

Abstract
Computed tomography enterography (CTE) has become a main modality for the evaluation of inflammatory bowel disease (IBD). It simultaneously offers visualization of the small bowel and extraintestinal status, which is helpful for diagnosing IBD. Crohn disease has long segmental enhancing wall thickening related with the eccentric longitudinal distribution. In addition, mural stratification, fibrofatty proliferation, positive comb sign by increased mesenteric vascularity and internal/perianal fistula are characteristics of Crohn disease and can be identified on CTE. Short segmental inflammatory wall thickening and the central low attenuated lymph nodes are favorable CT finding of intestinal tuberculosis. A geographic, relatively large, and deep penetrating ulcer with bowel wall thickening and mural hyperenhancement in ileocecal area are characteristics of intestinal Behcet disease. Each of CTE findings for the IBDs is helpful for differential diagnosis. The main disadvantage of this technique is the requisite radiation exposure of patients, particularly in young patients. However, recent development of advanced CT techniques is promising for radiation dose reduction without compromising diagnostic image quality.
Keywords: Computed tomography enterography, Inflammatory bowel diseases, Crohn disease, Intestinal tuberculosis, Behcet syndrome
INTRODUCTION
Computed tomography enterography (CTE) has been validated as an important imaging tool for small bowel evaluation over the recent years and has a clear established role as one of the primary diagnostic tools in the evaluation of patients with inflammatory bowel disease (IBD). CTE was first introduced by Raptopoulos et al.1 in 1997 as a modified abdominopelvic CT examination to specifically examine the small bowel, particularly to evaluate the extent and severity of Crohn disease.
This technique consists of luminal distention by large volume of neutral or low density oral contrast agent and optimized bowel wall enhancement by intravenously administered contrast agent to maximize conspicuity of small bowel pathology. Recently developed multidetector CT technique provides optimal multiplanar images by thin section scanning. Compared with endoscopic exams or barium studies, CTE has the ability to delineate both intestinal and extraintestinal pathology.
Therefore, CTE is a noninvasive examination that offers important and relevant information in the diagnosis and management of patients with proven or suspected IBD such as Crohn disease, intestinal tuberculosis (TB), and intestinal Behcet disease (BD). This article will provide a review of CTE with procedural technique and imaging findings of each IBD. In addition, it will describe recent advances in radiation dose reduction, which is important in the follow-up of patients with Crohn disease.
TECHNIQUE
Luminal distention by oral contrast agent
An adequate luminal distention is prerequisite for CTE. Optimized luminal distention provides rapid and efficient luminal navigation, accurate detection and characterization of small bowel abnormalities. Patients drink approximately 1.0 to 1.5 L of oral contrast over 45 to 60 minutes. There are various oral contrast agents to obtain the distention of small bowel loops.2 The negative contrast agent such as polyethylene glycol solution (PEG), suspension of 0.1% barium sulphate and water-methylcellulose solution is preferred because they allow better depiction of bowel wall enhancement. Water-methylcellulose solution has been gradually replaced by PEG or suspension of 0.1% barium sulphate. Our current protocol is summarized in Table 1.
Table 1.
Technique of Computed Tomography Enterography

