

Abstract
Objectives:
Rotator cuff tears are a common and disabling complaint. The early diagnosis of medium and large size rotator cuff tears can enhance the prognosis of the patient. The aim of this study was to identify clinical features with the strongest ability to accurately predict the presence of a medium, large or multitendon (MLM) rotator cuff tear in a primary care cohort.
Methods:
Participants were consecutively recruited from primary health care practices (n = 203). All participants underwent a standardized history and physical examination, followed by a standardized X-ray series and diagnostic ultrasound scan. Clinical features associated with the presence of a MLM rotator cuff tear were identified (P<0.200), a logistic multiple regression model was derived for identifying a MLM rotator cuff tear and thereafter diagnostic accuracy was calculated.
Results:
A MLM rotator cuff tear was identified in 24 participants (11.8%). Constant pain and a painful arc in abduction were the strongest predictors of a MLM tear (adjusted odds ratio 3.04 and 13.97 respectively). Combinations of ten history and physical examination variables demonstrated highest levels of sensitivity when five or fewer were positive [100%, 95% confidence interval (CI): 0.86–1.00; negative likelihood ratio: 0.00, 95% CI: 0.00–0.28], and highest specificity when eight or more were positive (0.91, 95% CI: 0.86–0.95; positive likelihood ratio 4.66, 95% CI: 2.34–8.74).
Discussion:
Combinations of patient history and physical examination findings were able to accurately detect the presence of a MLM rotator cuff tear. These findings may aid the primary care clinician in more efficient and accurate identification of rotator cuff tears that may require further investigation or orthopedic consultation.
Keywords: Sensitivity, Specificity, Physical examination, Primary health care, Rotator cuff
Introduction
Rotator cuff tears are a common cause of shoulder pain with a reported prevalence of 26% among primary care patients with symptomatic shoulder conditions.1 Rotator cuff tears can result in considerable pain, functional disability, reduced quality of life and loss of independence.2–4 They may also result in loss of productivity and high costs of associated work-related compensation for those unable to continue in high-demand occupations.
The size and location of a rotator cuff tear can influence decisions regarding management that may affect the patient’s prognosis considerably.5 While several classification systems for rotator cuff tear size have been proposed, most define a ‘small tear’ as being less than 10 mm in size, ‘medium’ tears 10–30 mm in size, and a ‘large’ or ‘massive’ tear as being more than 30 mm in size, or with involvement of two or more tendons.6–9 Large tears are associated with significant weakness and loss of function especially in younger patients,7,10,11 with a ‘large’ cuff tear identified as one of several prognostic determinants of a poor outcome of conservative management.5,12 Although the optimal timing for surgical intervention is a contentious issue, there is evidence that surgical repair of full thickness tears results in more favorable outcomes for pain, strength and function.13–15
Medium size rotator cuff tears are also of clinical significance, and identification of these lesions may affect decisions regarding use of diagnostic imaging and influence rehabilitation decisions within conservative management programs. Studies investigating the natural history of rotator cuff tears have shown that, in contrast to small tears with little or no tendon retraction that rarely progress in size,16 medium sized partial-thickness rotator cuff tears, particularly those involving the articular surface of the cuff, frequently increase in size over time.17 Medium-size partial thickness tears are also associated with a high rate of coexistent glenohumeral joint pathology, particularly in active populations.18 Clinical suspicion of a medium size, or partial thickness tear may therefore influence decisions regarding the use of additional imaging for investigation of coexistent pathology, and may alter exercise selection and loading progressions within conservative management programs to minimize loss of function associated with increasing tear size over time. Identification of a medium size rotator cuff tear may also influence decisions regarding the need for surgical intervention. Aggressive surgical repair of partial-thickness rotator cuff lesions in elite athletes or high-demand occupations, particularly in the presence of associated labral or other pathology has been advocated due to the unfavorable natural history of these conditions and favorable results of surgical procedures.19
In addition to the size of the tear, the timing of diagnosis is of prognostic importance. Both medium and large size rotator cuff tears frequently develop characteristic changes including fatty infiltration and muscle atrophy that have been observed as early as 2 weeks following injury in animal models.20 Medium sized, and partial thickness tears have demonstrated little ability to heal spontaneously and may continue to rupture following injury.21 Untreated full thickness tears have also shown a limited capacity to heal without surgical intervention,7,16 frequently resulting in retraction of tendon ends and superior migration of the humerus with narrowing of the acromiohumeral distance.22 Such changes render cuff tears irreparable due to the poor tissue quality and altered mechanics which frequently results in osteoarthrosis and poor functional outcomes.23 In primary health care the early diagnosis of a clinically significant medium or large rotator cuff tear, prior to loss of tissue viability is therefore important to inform decisions regarding conservative or surgical management and to optimize surgical outcomes.24,25
In primary care practice, the clinical diagnosis of rotator cuff tears begins with a clinical examination. The majority of previous studies have estimated the diagnostic accuracy of a small number of physical examination tests for identifying rotator cuff tears.26–31 Although ‘lag’ signs have shown consistently high levels of specificity (88–98%) for large rotator cuff tears in a number of studies,30–38 other physical examination tests have demonstrated variable diagnostic accuracy.39 However, many of these studies contained sources of bias and variation meaning care must be taken when generalizing results to different populations, and when interpreting the results of these studies.
Previous studies were conducted almost exclusively in secondary or tertiary (surgical) settings where the prevalence of MLM rotator cuff tears is reported to be 28–67.2%,28,29 considerably higher than the 14% reported in primary care settings.1 Prevalence is known to affect the generalization of diagnostic accuracy estimates, particularly predictive values, to other settings in which the prevalence of the condition differs.40 Whether the diagnostic accuracy estimates for physical examination tests from previous studies are similar in primary care populations has not been investigated to date.
Several studies contained sources of bias that may have resulted in overestimation of diagnostic accuracy values including differential verification bias,35 disease progression bias34 and use of an inappropriate reference standard.28 Many studies did not report sufficient detail regarding the study design,26,28–30,35,41 conduct,26,30,33,42 test interpretation or analysis 26,28–30,35,41 to allow assessment of the extent to which the potential sources of bias may affect interpretation of diagnostic accuracy results. Hence their results cannot be applied with confidence in primary care practice.
In addition, few studies have investigated other aspects of the clinical examination including history variables (e.g. night pain) and resisted tests as potential clinical predictors of MLM tears in primary care populations.28,30,31,43 Yet such questions and tests may provide important information that might enhance the ability of the primary care clinician to diagnose MLM rotator cuff tears.
Population differences, methodological concerns and lack of investigation of comprehensive clinical examination variables in previous studies mean the accuracy of the clinical diagnosis of MLM rotator cuff tears in primary care remains largely unknown. Therefore, the aim of this study was to estimate the diagnostic accuracy of a comprehensive spectrum of demographic, history and physical examination findings, and to identify clinical features with the strongest ability to accurately detect a MLM rotator cuff tear in a population of primary care patients with shoulder pain.
Methods
Participants
Participants were recruited from community-based medical and physiotherapy practices across Christchurch, New Zealand. Consecutive patients over the age of 18 years, presenting to their primary care practitioner (general practitioner or physiotherapist) for the first time with a new episode of shoulder pain and with the ability to follow verbal instructions, were eligible for inclusion in the study. Exclusion criteria were known fractures or dislocations around the shoulder complex, shoulder pain reproduced during clinical assessment of the cervical spine, sensory or motor deficit involving the upper limb, previous surgery to the shoulder or cervical spine, or contraindications to imaging or injection procedures. Following referral to the study, eligible patients were contacted by the research assistant to check the inclusion and exclusion criteria were satisfied and an appointment was made for the clinical examination. Sample size was estimated using methods for estimates for diagnostic accuracy studies described by Flahault et al.44 and details are provided elsewhere.1 Ethical approval was granted by the New Zealand Ministry of Health Regional Ethics Committee. All participants provided written informed consent prior to participation in the study.
