

Abstract
Transient visualization of a FDG avid abnormality in the lungs without any structural lesion is reported in a case of iatrogenic pulmonary microembolism
Keywords: FDG, Pulmonary embolism, latrogenic
Introduction
F-18 fluorodeoxy glucose (FDG) positron emission tomography/computed tomography (PET/CT) offers an effective diagnostic modality, especially in the field of oncology allowing metabolic and morphologic information to be acquired in a single examination session. For the correct interpretation of F-18 FDG PET/CT, it is crucial to have a clear understanding of the biodistribution of FDG, physiological variations in its distribution, and related medical and surgical histories of the patient.
Case Report
A 48-year-old female, under surveillance following surgery for gastric cancer was referred for control evaluation by the F-18 FDG PET/CT study. F-18 FDG PET/CT images demonstrated an area of increased FDG uptake in the right lung middle lobe parenchyma, without any structural abnormality on CT [Figure 1]. A repeat F-18 FDG PET/CT scan was performed after a brief interval of 4 days of the first study did not reveal any abnormality; the previously noted intense focus of FDG avidity having been completely resolved [Figure 2]; the latter suggesting the benign nature of the lung abnormality. On the basis of clinical presentation and imaging studies a final diagnosis of iatrogenic microembolism was made.
Figure 1.
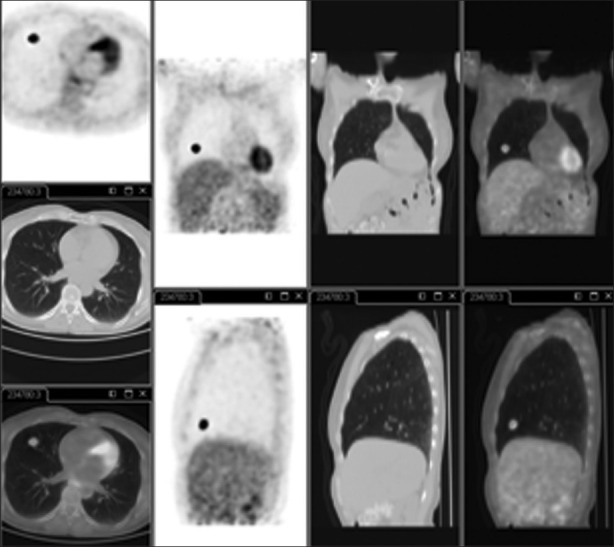
F-18 FDG PET/CT scan. Transaxial-, coronal-, and sagittal-section images of PET alone, CT alone and PET/CT fused images of the lungs show a discrete focus of increased uptake in the right lung middle lobe, without any structural abnormality on CT
Figure 2.
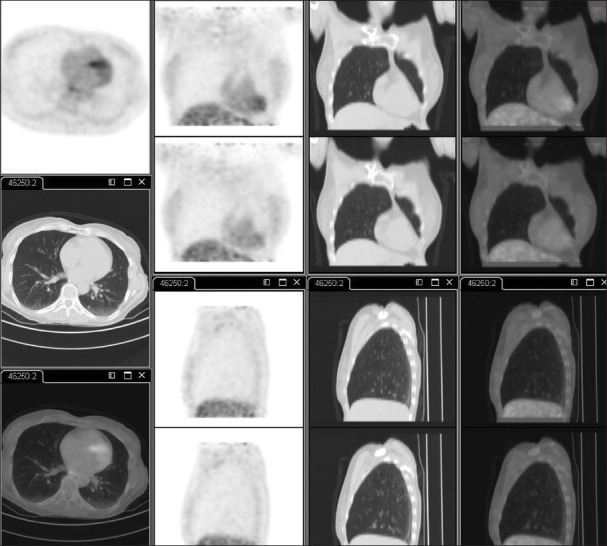
A control F-18 FDG PET/CT scan performed after 4 days of the first PET/CT. Transaxial-, coronal-, and sagittal-section images of PET alone, CT alone and PET/CT fused images of the lungs revealed complete resolution of the previously noted FDG avid focus. No other abnormalities were noted
Discussion
Pulmonary infection or inflammation might predispose patients to localized F-18 FDG lung uptake mimicking pulmonary metastases, thereby limiting the specificity of whole-body scans performed in patients with cancer. Normally, the FDG avid lesions are invariably accompanied by structural changes as evident on the CT scan. However, F-18 FDG foci without pathological CT are a rare finding and have been associated with inflammation and iatrogenic microembolism caused during injection. In the medical literature, two main causes have been identified which may give rise to such findings. These include uptake by a pre-existing inflammatory vascular thrombus or an iatrogenic microembolism formed during injection[1] of the radiotracer.