PEG, polyethylene glycol; CT, computed tomography; HU, Hounsfield unit; PACS, picture archiving and communication system.
In CTE, oral contrast agent is administered by the oral route. However, contrast infusion through nasojejunal tube may be performed. The CT imaging after total opacification of the small bowel by such infusion is called as CT enteroclysis. Although the CT enteroclysis has better jejunal distention and higher specificity for detecting pathologic small bowel,2 there are unavoidable limitations such as patient's discomfort related with nasojejunal tube insertion and the increased radiation dose.3 Therefore, CTE has become a more preferred imaging technique for evaluating IBD because of the superior patient compliance and procedural convenience.
CT imaging protocol
CTE imaging protocol is as follows in our institute. It was performed using multidetector CT (Sensation-16 or Sensation-64; Siemens Medical Systems, Erlangen, Germany). Intravenous contrast material (120 to 150 mL) (Omnipaque 300 mg I/mL; Amersham Health Inc., Princeton, NJ, USA) was administered at a rate of 3 mL/sec. A bolus-tracking program was used to obtain singe enteric phase CT data after the intravenous injection of contrast agent. The region of interest cursor for bolus tracking was placed in the descending aorta at the level of the first lumbar vertebra for real time serial monitoring.
Acquisition of enteric phase images was commenced at 35 seconds after the trigger (trigger threshold level, 100 Hounsfield unit [HU]). Axial and coronal images were reconstructed and transferred to a picture archiving and communication system for image interpretation (slice thickness of 3 mm, and a reconstruction interval of 3.0 mm).
CTE FINDINGS OF CROHN DISEASE
Crohn disease, one of the major subtypes of the idiopathic IBD, is characterized by chronic, transmural, often granulomatous, intestinal inflammation. The small bowel is involved in almost 80% of the cases, with ileocecal region affected in 50%.4 Enteric involvement of Crohn disease tends to be transmural, segmental, and usually discontinuous. Multifocal small bowel disease may present with areas of different activity, some areas with acute inflammatory, and others with fibrostenosing disease.
As Crohn disease is a chronic and relapsing disease, multiple examinations are required to identify the status of the disease (e.g., the severity and activity), to evaluate the efficacy of current therapy and to modulate the therapeutic strategy. In that point, CTE can be an appropriate technique that can be easily performed, well tolerated for patients, be reliable in comparison of repeated exams as well as operator-independent. However, the effective dose of radiation from CT is relatively high compared with other modalities, and thus, patients with IBD can be exposed to significantly harmful amount of diagnostic radiation, mainly as a result of repeated CT examinations.
Active inflammatory disease
Crohn disease has a variety of appearances at CTE depending on whether the activity is acute inflammatory or chronic fibrostenosing and whether there are complications such as fistula or abscess. On CTE, enteric findings such as mural hyperenhancement, bowel wall thickening, mural stratification and extraenteric findings such as engorged vasa recta ("comb sign"),5 and increased attenuation of the mesenteric fat are features of active inflammatory small bowel Crohn disease.6,7
Among these findings, combination of mural hyperenhancement and bowel wall thickening is the most sensitive CTE findings suggesting the active inflammatory Crohn disease.7 While early studies suggested that bowel wall thickness correlated best with disease activity,7,8 more recent studies have suggested that mural hyperenhancement may be a more sensitive sign.9
Mural hyperenhancement refers to segmental hyperenhancement of the small bowel wall compared with the adjacent small bowel loops (Figs. 1, 2).7,9 It is important to compare the bowel loops with similar degree of distension because normal collapsed loops show greater attenuation than that of distended bowel loop. Quantitative measurement techniques have been used to objectively correlate mural hyperenhancement and bowel wall thickness with disease activity. Using a mural attenuation threshold of 109 HU and an abnormal to normal loop enhancement ratio of more than 1.3, CTE is highly correlated with histologic findings of active disease. Visual assessment, however, presents higher specificity than do quantitative measurements.9
Fig. 1.

Active inflammatory Crohn disease in a 28-year-old man. (A) Axial computed tomography enterography images demonstrate multifocal segmental mural hyperenhancement and trilaminar mural stratification in the ileum (arrows), suggesting active disease. (B) Also note engorged vasa recta (arrowheads) and increased attenuation of the mesenteric fat (asterisk).
Fig. 2.

Active inflammatory Crohn disease with extraenteric complications in a 29-year-old man. (A) Coronal computed tomography enterography images demonstrate multifocal segmental stricture showing wall thickening, mural hyperenhancement and stratification (arrows), and engorged vasa recta, "comb sign" (circle). (B, C) Also noted a mesenteric abscess (arrowheads in B) adjacent to the enteroenteric fistula (arrow in C).
Bowel wall thickening refers to wall thickness of greater than 3 mm in a distended bowel loop (Figs. 1-3). It is the most frequently observed CT finding in Crohn disease, presenting in up to 82% of patients.10
Fig. 3.