Clinical examination
All clinical examinations were carried out in a dedicated research office in Christchurch, New Zealand. All participants completed self-report questionnaires consisting of the Shoulder Pain and Disability Index (SPADI),45 and the SF-8™ health survey (physical component and mental component scores).46 A modified Fear Avoidance Beliefs Questionnaire (FABQ)47 was also used in which the words ‘back pain’ were replaced with ‘shoulder pain’. Fear of pain has been associated with reduced shoulder function48 and also with persistent shoulder pain and disability.49 All participants then completed a standardized history questionnaire including pain drawing, pain intensity visual analogue scales, pain behavior, mechanism of onset, past history and medical history. Responses were checked for missing or ambiguous responses prior to the physical examination.
The physical examination was standardized for all participants and included measures of active and passive range of motion (ROM) and peak muscle force during resisted tests using a hand-held dynamometer.50 Pain responses to active and passive ROM tests were recorded according to whether they reproduced the participants’ symptoms using procedures described elsewhere.50 Peak muscle force50 and symptom responses were recorded during resisted abduction (in 10° abduction), external rotation and internal rotation (in 0° abduction). Orthopedic tests were performed according to original descriptions: Hawkins–Kennedy test,51 drop-arm test,52 empty can test,53 external rotation lag sign,35 belly-press test,32 Speed’s test,54 active-compression test,55 apprehension-relocation test,56 and pain responses to palpation of the shoulder region.57 All physical examinations were conducted by a clinician with 22 years’ experience (AC). A list of clinical examination variables and response criteria is presented in the Appendix. Indeterminate results of clinical examination tests were recorded and coded as missing data.
Diagnostic imaging
Following the clinical examination, an appointment was made at a specialist musculoskeletal imaging facility for X-ray and diagnostic ultrasound scan investigations. All participants underwent a standardized series of shoulder radiographs [anterior–posterior (AP) views in neutral, external and internal rotation, axial view and outlet view],58 followed by a diagnostic ultrasound scan performed by experienced musculoskeletal sonographers and reported by fellowship trained musculoskeletal radiologists. The diagnostic ultrasound procedure is described in detail elsewhere.1 Sonographers and radiologists recorded diagnostic information on a standardized worksheet that included recording pathological findings affecting the subacromial bursa, rotator cuff, long head of biceps tendon, acromioclavicular joint and whether a glenohumeral joint effusion was present. Rotator cuff tears were classified according to size (tear width and length in mm), location (intrasubstance, articular or bursal surface) and grade classification (high-grade, more than 50% of tendon thickness; low grade, less than 50% of tendon thickness; or full thickness tear including retraction). A ‘medium, large or multitendon’ (MLM) rotator cuff tear was defined as any tear exceeding 10mm (regardless of location or grade) or a tear affecting two or more tendons.6 Diagnostic ultrasound scans have a reported sensitivity and specificity exceeding 90% compared with surgery for medium and large size rotator cuff tears.59
Blinding
The clinician who performed the clinical examination was blinded to diagnostic imaging results and the sonographer and radiologist were blinded to results of the clinical examination.
Statistical methods
The Fisher exact test was used to assess the association between individual demographic, self-report and clinical examination variables with a MLM rotator cuff tear using the Statistical Package for the Social Sciences (SPSS) version 17.0 (IBM® Corporation 2010). Variables demonstrating univariate association with a rotator cuff tear at the P≤0.200 level were included in multiple logistic regression analyses and stepwise backward variable elimination was performed using Akaike’s Information Criterion60 to derive the strongest predictors of a MLM rotator cuff tear. Multiple regression analysis was undertaken using ‘R’ statistical software.61 The goodness of fit for the model was assessed using the Hosmer–Lemeshow test.62
Diagnostic accuracy statistics including sensitivity, specificity, predictive values, positive likelihood ratios (+LR) and negative likelihood ratios (−LR) and 95% confidence intervals (CI) were calculated for individual and combinations of clinical variables. The area under the receiver operator curve was assessed to find the optimal number of clinical tests for identifying a MLM rotator cuff tear. Confidence Interval Analysis software63 was used for calculation of diagnostic accuracy statistics.
Results
Three hundred and seventy three patients were referred to the study between July 2009 and June 2010 resulting in 208 subjects being included in the study. A total of 203 participants completed the clinical examination and diagnostic ultrasound scan (Fig. 1). There were no significant differences between those included and excluded from the study with respect to age or gender. Those excluded from the study reported shorter duration of symptoms (median 2 weeks; IQ range 4 weeks) (Mann–Whitney P<0.001). Demographic data for those who completed the study are presented in Table 1. Those for whom a MLM rotator cuff tear was identified were older, heavier, reported higher levels of pain, disability and fear avoidance beliefs, and had more coexisting medical conditions (P<0.05). The mean time between the clinical examination (index test) and diagnostic ultrasound scan (reference standard test) was 3.9 days (SD 2.6, range 1–19 days).
Figure 1.

Flow chart showing completion rate and dropout explanations.
Table 1. Participant characteristics.
| All cases (N = 203) | MLM tear (n = 24) | No MLM tear (n = 179) | ||
| Participant characteristics | Mean (SD) | Range | Mean (SD) | Mean (SD) |
| Age (years) | 42 (14) | 18–81 | 51 (13) | 41 (14)* |
| Height (cm) | 172 (10) | 147–199 | 173 (10) | 172 (10) |
| Weight (kg) | 80.6 (18.0) | 50.3–189.0 | 87.6 (26.3) | 79.6 (16.4)* |
| Symptom duration (weeks)† | 7 (13)* | 0–175 | 10 (11) | 13 (20) |
| VAS (worst) | 62 (23) | 3–100 | 68 (21) | 62 (23) |
| SPADI pain score (%) | 50 (22) | 0–100 | 59 (21) | 49 (21)* |
| SPADI disability score (%) | 30 (23) | 0–96 | 39 (24) | 29 (22)* |
| SPADI total (%) | 38 (21) | 0–98 | 47 (22) | 37 (21)* |
| FABQ physical activity score (%) | 64 (22) | 0–100 | 71(26) | 64 (22) |
| FABQ work score (%)‡ | 27 (23) | 0–81 | 35 (22) | 24 (23)* |
| FABQ total score (%)‡ | 41 (19) | 0–87 | 48 (21) | 38 (18)* |
| % male gender | 51 | 71 | 49 | |
| % right hand dominant | 87 | 50 | 53 | |
| % dominant arm affected | 53 | 46 | 54 | |
| % history of trauma | 21 | 67 | 34* | |
| % ACC claim | 93 | 100 | 92 | |
| % physiotherapist referrals | 98 | 100 | 97 | |
| Employment status | ||||
| % in paid employment | 80 | 83 | 80 | |
| % off work | 3 | 8 | 3 | |
| % co-existent medical conditions | 34 | 54 | 31* | |
| % smoker | 19 | 25 | 19 | |
Note: VAS, 100 mm visual analogue pain score in previous 48 hours; SPADI, Shoulder Pain and Disability Index; FABQ, Fear Avoidance Beliefs Questionnaire; ACC, Accident Compensation Corporation.
