a, confirming the B-cell phenotype of these cells. Reactive T-cell infiltrate was also observed. Based on these findings, the diagnosis of PCDLBCL-LT was made.
Figure 2A. A dense infiltrate of large atypical lymphoid cells within the dermis and subcutaneous fat (H&E stain, x 4).
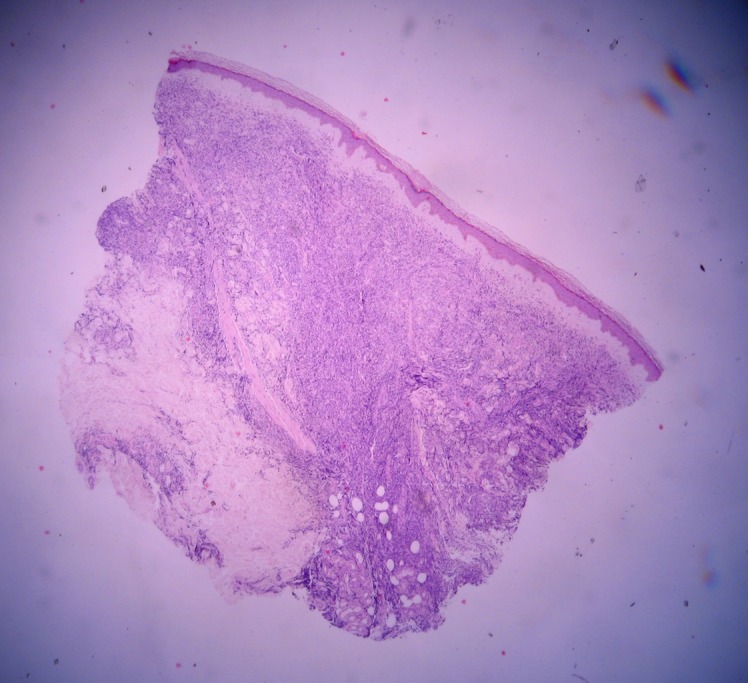
Figure 2B. Dense infiltrate, strongly positive for CD20 (CD20, x 4).
Complete work up examination for disease staging purpose was performed. Physical examination apart from the skin lesions in both lower extremities did not reveal any abnormality. There was neither palpable lymphadenopathy nor splenomegaly. However, computed tomography of the thorax, abdomen and pelvix did show mediastinal lymphadenopathy measuring approximately 3 cm in maximum diameter. Both bone marrow aspiration and trephine did not show any evidence of bone marrow infiltration.
Patient was treated with R-CHOP regimen along with dextrazoxane and GCSF support every 21 days. Dextrazoxane was used for cardiac protection due to patient’s borderline EF. He received six cycles of chemotherapy, which were delivered uneventfully with no major toxicities resulting to complete remission in both skin lesions and mediastinal lymph nodes. A Gallium scan performed two months after the end of the treatment confirmed his complete response.Only mild skin discoloration was observed at the sites where the initial lymphoma was located; a skin biopsy was performed which did not show any lymphoma infiltration. Patient was subsequently commenced on maintenance therapy with the monoclonal antibody rituximab at a dose of 375 mg/m2 every two months.
Nevertheless, five months after completion of chemotherapy he presented with multiple small nodules near the border of the previous tumors on his left lower leg ((Figure 1B)). Clinical, histological and immunohistochemical findings from the new lesions were identical to the previous ones. Imaging studies did not reveal any systemic disease. He had local palliative radiotherapy for his locoregional skin relapse along with rituximab which resulted to complete remission. The radiation therapy was applied in 10 sessions of 300cGy each (total 3000cGy). Five months later, the patient developed a second recurrence of the lymphoma on the left lower leg, which was histologically confirmed. There was no evidence of any other cutaneous or extracutaneous spread of the disease. Due to his concurrent comorbidities and the absence of disease elsewhere, he decided not to receive any palliative chemotherapy. However, he hadthe same radiotherapy scheme as previously in his new skin lesions. He had again complete response to his skin lesions and he is on maintenance rituximab every two months. A recent full imaging, 2 years since the initial diagnosis, did not demonstrate any recurrent disease and he is been regularly assessed in the outpatient clinic.
Figure 1B. New nodules at the periphery of the post radiation hyperpigmentation.
Discussion
Since PCDLBCLs-LT have poor prognosis, a more aggressive behavior and a worse outcome, due to frequent relapses and tendency to extracutaneous dissemination1-3,6,7,9, their timely diagnosis and treatment are of great importance.
The diagnosis is based on clinical, histologic and immunohistochemical data3,9, whereas essential for the diagnosis is the exclusion of a systemic non-Hodgkin diffuse large B-cell lymphoma at the time of initial diagnosis9. Histologically, this type of lymphoma shows a dense diffuse infiltrate of a monotonous population or confluent sheets of medium-sized to large B-cells with round nuclei, prominent nucleoli and coarse chromatin resembling centroblasts and/or immunoblasts within the dermis and subcutis. The neoplastic B-cells usually express B-cell markers (CD19, CD20, CD22, CD79a)1-3,7.Additionally, Bcl-21-3,7,9, MUM-1/IRF41-3,7,9, IgM2,7 and FOXP11,3 proteins are strongly positive. Furthermore, CD10 and CD138 are usually negative3, whereas clonal rearrangement of IgH genes can be detected in most cases7.