Crohn disease in a 31-year-old man. (A, B) Coronal computed tomography enterography images show pseudosacculation along the antimesenteric border of small bowel (arrowheads). (B) Fibrofatty proliferation is also demonstrated in the mesentery (circle). (C) Sinus tract arising in the terminal ileum (arrow) which shows mural hyperenhancement and stratification, suggesting active inflammatory disease, is also noted.
Mural stratification is visualization of the bowel wall layers on CT after intravenous contrast administration.6,7 Bilaminar mural stratification refers to mucosal hyperenhancement and decreased intramural attenuation. Trilaminar mural stratification refers to alternating areas of high and low attenuation due to mucosal and serosal hyperenhancement and low intramural attenuation (Figs. 1, 2). The low intramural attenuation can represent edema, inflammatory infiltrate, or fat. Mural stratification due to intramural edema is more indicative of active disease compared to a homogenously enhanced wall,8,11 while the presence of intramural fat indicates a more chronic process.6 One thing to notice is that mural stratification is not specific for Crohn disease and may be seen with other small bowel inflammatory conditions, such as ischemia, ulcerative colitis, and radiation enteritis.10
Increased attenuation of the mesenteric fat is due to edema and engorgement of the vasa recta (Fig. 1). The "comb sign" refers to engorged vasa recta that penetrate the bowel wall perpendicular to the bowel lumen, simulating the appearance of a comb (Fig. 2). Increased attenuation of the mesenteric fat in combination with the "comb" sign is the most specific CT finding for active Crohn disease.12 It correlates with clinically advanced, active, and extensive Crohn disease.5,11,12 The "comb sign" on CTE is also reported to be associated with higher C-reactive protein levels12 and more intensive medication regime than for patients with normal vasculature.11
Fibrostenosing disease
It is important to differentiate active inflammatory small bowel strictures from fibrotic strictures in patients with Crohn disease, because the former are mostly managed medically whereas the latter may require surgical intervention (e.g., balloon dilation, strictureplasty, or resection).3 CTE signs of chronic fibrostenosing disease are strictures without mural hyperenhancement or other signs of active inflammation, submucosal fat deposition, sacculations, and fibrofatty proliferation (Fig. 4).6,13
Fig. 4.

Fibrostenosing Crohn disease in a 32-year-old man. Axial computed tomography enterography image shows a segmental stricture involving proximal ileal loop. Homogenous mural thickening is seen at the strictured segment without mural hyperenhancement, suggesting fibrostenotic disease (arrow).
In fibrostenosing Crohn disease, mural stratification may be absent because of the transmural fibrosis and/or muscular hypertrophy and collagen deposition leading to a homogeneous and less-intense enhancement.10 Strictures may occur in patients with active inflammatory disease due to inflammation with edema and bowel spasm. However, strictures are more frequent with chronic fibrosis.14,15 Differential point is that a stricture in acute disease is manifested by mural hyperenhancement, more severe bowel wall thickening, and mural stratification. Submucosal fatty deposition in the bowel wall is also considered chronic changes of Crohn disease.6 However, active inflammation and fibrosis often coexist in the same patient or even in the same affected bowel segments in Crohn disease.
As the mesenteric border of bowel is preferentially affected by the inflammatory process of Crohn disease, the bowel loops often exhibit asymmetric mural fibrosis and shortening. Eventually, asymmetric fibrosis of the bowel loops combined with the increase in intraluminal pressure during the peristaltic movements results in sacculation of the antimesenteric wall (Fig. 3A).16
Fibrofatty proliferation has been long recognized as a hallmark of Crohn disease (Fig. 3B). It extends from the mesenteric attachment and partially covers the chronically inflamed bowel loop. Recent studies suggest that the hypertrophied mesenteric fat might have a role-related to the fat's capacity to produce tumor necrosis factor α-in sustaining the inflammatory process in Crohn disease.17
Extraenteric complications
The transmural inflammation of the bowel in Crohn disease coupled with increased intraluminal pressure proximal to the site of strictures can lead to extension of the inflammatory process across the serosal surface into the adjacent mesentery or structures. CTE has an important role in the evaluation of extraenteric complications of Crohn disease. The most common extraenteric complications include fistula, sinus tract, and abscess.15,18,19
Blind-ending inflammatory tracts form a sinus that can lead to a fistula if it communicates with another structure or fluid cavity. On CTE, sinus (Fig. 3C) or fistula (Figs. 2B, C, 5) are demonstrated as tethering of bowel loops and visualization of linear, enhancing tracts with or without communication with adjacent structures such as peritoneal or retroperitoneal spaces, skin or adjacent organs, or bowel, respectively.20 The most common type of fistula in Crohn disease is a perianal fistula (Fig. 5B). Other types of fistulas in Crohn disease include enterocutaneous, rectovaginal, enterovaginal, and enterovesicular fistulas.19 CTE has a high sensitivity for diagnosing fistulas. A recent study reported that CTE correctly identifies the presence or absence of fistulae in 94% of patients.15 The improved detection of fistulas by CTE compared to earlier studies likely reflects the improved spatial resolution due to thinner slice collimation and higher quality multiplanar images.
Fig. 5.