*Significant difference between groups P≤0.05.
†Variable not normally distributed; median (interquartile range) are presented.
‡Only cases ‘in paid employment’ used in analysis.
A MLM rotator cuff tear was identified on ultrasound in 24 participants (11.8%). Rotator cuff tear sizes and descriptions are presented in Table 2. Nineteen of 24 (79%) tears larger than 10 mm affected the supraspinatus component (Fig. 2). Large tears affecting more than one rotator cuff component were identified in four cases (Table 2). A description of other pathology identified on ultrasound in groups with, and without MLM rotator cuff tears is presented in Table 3. Those with a MLM rotator cuff tear were more likely to have coexisting subacromial bursal pathology (bursal thickening or effusion) (P≤0.001), a biceps tendon sheath effusion or long head of biceps tendon pathology (P≤0.01) than those without a MLM rotator cuff tear.
Table 2. Description of rotator cuff tears (N = 203).
| Tear size | Tear location (n) | n | % |
| No tear | 151 | 74.3 | |
| Small tear (<10 mm) | 28 | 14.3 | |
| Supraspinatus | 21 | 10.3 | |
| Intrasubstance (10) | |||
| Bursal surface — low grade (3) | |||
| Bursal surface — high grade (1) | |||
| Articular surface — low grade (4) | |||
| Articular surface — high grade (1) | |||
| Full thickness tears (3) | |||
| Infraspinatus | 1 | 1.0 | |
| Low grade (1) | |||
| Subscapularis | 6 | 3.4 | |
| Low grade (6) | |||
| Medium-large tear (≥10 mm) | 24 | 11.8 | |
| Supraspinatus | 19 | 9.4 | |
| Intrasubstance (8) | |||
| Articular surface — high grade (4) | |||
| Full thickness tear (7) | |||
| Infraspinatus | 2 | 1.0 | |
| Low grade (1) | |||
| Full thickness tear (1) | |||
| Subscapularis | 3 | 1.5 | |
| High grade (2) | |||
| Full thickness tear (1) | |||
| Multiple large tendon tears | 4 | 1.9 | |
| All three tendons (1) | 0.5 | ||
| Supraspinatus and infraspinatus (1) | 0.5 | ||
| Supraspinatus and subscapularis (2) | 1.0 | ||
Note: Tear size dimensions (mm) refer to transverse width. Low grade = less than 50% of vertical thickness is affected; high grade = more than 50% of vertical thickness is affected.
Figure 2.
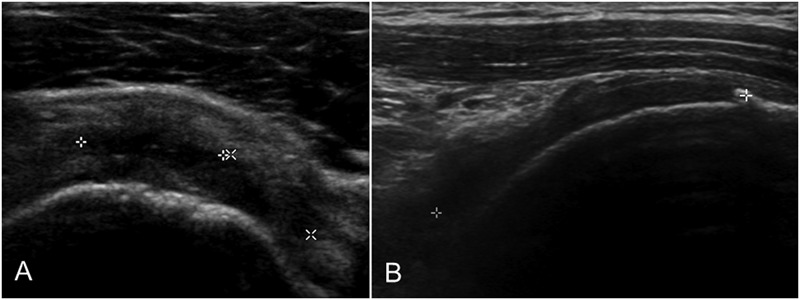
Rotator cuff tears identified on ultrasound. (A) High grade, articular surface supraspinatus tear (transverse view); (B) full thickness supraspinatus tear (longitudinal view).
Table 3. Distribution of other pathology in groups with and without MLM rotator cuff tears.
| Pathology identified on ultrasound | MLM tear (n = 24) | No MLM tear (n = 179 ) |
| % with pathology | % with pathology | |
| SAB pathology | 63 | 27*** |
| Dynamic bursal bunching | 74 | 58 |
| Rotator cuff tendinosis | 17 | 15 |
| supraspinatus | 13 | 14 |
| infraspinatus | 0 | 1 |
| subscapularis | 4 | 2 |
| Calcific tendinopathy | 21 | 25 |
| supraspinatus | 4 | 18 |
| infraspinatus | 4 | 5 |
| subscapularis | 21 | 8 |
| LHB pathology | 17 | 1** |
| Biceps tendon sheath effusion | 33 | 10** |
| GHJ effusion | 17 | 2 |
| ACJ pathology | 26 | 26 |
Note: MLM, medium, large or multitendon rotator cuff tear; SAB, subacromial bursa; LHB, long head of biceps; GHJ, glenohumeral joint; ACJ, acromioclavicular joint.
*P≤0.05; **P≤0.01; ***P≤0.001.
The clinical examination features that were associated with the presence of a MLM rotator cuff tear (P≤0.200) were age, SPADI pain subscale score, a traumatic mechanism of injury, night pain, reproduction of pain during resisted abduction or external rotation, symptom provocation during passive ROM external rotation (performed at 90° abduction), positive external rotation lag sign, a positive Speed’s test (Table 4), constant pain and painful arc in abduction (Table 5). Sensitivity ranged from 0.13 (external rotation lag sign) to 0.96 (Speed’s test) and specificity ranged from 0.22 (pain with resisted abduction or external rotation) to 0.97 (external rotation lag sign) (Table 4). The highest +LR (4.4) was observed for the external rotation lag sign (Table 4), and the lowest −LR (0.12) was observed for painful arc in abduction (Table 5). The Hawkins–Kennedy test and the empty can test were not associated with the presence of a MLM tear (P>0.200).
Table 4. Diagnostic accuracy of individual clinical examination variables for a MLM rotator cuff tear (N = 203).
| Clinical variables | Cell counts | Diagnostic accuracy | |||||||||
| TP | FN | FP | TN | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | +LR (95% CI) | −LR (95% CI) | OR (95% CI) | |
| Age >50 years | 12 | 12 | 50 | 129 | 0.50 (0.31, 0.69) | 0.72 (0.65, 0.78) | 0.19 (0.11, 0.31) | 0.92 (0.86, 0.95) | 1.79 (1.07, 2.70) | 0.69 (0.43, 0.97) | 2.58* (1.09, 6.12) |
| SPADI (pain >48%) | 17 | 7 | 97 | 81 | 0.71 (0.51, 0.85) | 0.46 (0.38, 0.53) | 0.15 (0.10, 0.23) | 0.92 (0.85, 0.96) | 1.30 (0.91, 1.66) | 0.64 (0.32, 1.12) | 2.03 (0.80, 5.13) |
| Traumatic onset | 16 | 8 | 61 | 118 | 0.67 (0.47, 0.82) | 0.66 (0.59, 0.73) | 0.21 (0.13, 0.31) | 0.94 (0.88, 0.97) | 1.96 (1.31, 2.67) | 0.51 (0.27, 0.82) | 3.87* (1.57, 9.55) |
| Night pain | 18 | 5 | 87 | 89 | 0.78 (0.58, 0.90) | 0.51 (0.44, 0.58) | 0.17 (0.11, 0.26) | 0.95 (0.88, 0.98) | 1.59 (1.15, 2.00) | 0.43 (0.19, 0.84) | 3.68* (1.31, 10.36) |
| Painful resisted abd or ER | 21 | 2 | 138 | 38 | 0.91 (0.73, 0.98) | 0.22 (0.17, 0.29) | 0.13 (0.09, 0.19) | 0.95 (0.84, 0.99) | 1.17 (0.93, 1.32) | 0.40 (0.11, 1.27) | 2.89 (0.65, 12.88) |
| Painful PROM ER(90o) | 22 | 2 | 130 | 46 | 0.92 (0.74, 0.98) | 0.27 (0.21, 0.34) | 0.14 (0.10, 0.21) | 0.96 (0.86, 0.99) | 1.25 (1.00, 1.42) | 0.31 (0.09, 1.00) | 3.89 (0.88, 17.20) |
| ERLS (positive) | 3 | 21 | 5 | 171 | 0.13 (0.04, 0.31) | 0.97 (0.94, 0.99) | 0.38 (0.14, 0.69) | 0.89 (0.84, 0.93) | 4.43 (1.20, 15.40) | 0.90 (0.71, 0.99) | 4.89 (1.09, 21.93) |
| Speed’s test (positive) | 22 | 1 | 109 | 64 | 0.96 (0.79, 0.99) | 0.37 (0.30, 0.44) | 0.17 (0.11, 0.24) | 0.99 (0.92, 1.00) | 1.51 (1.23, 1.74) | 0.12 (0.02, 0.58) | 12.92*** (1.70, 98.12) |
Note: TP, true positives; FN, false negatives; FP, false positives; TN, true negatives; PPV, positive predictive value; NPV, negative predictive value; +LR, positive likelihood ratio; −LR, negative likelihood ratio; OR, odds ratio; SPADI, Shoulder Pain and Disability Index; PROM, passive range of motion; abd, abduction; ER, external rotation; ERLS, external rotation lag sign.