A few publications are available in the literature.[1–8] In all instances the FDG avid abnormalities have shown complete resolution in the follow-up studies. In most instances the follow-up scans were performed after a period of a few weeks to a few months. It is interesting to note that in our particular case the follow-up F-18 FDG PET/CT study was performed only after a brief interval of just 4 days of the initial scan; and we were able to document complete resolution of the FDG avid focus. This is probably the only instance where an acute episode of iatrogenic microembolism and its prompt resolution within a few days have been documented by an F-18 FDG PET/CT study. It is interesting to note that the follow-up scan did not reveal any structural abnormality like infiltration, consolidation, or atelectasis, which is normally associated with such episodes of infection or microembolization.
Conclusions
Pulmonary iatrogenic microembolism or inflammation might predispose patients to localized F-18 FDG uptake in the lungs without any associated structural lesion. Such abnormalities should be treated with caution. A follow-up scan after a period of few days or weeks may help in arriving at a diagnosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Conca DM, Brill DR, Shoop JD. Pulmonary radioactive microemboli following radionuclide venography. J Nucl Med. 1977;18:1140–1. [PubMed] [Google Scholar]
- 2.Schreiter N, Nogami M, Buchert R. Pulmonary FDG uptake without a CT counterpart: A pitfall in interpreting PET/CT images. Acta Radiol. 2011;52:513–5. doi: 10.1258/ar.2011.100448. [DOI] [PubMed] [Google Scholar]
- 3.Hany TF, Heuberger J, Schulthess GK. Iatrogenic FDG foci in the lungs: A pitfall of PET image interpretation. Eur Radiol. 2003;13:2122–7. doi: 10.1007/s00330-002-1681-y. [DOI] [PubMed] [Google Scholar]
- 4.Karantanis D, Subramaniam RM, Mullan BP, Peller PJ, Wiseman GA. Focal F-18 fluoro-deoxy-glucose accumulation in the lung parenchyma in the absence of CT abnormality in PET/CT. J Comput Assist Tomogr. 2007;31:800–5. doi: 10.1097/RCT.0b013e3180340376. [DOI] [PubMed] [Google Scholar]
- 5.Ha JM, Jeong SY, Seo YS, Kwon SY, Chong A, Oh JR, et al. Incidental focal F-18 FDG accumulation in lung parenchyma without abnormal CT findings. Ann Nucl Med. 2009;23:599–603. doi: 10.1007/s12149-009-0262-4. [DOI] [PubMed] [Google Scholar]
- 6.Mester U, Even-Sapir E. Increased (18) F-fluorodeoxyglucose uptake in benign, nonphysiologic lesions found on whole-body positron emission tomography/computed tomography (PET/CT): Accumulated data from four years of experience with PET/CT. Semin Nucl Med. 2007;37:206–22. doi: 10.1053/j.semnuclmed.2007.01.001. [DOI] [PubMed] [Google Scholar]
- 7.Eugene Lin, Abass Alavi. 2nd ed. Stuttgart, Germany: Thieme Publishers; 2009. PET and PET/CT: A Clinical Guide; pp. 53–4. [Google Scholar]
- 8.Fathinul Fikri A, Lau W. An intense 18F-FDG pulmonary microfocus on PET without detectable abnormality on CT: A manifestation of an iatrogenic FDG pulmonary embolus. Biomed Imaging Interv J. 2010;6:e37. doi: 10.2349/biij.6.4.e37. [DOI] [PMC free article] [PubMed] [Google Scholar]