Crohn disease in a 34-year-old woman. (A) Axial computed tomography enterography image shows enteroenteric fistula involving ileal loops (arrow). (B) Perianal fistula is also seen (arrow).
Abscesses are easily detected by CTE which is usually contiguous to the diseased bowel segment and is seen in the mesentery or retroperitoneal space (Fig. 2).6 The accurate detection of abscesses and fistulas has high importance not only because it affects the decision to treat medically or surgically, but also it can affect the method of surgical approach (laparoscopic vs. open). A recent study by Bruining et al.21 showed that CTE affected on the physician's level of confidence for the findings of active small bowel disease, fistula, abscess, or stricture formation, which was altered in more than 90% of cases, with clinically significant changes in up to 77.6%. Booya et al.22 also reported detection of clinically unsuspected penetrating disease on CTE examinations, leading to alteration in therapy in up to 61% of patients with Crohn disease.
Other extraenteric manifestations of Crohn disease, such as mesenteric lymphadenopathy, cholelithiasis, nephrolitiasis, sacroiliitis, and primary sclerosing cholangitis, can also be evaluated.6
Treatment response evaluation
CTE can also be used to assess treatment response in Crohn disease, which manifests as decreasing mural hyperenhancement and bowel wall thickening, and improvement in the engorged vasa recta.8,23,24 Hara et al.8 observed that CTE interpretation of the disease progression or regression correlated with symptoms in 16/20 (80%) patients. Wu et al.23 reported that CTE findings have high correlation with clinical remission. According to their results, mural hyperenhancement and bowel wall thickening, the most sensitive signs of active disease, were decreased significantly after effective therapy, using a combination of clinical, endoscopic, pathologic, and laboratory findings as the criteria of disease remission. They also observed that the pattern of mural stratification changed with the trend from trilaminar or bilaminar stratification with mucosal hyperenhancement toward homogenous or bilaminar stratification without mucosal hyperenhancement. In addition, CTE can be used in evaluating postoperative recurrence of Crohn disease, which is most frequently seen at or immediately proximal to the anastomotic site.
CTE FINDINGS OF INTESTINAL TB
The diagnosis of intestinal TB remains a diagnostic challenge because it can mimic a lot of other disease entities, particularly Crohn disease. It is very difficult to differentiate intestinal TB from Crohn disease because they share similar clinical, pathological, and endoscopic findings.25 Although coexistence of pulmonary TB may be suggestive of small bowel TB, only 15% of cases of abdominal TB have evidence of pulmonary TB.26
Most frequent site of intestinal TB is ileocecal area (approximately 90% in case of gastrointestinal TB). CT may show circumferential wall thickening in the cecum and terminal ileum (Fig. 6). CT findings that may assist with the differentiation of intestinal TB from Crohn disease include short segmental inflammatory wall thickening related with the circumferential distribution of superficial ulcers (Fig. 7) in TB versus relatively long segmental wall thickening related with the eccentric longitudinal distribution of ulcers in Crohn disease. In addition, incompetence of ileocecal valve appears to be common in TB but uncommon in Crohn disease (Fig. 8). Mural stratification is known to be more frequent in Crohn disease.27
Fig. 6.

Intestinal tuberculosis in a 37-year-old woman. Coronal computed tomography enterography image shows circumferential wall thickening in the ileocecal valve area (arrow). Such ileocecal involvement is the most common form of intestinal tuberculosis.
Fig. 7.

Intestinal tuberculosis in a 52-year-old woman. Coronal computed tomography enterography image shows two short segmental circumferential enhancing wall thickenings involving proximal ileal loop (arrows). Associated prestenotic bowel dilatation is also seen.
Fig. 8.