Some cell counts do not total 203 due to missing data.
*P≤0.05; **P≤0.01; ***P≤0.001.
Table 5. Diagnostic accuracy of clinical examination prediction model variables for a MLM rotator cuff tear.
| Clinical variables | Cell counts | Diagnostic accuracy | ||||||||||
| TP | FN | FP | TN | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | +LR (95% CI) | −LR (95% CI) | OR (95% CI) | AOR (95% CI) | |
| All cases (n = 203) | ||||||||||||
| Constant pain | 13 | 11 | 50 | 129 | 0.54 (0.35, 0.72) | 0.72 (0.65, 0.78) | 0.21 (0.13, 0.32) | 0.92 (0.87, 0.96) | 1.95 (1.20, 2.88) | 0.64 (0.38, 0.91) | 3.05* (1.28, 7.26) | 3.04* (1.11, 8.30) |
| Painful arc abduction | 18 | 1 | 86 | 71 | 0.95 (0.75, 0.99) | 0.45 (0.37, 0.53) | 0.17 (0.11, 0.26) | 0.99 (0.93, 1.00) | 1.72 (1.34, 2.04) | 0.12 (0.02, 0.56) | 14.86*** (1.94, 114.06) | 13.97* (1.81, 108.82) |
| Both | 9 | 10 | 24 | 133 | 0.47 (0.27, 0.68) | 0.85 (0.78, 0.90) | 0.27 (0.15, 0.44) | 0.93 (0.88, 0.96) | 3.10 (1.62, 5.36) | 0.62 (0.37, 0.87) | 4.99** (1.84, 13.56) | |
| Age ≥50 years (n = 61) | ||||||||||||
| Constant pain | 5 | 7 | 16 | 33 | 0.42 (0.19, 0.68) | 0.67 (0.53, 0.79) | 0.24 (0.11, 0.45) | 0.83 (0.68, 0.91) | 1.28 (0.55, 2.53) | 0.87 (0.46, 1.31) | 1.52 (0.42, 5.53) | |
| Painful arc abduction | 9 | 0 | 22 | 16 | 1.00 (0.70, 1.00) | 0.42 (0.28, 0.58) | 0.29 (0.16, 0.47) | 1.00 (0.81, 1.00) | 1.73 (1.52, 2.37) | 0.00 (0.00, 0.74) | 0.71* (0.57, 0.89) | |
| Both | 3 | 6 | 6 | 32 | 0.33 (0.12, 0.65) | 0.84 (0.70, 0.93) | 0.33 (0.12, 0.65) | 0.84 (0.70, 0.93) | 2.11 (0.64, 6.07) | 0.79 (0.42, 1.12) | 2.67 (0.52, 13.71) | |
| Age <50 years (n = 142) | ||||||||||||
| Constant pain | 8 | 4 | 34 | 96 | 0.67 (0.39, 0.86) | 0.74 (0.66, 0.81) | 0.19 (0.10, 0.33) | 0.96 (0.90, 0.98) | 2.55 (1.41, 3.89) | 0.45 (0.19, 0.84) | 5.65 (1.60, 19.96)** | |
| Painful arc abduction | 9 | 1 | 65 | 55 | 0.90 (0.60, 0.98) | 0.46 (0.37, 0.55) | 0.12 (0.07, 0.22) | 0.98 (0.91, 1.00) | 1.66 (1.08, 2.07) | 0.22 (0.04, 0.90) | 7.62 (0.94, 62.0)* | |
| Both | 6 | 4 | 18 | 102 | 0.60 (0.31, 0.83) | 0.85 (0.78, 0.90) | 0.25 (0.12, 0.45) | 0.96 (0.91, 0.99) | 4.00 (1,87, 7.17) | 0.47 (0.20, 0.82) | 8.50 (2.18, 33.14)** | |
Notes: TP, true positives; FN, false negatives; FP, false positives; TN, true negatives; PPV, positive predictive value; NPV, negative predictive value; +LR, positive likelihood ratio; −LR, negative likelihood ratio; OR, odds ratio; AOR, adjusted odds ratio.
Cell counts may not total stated number due to missing data.
*P≤0.05; **P≤0.01; ***P≤0.001.
The constant nature of pain and a painful arc in abduction were the strongest predictors of a MLM rotator cuff tear (adjusted odds ratios: 3.04 and 13.97 respectively; 95% CI: 1.11–8.30 and 1.81–108.82 respectively) (Table 5). Of the two variables, a painful arc in abduction demonstrated the highest sensitivity (0.95) and the report of constant pain demonstrated highest specificity (0.72), with a +LR of 3.10 when both were positively identified (Table 5). Diagnostic accuracy, predictive values and likelihood ratios for constant pain and painful arc in abduction did not differ widely between older age groups (≥50 years) and younger age groups (<50 years) (Table 5).
Diagnostic accuracy results for combinations of all clinical examination variables are presented in Table 6. Highest sensitivity (1.00) was observed for up to five positive clinical examination findings and highest specificity (1.00) was observed when all 10 clinical examination findings were present. The highest +LR (infinity) was also observed for 10 clinical examination findings, and the lowest −LR was observed when fewer than five clinical examination findings were present. The area under the receiver operator curve curve was 0.838 (0.772, 0.905; P<0.001) and any combination of five positive clinical examination findings represented the optimal diagnostic point with sensitivity and specificity 0.88 and 0.66 respectively. A clinical summary of the diagnostic accuracy results is presented in Figure 3.