Due to the relative rarity of PCDLBCL-LT, there are no completed randomized trials to clarify the optimal treatment4. However, PCDLBCL-LT is recommended to be treated similarly to a systemic diffuse large B-cell lymphoma3,6. Therefore, the recommended frontline therapeutic approach is R-CHOP (rituximab- cyclophosphamide, doxorubicin, vincristine, prednisone) possibly accompanied by involved field radiation therapy2,3,6. Reported therapy options include radiotherapy, multiagent chemotherapy, chemotherapy, polychemotherapy with rituximab, and rituximab as single agent8. The first-line therapy for solitary tumor nodes is excision and radiotherapy, whereas for multifocal lesions and involvement of both legs polychemotherapy in combination with anti-CD20 antibodies (rituximab) or radioimmunotherapy are indicated7. It has also been reported that rituximab monotherapy for the treatment of PCDLBCL-LT induces an encouraging initial response, but with a relapse observed within a short time-period8. The response rate of rituximab monotherapy is lower than the response rate of rituximab with polychemotherapy8. However, the tolerance of rituximab monotherapy is higher than this of rituximab with polychemotherapy8. Therefore, rituximabmonotherapy may be appropriate in elderly patients unable to tolerate multiagent chemotherapy3.Additionally, a reduction in doses of R-CHOP can be made or less aggressive therapies are sometimes compulsory in cases of patient’s old age, presence of cardiopathy, poor general condition or presence of comorbidities9,10. In cases of recurrent disease, R-CHOP chemotherapy has proven to be effective, as well as chemotherapeutic compounds being applied for relapsing systemic B-cell non-Hodgkin lymphoma9. Moreover, radiotherapy or operation may be successfully applied in cases of relapsing PCDLBCL-LT9.
Our patient presented with mediastinal lymphadenopathy and was challenged with R-CHOP chemotherapy, as per common practice. It is interesting that he developed two local relapses in his skin disease treated with local radiotherapy and retuximab but so far, he has not progressed elsewhere. Salvage cytotoxic chemotherapy was not considered for his relapse because of his age and his comorbidities. Despite the avoidance of chemotherapy, rituximab and radiotherapy has managed to keep his skin disease under control and preserve his quality of life. Treatment choice in relapsed disease is difficult especially in older patients with compromised health. It is generally palliative in nature and should be always taken into consideration for decision making.
Regarding the old age of the majority of patients with primary cutaneous B-cell lymphoma leg type, the age related comorbidities and the number of relapses, treatment decisions remain quite difficult. In every case, a strict follow up of patients is considered a matter of high significance.
Conflict of interest
None declared.
References
- 1.Muniesa C, Pujol RM, Estrach MT, Gallardo F, García-Muret MP, Climent J, et al. Primary cutaneous diffuse large B-cell lymphoma, leg type and secondary cutaneous involvement by testicular B-cell lymphoma share identical clinicopathological and immunophenotypical features. J Am Acad Dermatol. 2012;66:650–654. doi: 10.1016/j.jaad.2011.03.031. [DOI] [PubMed] [Google Scholar]
- 2.Sokol L, Naghashpour M, Glass LF. Primary cutaneous B-cell lymphomas: recent advances in diagnosis and management. Cancer Control. 2012;19:236–244. doi: 10.1177/107327481201900308. [DOI] [PubMed] [Google Scholar]
- 3.Thomas V, Dobson R, Mennel R. Primary cutaneous large B-cell lymphoma, leg type. Proc (Bayl Univ Med Cent ) 2011;24:350–353. doi: 10.1080/08998280.2011.11928757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bessell EM, Humber CE, O’Connor S, English JS, Perkins W, Dickinson PD, et al. Primary cutaneous B cell lymphoma in Nottinghamshire U.K.: prognosis of sub-types defined in the WHO-EORTC classification. Br J Dermatol. 2012;167:1118–1123. doi: 10.1111/j.1365-2133.2012.11122.x. [DOI] [PubMed] [Google Scholar]
- 5.Nakayama-Ichiyama S, Yokote T, Iwaki K, Miyoshi T, Takubo T, Tsuji M, et al. Co-infection of human herpesvirus-6 and human herpesvirus-8 in primary cutaneous diffuse large B-cell lymphoma, leg type. Br J Haematol. 2011;155:514–516. doi: 10.1111/j.1365-2141.2011.08702.x. [DOI] [PubMed] [Google Scholar]
- 6.Hristov AC, et al. Primary cutaneous diffuse large B-cell lymphoma, leg type: diagnostic considerations. Arch Pathol Lab Med. 2012;136:876–881. doi: 10.5858/arpa.2012-0195-RA. [DOI] [PubMed] [Google Scholar]
- 7.Kempf W, Denisjuk N, Kerl K, Cozzio A, Sander C. Primary cutaneous B-cell lymphomas. J Dtsch Dermatol Ges. 2012;10:12–22. doi: 10.1111/j.1610-0387.2011.07852.x. [DOI] [PubMed] [Google Scholar]
- 8.Fenot M, Quereux G, Brocard A, Renaut JJ, Dreno B. Rituximab for primary cutaneous diffuse large B-cell lymphoma-leg type. Eur J Dermatol. 2010;20:753–757. doi: 10.1684/ejd.2010.1102. [DOI] [PubMed] [Google Scholar]
- 9.Wobser M, Kneitz H, Bröcker EB, Becker JP. Primary cutaneous diffuse large B-cell lymphoma, leg-type, treated with a modified R-CHOP immunochemotherapy - diagnostic and therapeutic challenges. J Dtsch Dermatol Ges. 2011;9:204–211. doi: 10.1111/j.1610-0387.2010.07578.x. [DOI] [PubMed] [Google Scholar]
- 10.Guyot A, Ortonne N, Valeyrie-Allanore L, Bagot M. Combined treatment with rituximab and anthracycline-containing chemotherapy for primary cutaneous large B-cell lymphomas, leg type, in elderly patients. Arch Dermatol. 2010;146:89–91. doi: 10.1001/archdermatol.2009.345. [DOI] [PubMed] [Google Scholar]