Intestinal tuberculosis in a 27-year-old woman. Axial computed tomography enterography image shows enhanced wall thickening involving cecum and terminal ileum with patulous ileocecal valve (arrows). Associated central low attenuated lymph nodes are seen at the ileocecal mesentery, suggesting caseous necrosis (arrowheads).
Among extraintestinal findings, the central low attenuated lymph nodes, indicative of caseous necrosis, is a favorable CT finding of TB (Fig. 8). Fibrofatty proliferation, positive comb sign by increased mesenteric vascularity and internal/perianal fistula suggests the possibility of Crohn disease rather than intestinal TB. The CT findings for differential diagnosis between are summarized in Table 2. However, the differentiation between intestinal TB and Crohn disease may be difficult because they sometimes share similar radiologic findings (Fig. 9).
Table 2.
Differential Diagnosis of Tuberculosis from Cronh Disease
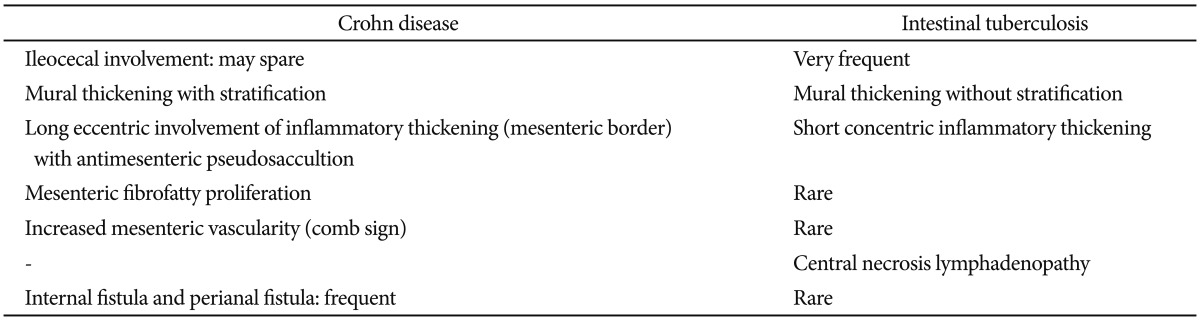
Fig. 9.

Crohn disease mimicking intestinal tuberculosis in a 53-year-old man. Relatively short segmental circumferential stricture is suspected in the distal ileal loop (arrow). Associated angulation is also seen. There is no remarkable finding in the mesentery. Preoperative computed tomography diagnosis was intestinal tuberculosis, but Crohn disease was confirmed after segmental resection of the small bowel loop.
CTE FINDINGS OF INTESTINAL BD
BD is characterized by the histopathologic finding of nonspecific vasculitis in multiple organs. The diagnosis is usually made on the basis of the combination of clinical signs and symptoms. It involves the gastrointestinal tract in 10% to 50% of patients.28 The most commonly involved site in the gastrointestinal tract is the ileocecal area.29,30 Intestinal BD is diagnosed by the presence of typical intestinal ulcers (a few round-shaped, deep ulcers with discrete margins in the ileocecal area) and systemic symptoms meeting the BD diagnostic criteria.30 The inflammation is transmural and extends to the serosa, manifested as the ulceration penetrating to the serosa or the fascia, with a tendency to irregularly undermine the tissue. On CTE, intestinal BD are commonly manifested as geographic, relatively large, and deep penetrating ulcer with bowel wall thickening and mural hyperenhancement in the ileocecal region (Figs. 9, 10). Occasionally, intestinal BD manifests as a cecal mass or an aneurysmal dilatation of the terminal ileum masquerading as a malignant tumor (Fig. 11).31,32 The undermining tendency of ulcers often results in bowel perforation and hemorrhage. CTE has advantages in the evaluation of extraluminal changes, contributing to early detection of complications such as perforation, fistula, hemorrhage, and peritonitis.31,32
Fig. 10.

Behcet disease in a 53-year-old woman. Axial computed tomography enterography image shows focal wall thickening with a deep penetrating ulcer (arrowheads) in the terminal ileum, and mesenteric fat infiltration around the ileocecal area.
Fig. 11.

Behcet disease in a 41-year-old man. (A, B) Axial computed tomography enterography images show wall thickening and several large, deep ulcers (arrowheads in A) in the terminal ileum with aneurysmal dilatation (asterisk in B).
In patients with intestinal BD, the frequency of postoperative recurrence ranges from 40% to 80%.33,34 There are three types of recurrence: the most common type consists of one or two deep ulcers, the second most common type is multiple aphthous ulcers, and the least common type is enterocutaneous fistula.33 Most recurrent ulcers occur at or near the anastomosis site (Fig. 12) and develop within 2 years after surgery.33 Considering the high frequency of postoperative recurrence and the common recurrence site at or near the anastomosis site, CTE may also have an important role in the detection of postoperative recurrence and the differentiation from postoperative complication.
Fig. 12.