Table 6. Diagnostic accuracy for combinations of clinical variables for a MLM rotator cuff tear.
| Variable combinations | Cell counts | Diagnostic accuracy | |||||||||
| Number of positive clinical tests† | TP | FN | FP | TN | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | +LR (95% CI) | −LR (95% CI) | OR (95% CI) |
| 1 or more | 24 | 0 | 178 | 1 | 1.00 (0.86, 1.00) | 0.01 (0.00, 0.03) | 0.12 (0.08, 0.17) | 1.00 (0.21, 1.00) | 1.01 (1.00, 1.03) | 0.00 (0.00, 27.73) | 0.88 (0.84, 0.93) |
| 2 or more | 24 | 0 | 166 | 13 | 1.00 (0.86, 1.00) | 0.07 (0.04, 0.12) | 0.13 (0.09, 0.18) | 1.00 (0.77, 1.00) | 1.08 (1.07, 1.14) | 0.00 (0.00, 1.96) | 0.87 (0.83, 0.92) |
| 3 or more | 24 | 0 | 148 | 31 | 1.00 (0.86, 1.00) | 0.18 (0.13, 0.24) | 0.14 (0.10, 0.20) | 1.00 (0.89, 1.00) | 1.21 (1.18, 1.31) | 0.00 (0.00, 0.81) | 0.86* (0.81, 0.91) |
| 4 or more | 24 | 0 | 125 | 54 | 1.00 (0.86, 1.00) | 0.31 (0.24, 0.38) | 0.16 (0.11, 0.23) | 1.00 (0.94, 1.00) | 1.43 (1.36, 1.59) | 0.00 (0.00, 0.46) | 0.84*** (0.78, 0.90) |
| 5 or more | 24 | 0 | 90 | 89 | 1.00 (0.86, 1.00) | 0.50 (0.43, 0.57) | 0.21 (0.15, 0.29) | 1.00 (0.96, 1.00) | 1.99 (1.78, 2.32) | 0.00 (0.00, 0.28) | 0.79*** (0.72, 0.87) |
| 6 or more | 21 | 3 | 61 | 118 | 0.88 (0.69, 0.96) | 0.66 (0.59, 0.73) | 0.26 (0.17, 0.36) | 0.98 (0.93, 0.99) | 2.57 (1.91, 3.27) | 0.19 (0.07, 0.47) | 13.54*** (3.89, 47.20) |
| 7 or more | 15 | 9 | 35 | 144 | 0.63 (0.43, 0.79) | 0.81 (0.74 0.86) | 0.30 (0.19, 0.44) | 0.94 (0.89, 0.97) | 3.20 (2.08, 4.91) | 0.47 (0.28, 0.79) | 6.86*** (2.77, 16.95) |
| 8 or more | 10 | 14 | 16 | 163 | 0.42 (0.25, 0.61) | 0.91 (0.86, 0.95) | 0.39 (0.22, 0.58) | 0.92 (0.87, 0.95) | 4.66 (2.34, 8.74) | 0.64 (0.43, 0.83) | 7.28*** (2.79, 19.01) |
| 9 or more | 5 | 19 | 3 | 176 | 0.21 (0.09, 0.41) | 0.98 (0.95, 0.99) | 0.63 (0.31, 0.86) | 0.91 (0.85, 0.94) | 12.43 (3.40, 44.18) | 0.81 (0.61, 0.93) | 15.44*** (3.42, 69.72) |
| 10 | 2 | 22 | 0 | 179 | 0.08 (0.02, 0.26) | 1.00 (0.98, 1.00) | 1.00 (0.34, 1.00) | 0.89 (0.84, 0.93) | ∼ (1.78, 728.00) ‡ | 0.92 (0.79, 1.03) ‡ | 9.14* (6.16, 13.55) |
Note: TP, true positives; FN, false negatives; FP, false positives; TN, true negatives; PPV, positive predictive value; NPV, negative predictive value; +LR, positive likelihood ratio; −LR, negative likelihood ratio; OR, odds ratio; ∼, infinity.
Some cell counts do not total 203 due to missing data.
*P≤0.05; **P≤0.01; ***P≤0.001.
†Refers to combinations of clinical tests including any of: age >50 years, SPADI (pain) score >48%, traumatic onset, constant pain, night pain, painful arc abduction, pain with resisted abduction or external rotation, symptoms reproduced with passive external rotation (at 90° abduction), positive external rotation lag sign, positive Speed’s test
‡0.5 added to cells to estimate 95% CIs.
Figure 3.
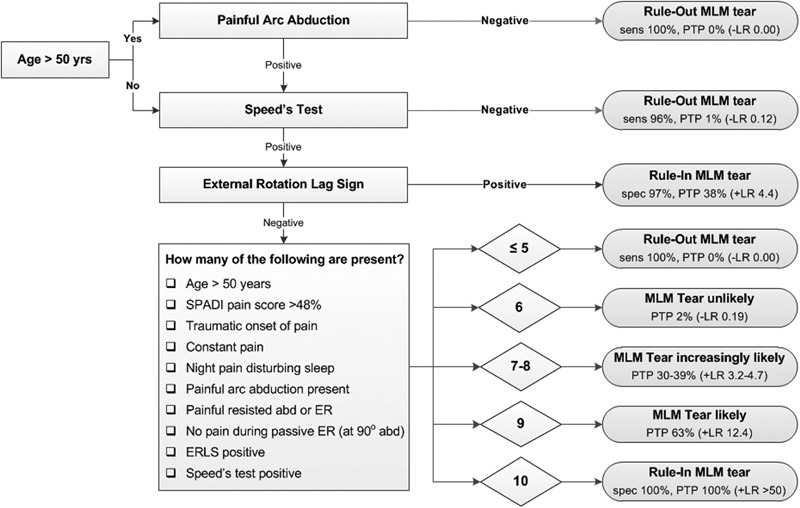
Flow chart showing diagnostic value of clinical tests for identifying a MLM rotator cuff tear.
Discussion
MLM rotator cuff tears are of diagnostic and prognostic significance with identification of these lesions influencing decisions regarding conservative or surgical management. The early identification of MLM rotator cuff tears at primary care level may improve patient outcomes by identifying those who require additional imaging investigations to evaluate rotator cuff integrity and associated pathology and who may require subsequent referral for surgical opinion. Early identification also facilitates optimal timing of surgery, leading to better structural integrity of tissues at the times of operation, and subsequently improved post-surgical outcomes.
Combinations of ten history and physical examination variables demonstrated the highest levels of diagnostic accuracy for identifying a MLM rotator cuff tear in this primary care study. When fewer than five of the 10 clinical features were present, the odds of a MLM rotator cuff tear were almost zero, and this lesion could be ruled-out with a moderate to high level of confidence (sensitivity 100%, lower confidence limit 0.86; −LR 0.00, upper confidence limit 0.28). Those with at least eight positive tests were almost five times more likely to have a significant rotator cuff tear (specificity 0.91, lower confidence limit 0.86), increasing to 12 times more likely when nine tests were positive (specificity: 0.98; lower confidence limit: 0.95; +LR: 12.4; 95% confidence limits: 3.40, 44.18). Ten positive tests resulted in 100% specificity and a +LR of infinity, however, only two participants satisfied this criterion resulting in a wide 95% CI for the +LR (1.78, 728.0). Appropriate care should therefore be taken when applying this result in clinical practice. These findings support previous reports of improved accuracy for rotator cuff pathology using combinations of clinical tests.28,30,31,42
The majority of previous diagnostic accuracy studies in this area involved patients recruited primarily from surgical waiting lists and investigated only a small number of predominantly physical examination tests, reporting variable accuracy findings.26,29,32,38,64 Only a limited number of studies estimated the diagnostic accuracy of patient history variables for identifying rotator cuff tears.28,30,65 Our results support findings from these studies in which older age and the presence of night pain were found to be strong predictors of a rotator cuff tear.28,30,65 In addition, our study identified several patient history variables (SPADI pain subscale score, traumatic mechanism of injury and constant nature of pain) and other physical examination findings (symptom provocation during resisted abduction or external rotation, and during passive external rotation) that, when combined, resulted in high levels of diagnostic accuracy for a medium or large rotator cuff tear.
The strongest predictors of a MLM rotator cuff tear in this primary care cohort were constant pain and a painful arc in abduction. Those patients who reported both constant pain and a painful arc in abduction were up to three times more likely to have a significant rotator cuff tear than those who did not report both these clinical features (+LR 3.10, lower confidence limit 1.62). A painful arc during active abduction has long been used in the diagnosis of ‘impingement’ syndromes, which includes rotator cuff tears66 and has also previously been identified as a strong predictor of supraspinatus tears.22,31,65 Although constant pain and a painful arc in abduction were identified as the two strongest predictors of a MLM rotator cuff tear, the post-test probabilities and likelihood ratios for combinations of the ten clinical examination features were able to more accurately identify the presence or absence of a MLM rotator cuff tear in individual patients than these two clinical predictor variables alone.
The specificity of individual clinical examination features for a MLM rotator cuff tear was variable (0.22–0.97). A number of other pathologies including subacromial bursa pathology were also identified on ultrasound in the group with a MLM rotator cuff tear and it is possible that provocation of symptoms from coexisting pathology may explain the lack of test specificity for a MLM rotator cuff tear in this cohort. Our results do support previous findings in which a positive external rotation lag sign was reported to be highly specific for a rotator cuff tear (94–100%)33,35,36 and, compared with a pre-test probability of 11.8%, a positive positive external rotation lag sign also demonstrated in the largest increase in post-test probability (38%) of all individual clinical tests.
Pain provocation during Speed’s test (resisted straight-arm raise), demonstrated the highest sensitivity (0.96) and lowest −LR (0.12) assisting to rule-out a significant rotator cuff tear with a moderate to high level of confidence when this test was negative. Speed’s test is reported to predominantly stress the long head of biceps tendon,67 however the complex anatomic relationship between the biceps tendon, rotator interval, subscapularis and supraspinatus tendons and association between anterior–superior rotator cuff tears and rotator interval injury68 mean injury to any of these structures may provoke pain during this test. This may explain the high sensitivity but low specificity of Speed’s test for a MLM rotator cuff tear. The absence of pain during resisted abduction or external rotation, and passive external rotation also demonstrated high sensitivity (>0.90); however, the −LR were modest (0.40 and 0.31 respectively) with the upper 95% confidence limit reaching 1.00, reducing confidence in the ability to rule-out a significant tear in the presence of a negative test.
In contrast to previous studies, the Hawkins–Kennedy test and empty-can test were not found to be associated with a MLM rotator cuff tear in this study. Although moderate to high levels of sensitivity have been reported for the Hawkins–Kennedy test by some authors (89–92%),29,42 closer inspection of these study results reveals that a negative Hawkins–Kennedy test resulted in only a small change (reduction) in post-test probability of a partial or full thickness rotator cuff tear from 28% (pre-test probability) to 11% (post-test probability) in one study,29 and resulted in negative predictive values of only 50% for Stage 2 impingement (including partial thickness tears) in the other study.42 No CIs were reported for estimates of diagnostic accuracy in either study, hence the findings of these studies should be interpreted with caution.
A negative empty can test has also been reported as sensitive for a supraspinatus tear (sensitivity 89–99%, negative predictive values 93–98%) in surgical settings using the same positive test criteria as defined in our study (pain or weakness).26,69 The diagnostic value of the empty can test for a rotator cuff (supraspinatus) tear is predicated on the belief that this test predominantly activates the supraspinatus muscle.53 However, recent work casts doubt on this assumption,53 reporting that infraspinatus, subscapularis, the upper, middle and lower fibers of trapezius, serratus anterior and all portions of the deltoid muscle were activated to a similarly high level as supraspinatus during the empty can test.70 The recruitment of large scapula muscles and the powerful deltoid muscle may compensate for a structurally compromised rotator cuff during the empty can test giving rise to false negative test results when muscle weakness is included in the test criteria. This may explain the lack of a relationship between a positive empty can test and the presence of a MLM rotator cuff tear in our study.
Effect of age on diagnostic accuracy
Increasing age has frequently been associated with the presence of rotator cuff tears in asymptomatic populations, becoming particularly prevalent in those over 50 years of age.71–73 In symptomatic populations, the frequency of rotator cuff tears has also been reported to increase after the age of 40 years.30 Results from the current study involving symptomatic participants also identified a relationship between increasing age and MLM cuff tears, with those over the age of 50 years being 2.5 times more likely to be diagnosed with a significant rotator cuff tear, although the lower confidence limit for the odds ratio only just exceeded 1.0 (1.09). Despite this finding, age alone was not able to predict the presence of a MLM tear in our study, and age was not retained in the multiple logistic regression model indicating that other clinical examination variables contributed more strongly to predicting the presence of a MLM tear in this cohort. In addition, aside from a small increase in post-test probability (positive predictive value) for a MLM tear from 17 to 29% in the older age group when a painful arc in abduction was reported, no other observable difference in post-test probabilities was identified between the older and younger age groups (Table 5). These results suggest that larger rotator cuff tears may be more prevalent in older age groups, however this does not imply a cause-and-effect relationship. In symptomatic primary care patients, older age alone (≥50 years) did not significantly increase the probability of a larger rotator cuff tear being present and other clinical features are likely to be of more diagnostic value for these lesions.
Limitations of the study
Limitations included the potential for diagnostic ultrasound to miss subtle partial-thickness articular surface rotator cuff tears. However, the aim of this study was to identify medium-large rotator cuff tears, and the sensitivity of diagnostic ultrasound for medium and large size tears has been reported to approach the sensitivity of MRI when performed by trained staff using modern equipment as was the case in this study.59,74
Conclusion
The prevalence of clinically significant rotator cuff tears in this group of primary care patients was low. However, when present, such lesions may warrant early referral for additional imaging to determine tear magnitude and associated pathology, or referral for orthopedic consultation. Combinations of patient history and physical examination findings were able to accurately identify the presence of a MLM rotator cuff tear. These findings may aid the clinician in more efficient and accurate identification of clinically significant rotator cuff tears and inform decisions regarding referral for further investigations or for surgical opinion.
Acknowledgments
We thank Dr Tony Young of Christchurch Radiology Group for support in-kind, Dr Mark Coates for radiological expertise and Mr Khalid Mohammed for his advice during the study. Thanks to Industrial Research Ltd for their technical support for the hand-held dynamometer. Funding support provided by the Health Research Council of New Zealand (Clinical Research Training Fellowship) (AC), New Zealand Manipulative Physiotherapists Association, Physiotherapy New Zealand and AUT University Faculty of Health and Environmental Science and the AUT University Short-Term Postdoctoral Fellowship (AC).