Recurrent Behcet disease in a 30-year-old woman. Coronal computed tomography enterography image shows an ulceration with peripheral enhancement at the anastomosis site of ileocecectomy (arrows).
Radiation dose reduction issue
Radiation concern is an important issue in CTE because patients with Crohn disease are relatively younger and are expected to undergo multiple follow-up CT studies.35 Desmond et al.36 reported that portion of CT scans contributing to cumulative effective dose increased from 46.3% during the first 5 years to 84.7% during the final 5 years in their 15-year study of patients with IBD. This increase is likely due to the increased use of CT. In addition, a very recent study of Korean patients with IBD showed that 34.7% of patients with Crohn disease were exposed to harmful levels of radiation (cumulative effective dose >50 mSv) and CT accounted for 81.6% of total effective dose.37 Therefore, radiation dose reduction technique should be applied in CTE image acquisition protocol. Various techniques have been developed to reduce the radiation dose to the patient. First one is tube current (mA) modulation, which modulates the mAs based on the body thickness of each individual patient with sustaining diagnostic image quality.38 Second one is tube potential modulation (kV). Lowering tube potential is effective for dose reduction. In addition, lowering kV typically leads to an increase in iodine contrast, which may be helpful for detecting enhanced inflammatory bowel thickening. However, it allows more noise. Therefore, lower dose with constant image quality (contrast noise ratio) is essential in application of lowering tube potential.39 New image reconstruction technique such as iterative reconstruction enables the noise reduction using CT projection data in the lowering kV setting. Kaza et al.40 reported that CTE at 80 kVp with iterative reconstruction can produce diagnostically acceptable image quality with effective dose, 4.6 mSV, while the effective dose of routine CTE at 120 kVp was 15.8 mSV. There are more important dose reduction strategies apart from these advanced technologies. One is to minimize the number of dynamic CT phases. Wold et al.41 reported that arterial phase imaging is not contributory for detection of active Crohn disease. Single-phase imaging at CTE is sufficient in most cases of evaluation of Crohn disease (Fig. 13).
Fig. 13.