References
- 1.Cadogan A, Laslett M, Hing W, McNair P, Coates M. A prospective study of shoulder pain in primary care: Prevalence of imaged pathology and response to guided diagnostic blocks. BMC Musculoskelet Disord. 2011;12:119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Antonopoulou M, Alegakis A, Hadjipavlou A, Lionis C. Studying the association between musculoskeletal disorders, quality of life and mental health. A primary care pilot study in rural Crete, Greece. BMC Musculoskelet Disord. 2009;10(1):143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gartsman GM, Brinker MR, Khan M. Early effectiveness of arthroscopic repair for full-thickness tears of the rotator cuff. An outcome analysis. J Bone Joint Surg Am. 1998;80(1):33–40 [PubMed] [Google Scholar]
- 4.Ostor AJK, Richards CA, Prevost AT, Speed CA, Hazleman BL. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology. 2005;44:800–5 [DOI] [PubMed] [Google Scholar]
- 5.Bartolozzi A, Andreychik D, Ahmad S. Determinants of outcome in the treatment of rotator cuff disease. Clin Orthop Rel Res. 1994;308:90–7 [PubMed] [Google Scholar]
- 6.Bateman JE. The diagnosis and treatment of ruptures of the rotator cuff. Surg Clin North Am. 1963;43:1523–30 [DOI] [PubMed] [Google Scholar]
- 7.Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82(4):505–15 [DOI] [PubMed] [Google Scholar]
- 8.Patte D. Classification of rotator cuff lesions. Clin Orthop Rel Res. 1990;254:81–6 [PubMed] [Google Scholar]
- 9.Snyder SJ. Evaluation and treatment of the rotator cuff. Orthop Clin North Am. 1993;24(1):173–92 [PubMed] [Google Scholar]
- 10.Itoi E, Minagawa H, Sato T, Sato K, Tabata S. Isokinetic strength after tears of the supraspinatus tendon. J Bone Joint Surg Br. 1997;79(1):77–82 [DOI] [PubMed] [Google Scholar]
- 11.McCabe RA, Nicholas SJ, Montgomery KD, Finneran JJ, McHugh MP, McCabe RA, et al. The effect of rotator cuff tear size on shoulder strength and range of motion. J Orthop Sports Phys Ther. 2005;35(3):130–5 [DOI] [PubMed] [Google Scholar]
- 12.Neri BR, Chan KW, Kwon YW. Management of massive and irreparable rotator cuff tears. J Shoulder Elbow Surg. 2009;18(5):808–18 [DOI] [PubMed] [Google Scholar]
- 13.Burkhart SS, Barth JRH, Richards DP, Zlatkin MB, Larsen M. Arthroscopic repair of massive rotator cuff tears with stage 3 and 4 fatty degeneration. Arthroscopy. 2007;23(4):347–54 [DOI] [PubMed] [Google Scholar]
- 14.Lähteenmäki HE, Hiltunen A, Virolainen P, Nelimarkka O. Repair of full-thickness rotator cuff tears is recommended regardless of tear size and age: A retrospective study of 218 patients. J Shoulder Elbow Surg. 2007;16(5):586–90 [DOI] [PubMed] [Google Scholar]
- 15.Levy HJ, Gardner RD, Lemak LJ. Arthroscopic subacromial decompression in the treatment of full-thickness rotator cuff tears. Arthroscopy. 1991;7(1):8–13 [DOI] [PubMed] [Google Scholar]
- 16.Yamaguchi K, Tetro AM, Blam O, Evanoff BA, Teefey SA, Middleton WD. Natural history of asymptomatic rotator cuff tears: A longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg. 2001;10(3):199–203 [DOI] [PubMed] [Google Scholar]
- 17.Yamanaka K, Matsumoto T. The joint side tear of the rotator cuff. A followup study by arthrography. Clin Orthop Rel Res. 1994;304:68–73 [PubMed] [Google Scholar]
- 18.Walch G, Boileau P, Noel E, Donell ST. Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: an arthroscopic study. J Shoulder Elbow Surg. 1992;1(5):238–45 [DOI] [PubMed] [Google Scholar]
- 19.Matava MJ, Purcell DB, Rudzki JR. Partial-thickness rotator cuff tears. Am J Sports Med. 2005;33(9):1405–17 [DOI] [PubMed] [Google Scholar]
- 20.Rubino LJ, Stills HF, Jr, Sprott DC, Crosby LA. Fatty Infiltration of the Torn Rotator Cuff Worsens Over Time in a Rabbit Model. Arthroscopy. 2007;23(7):717–22 [DOI] [PubMed] [Google Scholar]
- 21.Hamada K, Tomonaga A, Gotoh M, Yamakawa H, Fukuda H. Intrinsic healing capacity and tearing process of torn supraspinatus tendons: In situ hybridization study of α1(I) procollagen mRNA. J Orthop Res. 1997;15(1):24–32 [DOI] [PubMed] [Google Scholar]
- 22.Moosikasuwan JB, Miller TT, Burke BJ. Rotator cuff tears: Clinical, radiographic, and US findings. Radiographics. 2005;25(6):1591–607 [DOI] [PubMed] [Google Scholar]
- 23.Gerber C, Wirth SH, Farshad M. Treatment options for massive rotator cuff tears. J Shoulder Elbow Surg. 2011;20(2):S20–9 [DOI] [PubMed] [Google Scholar]
- 24.Longo UG, Franceschi F, Berton A, Maffulli N, Droena V. Conservative treatment and rotator cuff tear progression. Med Sport Sci. 2012;57:90–9 [DOI] [PubMed] [Google Scholar]
- 25.Ruotolo C, Nottage WM. Surgical and nonsurgical management of rotator cuff tears. Arthroscopy. 2002;18(5):527–31 [DOI] [PubMed] [Google Scholar]
- 26.Itoi E, Kido T, Sano A, Urayama M, Sato K. Which is more useful, the full can test or the empty can test in detecting the torn supraspinatus tendon? Am J Sports Med. 1999;27(1):65–8 [DOI] [PubMed] [Google Scholar]
- 27.Leroux J, Thomas E, Bonnel F, Blotman F. Diagnostic value of clinical tests for shoulder impingement syndrome. Revue du Rhumatisme (Engl Ed). 1995;62:423–8 [PubMed] [Google Scholar]
- 28.Litaker D, Pioro M, El Bilbeisi H, Brems J. Returning to the bedside: using the history and physical examination to identify rotator cuff tears. J Am Geriatr Soc. 2000;48(12):1633–7 [DOI] [PubMed] [Google Scholar]
- 29.MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg. 2000;9(4):299–301 [DOI] [PubMed] [Google Scholar]
- 30.Murrell GAC, Walton J. Diagnosis of rotator cuff tears. Lancet. 2001;357(9258):769–70 [DOI] [PubMed] [Google Scholar]
- 31.Park HB, Yokota A, Gill HS, el Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 2005;87(7):1446–55 [DOI] [PubMed] [Google Scholar]
- 32.Barth JRH, Burkhart SS, de Beer JF. The Bear-Hug test: A new and sensitive test for diagnosing a subscapularis tear. Arthroscopy. 2006;22(10):1076–84 [DOI] [PubMed] [Google Scholar]
- 33.Castoldi F, Blonna D, Hertel R. External rotation lag sign revisited: Accuracy for diagnosis of full thickness supraspinatus tear. J Shoulder Elbow Surg. 2009;18(4):529–34 [DOI] [PubMed] [Google Scholar]
- 34.Gerber C, Hersche O, Farron A. Isolated rupture of the subscapularis tendon: results of operative repair. J Bone Joint Surg Am. 1996;78(7):1015–23 [DOI] [PubMed] [Google Scholar]
- 35.Hertel R, Ballmer FT, Lambert SM, Berber C. Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg. 1996;5(4):307–13 [DOI] [PubMed] [Google Scholar]
- 36.Miller CA, Forrester GA, Lewis JS. The validity of the lag signs in diagnosing full-thickness tears of the rotator cuff: a preliminary investigation. Arch Phys Med Rehab. 2008;89(6):1162–8 [DOI] [PubMed] [Google Scholar]