Radiation dose reduction by application of advanced techniques and computed tomography (CT) protocol optimization. Total dose-length product (DLP) was 861 mGycm in CT enterography (CTE) obtained in 2011 (upper row). Follow-up CTE was taken in the same patient with Crohn disease in 2013. Total DLP was remarkably decreased as 186 mGycm (lower row). In the recent CTE exam, tube current modulation, lowering tube potential, and iterative reconstruction techniques were applied. Only singe portal phase imaging was performed, whereas dual dynamic phases had been obtained in 2011. The similar image quality can be identified, comparing picture-in-picture images.
CONCLUSIONS
CTE allows the identification of intramural and extraintestinal sign of IBD such as Crohn disease, intestinal TB, and intestinal BD. The specific findings of each disease may be helpful for the differential diagnosis and planning of treatment strategy. CT dose reduction issue using several advanced techniques is emphasized without compromising the diagnostic image quality.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Raptopoulos V, Schwartz RK, McNicholas MM, Movson J, Pearlman J, Joffe N. Multiplanar helical CT enterography in patients with Crohn's disease. AJR Am J Roentgenol. 1997;169:1545–1550. doi: 10.2214/ajr.169.6.9393162. [DOI] [PubMed] [Google Scholar]
- 2.Minordi LM, Vecchioli A, Mirk P, Bonomo L. CT enterography with polyethylene glycol solution vs CT enteroclysis in small bowel disease. Br J Radiol. 2011;84:112–119. doi: 10.1259/bjr/71649888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maglinte DD, Sandrasegaran K, Lappas JC, Chiorean M. CT enteroclysis. Radiology. 2007;245:661–671. doi: 10.1148/radiol.2453060798. [DOI] [PubMed] [Google Scholar]
- 4.Stange EF, Travis SP, Vermeire S, et al. European evidence based consensus on the diagnosis and management of Crohn's disease: definitions and diagnosis. Gut. 2006;55(Suppl 1):i1–i15. doi: 10.1136/gut.2005.081950a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Meyers MA, McGuire PV. Spiral CT demonstration of hypervascularity in Crohn disease: "vascular jejunization of the ileum" or the "comb sign". Abdom Imaging. 1995;20:327–332. doi: 10.1007/BF00203365. [DOI] [PubMed] [Google Scholar]
- 6.Paulsen SR, Huprich JE, Fletcher JG, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. 2006;26:641–657. doi: 10.1148/rg.263055162. [DOI] [PubMed] [Google Scholar]
- 7.Booya F, Fletcher JG, Huprich JE, et al. Active Crohn disease: CT findings and interobserver agreement for enteric phase CT enterography. Radiology. 2006;241:787–795. doi: 10.1148/radiol.2413051444. [DOI] [PubMed] [Google Scholar]
- 8.Hara AK, Alam S, Heigh RI, Gurudu SR, Hentz JG, Leighton JA. Using CT enterography to monitor Crohn's disease activity: a preliminary study. AJR Am J Roentgenol. 2008;190:1512–1516. doi: 10.2214/AJR.07.2877. [DOI] [PubMed] [Google Scholar]
- 9.Bodily KD, Fletcher JG, Solem CA, et al. Crohn Disease: mural attenuation and thickness at contrast-enhanced CT Enterography: correlation with endoscopic and histologic findings of inflammation. Radiology. 2006;238:505–516. doi: 10.1148/radiol.2382041159. [DOI] [PubMed] [Google Scholar]
- 10.Madureira AJ. The comb sign. Radiology. 2004;230:783–784. doi: 10.1148/radiol.2303020645. [DOI] [PubMed] [Google Scholar]
- 11.Lee SS, Ha HK, Yang SK, et al. CT of prominent pericolic or perienteric vasculature in patients with Crohn's disease: correlation with clinical disease activity and findings on barium studies. AJR Am J Roentgenol. 2002;179:1029–1036. doi: 10.2214/ajr.179.4.1791029. [DOI] [PubMed] [Google Scholar]
- 12.Colombel JF, Solem CA, Sandborn WJ, et al. Quantitative measurement and visual assessment of ileal Crohn's disease activity by computed tomography enterography: correlation with endoscopic severity and C reactive protein. Gut. 2006;55:1561–1567. doi: 10.1136/gut.2005.084301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Solem CA, Loftus EV, Jr, Fletcher JG, et al. Small-bowel imaging in Crohn's disease: a prospective, blinded, 4-way comparison trial. Gastrointest Endosc. 2008;68:255–266. doi: 10.1016/j.gie.2008.02.017. [DOI] [PubMed] [Google Scholar]
- 14.Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997;202:597–610. doi: 10.1148/radiology.202.3.9051003. [DOI] [PubMed] [Google Scholar]