- 37.Scheibel M, Magosch P, Pritsch M, Lichtenberg S, Habermeyer P. The Belly-Off sign: a new clinical diagnostic sign for subscapularis lesions. Arthroscopy. 2005;21(10):1229–35 [DOI] [PubMed] [Google Scholar]
- 38.Walch G, Boulahia A, Calderone S, Robinson A. The ‘dropping’ and ‘hornblowers’ signs in evaluation of rotator cuff tears. J Bone Joint Surg Br. 1998;80(4):624–8 [DOI] [PubMed] [Google Scholar]
- 39.Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT, et al. Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests. Br J Sports Med. 2008;42:80–92 [DOI] [PubMed] [Google Scholar]
- 40.Leeflang MMG, Bossuyt PMM, Irwig L. Diagnostic test accuracy may vary with prevalence: Implications for evidence-based diagnosis. J Clin Epidemiol. 2009;62(1):5–12 [DOI] [PubMed] [Google Scholar]
- 41.Lyons AR, Tomlinson JE. Clinical diagnosis of tears of the rotator cuff. J Bone Joint Surg Br. 1992;74:414–5 [DOI] [PubMed] [Google Scholar]
- 42.Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis. 2000;59(1):44–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ebell MH. Diagnosing rotator cuff tears. Am Fam Physician. 2005;71(8):1587–8 [PubMed] [Google Scholar]
- 44.Flahault A, Cadilhac M, Thomas G. Sample size calculation should be performed for design accuracy in diagnostic test studies. J Clin Epidemiol. 2005;58(8):859–62 [DOI] [PubMed] [Google Scholar]
- 45.Roach KE, Budiman-Mak E, Songsiridej N, Lertratanakul Y. Development of a shoulder pain and disability index. Arthritis Care Res. 1991;4(4):143–9 [PubMed] [Google Scholar]
- 46.Ware JEJ, Kosinski M, Dewey JE, Gandek B. How to score and interpret single-item health status measures: a manual for users of the SF-8™ health survey. 3rd ed. Lincoln: QualityMetric Incorporated; 2001 [Google Scholar]
- 47.Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–68 [DOI] [PubMed] [Google Scholar]
- 48.Lentz TA, Barabas JA, Day T, Bishop MD, George SZ. The relationship of pain intensity, physical impairment, and pain-related fear to function in patients with shoulder pathology. J Orthop Sports Phys Ther. 2009;39(4):270–7 [DOI] [PubMed] [Google Scholar]
- 49.van der Windt DAWM, Kuijpers T, Jellema P, van der Heijden GJMG, Bouter LM. Do psychological factors predict outcome in both low-back pain and shoulder pain? Ann Rheum Dis. 2007;66(3):313–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Cadogan A, Laslett M, Hing W, McNair P, Williams M. Reliability of a new hand-held dynamometer in measuring shoulder range of motion and strength. Man Ther. 2011;16(1):97–101 [DOI] [PubMed] [Google Scholar]
- 51.Hawkins R, Kennedy J. Impingement syndrome in athletes. Am J Sports Med. 1980;8:151–8 [DOI] [PubMed] [Google Scholar]
- 52.Codman EA. Rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. In: Todd T, editor. The Shoulder Boston: T. Todd Company; 1934. p. 123–77 [Google Scholar]
- 53.Jobe F, Moynes D. Delineation of diagnostic criteria and a rehabilitation program for rotator cuff injuries. Am J Sports Med. 1982;10:336–9 [DOI] [PubMed] [Google Scholar]
- 54.Gill HS, El Rassi G, Bahk MS, Castillo RC, McFarland EG. Physical examination for partial tears of the biceps tendon. Am J Sports Med. 2007;35(8):1334–40 [DOI] [PubMed] [Google Scholar]
- 55.O'Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: A new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med. 1998;26(5):610–3 [DOI] [PubMed] [Google Scholar]
- 56.Jobe FW, Kvitne RS. Shoulder pain in the overhand or throwing athlete: The relationship of anterior instability and rotator cuff impingement. Orthop Rev. 1989;18(9):963–75 [PubMed] [Google Scholar]
- 57.Mattingly GE, Mackarey PJ. Optimal methods for shoulder tendon palpation: A cadaver study. Phys Ther. 1996;76(2):166–74 [DOI] [PubMed] [Google Scholar]
- 58.Anderson J, Read JW, Steinweg J. The shoulder and arm. In: Anderson J, Steinweg J, Read JW, editors. Atlas of imaging in sports medicine. 1st ed. Sydney, Australia: McGraw-Hill Book Company Australia Pty Limited; 1998. p. 96–129 [Google Scholar]
- 59.Fotiadou AN, Vlychou M, Papadopoulos P, Karataglis DS, Palladas P, Fezoulidis IV. Ultrasonography of symptomatic rotator cuff tears compared with MR imaging and surgery. Eur J Radiol. 2008;68(1):174–9 [DOI] [PubMed] [Google Scholar]
- 60.Akaike H. New look at the statistical model identification. IEEE Trans Automat Contr. 1974;19(6):716–23 [Google Scholar]
- 61. R Development Core Team. R: A language and environment for statistical computing. Version 2.12.0 ed. Vienna, Austria: R Foundation for Statistical Computing; 2010. [Google Scholar]
- 62.Hosmer DW, Lemeshow S. Applied logistic regression. 2nd ed. Shewhart W A, Wilks S S, editors. New York: Wiley; 2000 [Google Scholar]
- 63.Bryant TN. Confidence interval analysis. In: Altman DG, Machin D, Bryant TN, Gardner MJ, editors. Statistics with Confidence. 2.1.2 ed. Bristol: British Medical Journal Books; 2000 [Google Scholar]
- 64.Holtby R, Razmjou H. Validity of the supraspinatus test as a single clinical test in diagnosing patients with rotator cuff pathology. J Orthop Sports Phys Ther. 2004;34(4):194–200 [DOI] [PubMed] [Google Scholar]
- 65.Chew K, Pua YH, Chin J, Clarke M, Wong YS. Clinical predictors for the diagnosis of supraspinatus pathology. Physiother Singapore. 2004;13(2):12–7 [Google Scholar]
- 66.Cyriax JH. Textbook of Orthopaedic Medicine: Diagnosis of Soft Tissue Lesions. 7th ed. London: Bailliere Tindall; 1978 [Google Scholar]
- 67.Holtby R, Razmjou H. Accuracy of the Speed’s and Yergason’s tests in detecting biceps pathology and SLAP lesions: comparison with arthroscopic findings. Arthroscopy. 2004;20(3):231–6 [DOI] [PubMed] [Google Scholar]
- 68.Gaskill TR, Braun S, Millett PJ. The rotator interval: pathology and management. Arthroscopy. 2010;27(4):556–67 [DOI] [PubMed] [Google Scholar]
- 69.Kim E, Jeong HJ, Lee KW, Song JS. Interpreting positive signs of the supraspinatus test in screening for torn rotator cuff. Acta Med Okayama. 2006;60(4):223–8 [DOI] [PubMed] [Google Scholar]
- 70.Jobe CM. Posterior superior glenoid impingement: expanded spectrum. Arthroscopy. 1995;11(5):530–6 [DOI] [PubMed] [Google Scholar]
- 71.Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77:296–8 [PubMed] [Google Scholar]
- 72.Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995;77(1):10–5 [DOI] [PubMed] [Google Scholar]
- 73.Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg. 1999;8(4):296–9 [DOI] [PubMed] [Google Scholar]
- 74.Iannotti JP, Ciccone J, Buss DD, Visotsky JL, Mascha E, Cotman K, et al. Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. J Bone Joint Surg Am. 2005;87(6):1305–11 [DOI] [PubMed] [Google Scholar]