- 15.Vogel J, da Luz Moreira A, Baker M, et al. CT enterography for Crohn's disease: accurate preoperative diagnostic imaging. Dis Colon Rectum. 2007;50:1761–1769. doi: 10.1007/s10350-007-9005-6. [DOI] [PubMed] [Google Scholar]
- 16.Paulsen SR, Huprich JE, Hara AK. CT enterography: noninvasive evaluation of Crohn's disease and obscure gastrointestinal bleed. Radiol Clin North Am. 2007;45:303–315. doi: 10.1016/j.rcl.2007.03.009. [DOI] [PubMed] [Google Scholar]
- 17.Desreumaux P, Ernst O, Geboes K, et al. Inflammatory alterations in mesenteric adipose tissue in Crohn's disease. Gastroenterology. 1999;117:73–81. doi: 10.1016/s0016-5085(99)70552-4. [DOI] [PubMed] [Google Scholar]
- 18.Maglinte DD, Gourtsoyiannis N, Rex D, Howard TJ, Kelvin FM. Classification of small bowel Crohn's subtypes based on multimodality imaging. Radiol Clin North Am. 2003;41:285–303. doi: 10.1016/s0033-8389(02)00117-3. [DOI] [PubMed] [Google Scholar]
- 19.Schwartz DA, Loftus EV, Jr, Tremaine WJ, et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology. 2002;122:875–880. doi: 10.1053/gast.2002.32362. [DOI] [PubMed] [Google Scholar]
- 20.Bruining DH, Siddiki HA, Fletcher JG, Tremaine WJ, Sandborn WJ, Loftus EV., Jr Prevalence of penetrating disease and extraintestinal manifestations of Crohn's disease detected with CT enterography. Inflamm Bowel Dis. 2008;14:1701–1706. doi: 10.1002/ibd.20529. [DOI] [PubMed] [Google Scholar]
- 21.Bruining DH, Siddiki HA, Fletcher JG, et al. Benefit of computed tomography enterography in Crohn's disease: effects on patient management and physician level of confidence. Inflamm Bowel Dis. 2012;18:219–225. doi: 10.1002/ibd.21683. [DOI] [PubMed] [Google Scholar]
- 22.Booya F, Akram S, Fletcher JG, et al. CT enterography and fistulizing Crohn's disease: clinical benefit and radiographic findings. Abdom Imaging. 2009;34:467–475. doi: 10.1007/s00261-008-9419-1. [DOI] [PubMed] [Google Scholar]
- 23.Wu YW, Tang YH, Hao NX, Tang CY, Miao F. Crohn's disease: CT enterography manifestations before and after treatment. Eur J Radiol. 2012;81:52–59. doi: 10.1016/j.ejrad.2010.11.010. [DOI] [PubMed] [Google Scholar]
- 24.Wu YW, Tao XF, Tang YH, Hao NX, Miao F. Quantitative measures of comb sign in Crohn's disease: correlation with disease activity and laboratory indications. Abdom Imaging. 2012;37:350–358. doi: 10.1007/s00261-011-9808-8. [DOI] [PubMed] [Google Scholar]
- 25.Epstein D, Watermeyer G, Kirsch R. Review article: the diagnosis and management of Crohn's disease in populations with high-risk rates for tuberculosis. Aliment Pharmacol Ther. 2007;25:1373–1388. doi: 10.1111/j.1365-2036.2007.03332.x. [DOI] [PubMed] [Google Scholar]
- 26.Akhan O, Pringot J. Imaging of abdominal tuberculosis. Eur Radiol. 2002;12:312–323. doi: 10.1007/s003300100994. [DOI] [PubMed] [Google Scholar]
- 27.Makanjuola D. Is it Crohn's disease or intestinal tuberculosis? CT analysis. Eur J Radiol. 1998;28:55–61. doi: 10.1016/s0720-048x(97)00097-1. [DOI] [PubMed] [Google Scholar]
- 28.Lakhanpal S, Tani K, Lie JT, Katoh K, Ishigatsubo Y, Ohokubo T. Pathologic features of Behcet's syndrome: a review of Japanese autopsy registry data. Hum Pathol. 1985;16:790–795. doi: 10.1016/s0046-8177(85)80250-1. [DOI] [PubMed] [Google Scholar]
- 29.Sakane T, Takeno M, Suzuki N, Inaba G. Behcet's disease. N Engl J Med. 1999;341:1284–1291. doi: 10.1056/NEJM199910213411707. [DOI] [PubMed] [Google Scholar]
- 30.Cheon JH, Kim ES, Shin SJ, et al. Development and validation of novel diagnostic criteria for intestinal Behcet's disease in Korean patients with ileocolonic ulcers. Am J Gastroenterol. 2009;104:2492–2499. doi: 10.1038/ajg.2009.331. [DOI] [PubMed] [Google Scholar]
- 31.Ha HK, Lee HJ, Yang SK, et al. Intestinal Behcet syndrome: CT features of patients with and patients without complications. Radiology. 1998;209:449–454. doi: 10.1148/radiology.209.2.9807572. [DOI] [PubMed] [Google Scholar]
- 32.Chae EJ, Do KH, Seo JB, et al. Radiologic and clinical findings of Behcet disease: comprehensive review of multisystemic involvement. Radiographics. 2008;28:e31. doi: 10.1148/rg.e31. [DOI] [PubMed] [Google Scholar]
- 33.Iida M, Kobayashi H, Matsumoto T, et al. Postoperative recurrence in patients with intestinal Behcet's disease. Dis Colon Rectum. 1994;37:16–21. doi: 10.1007/BF02047208. [DOI] [PubMed] [Google Scholar]
- 34.Kasahara Y, Tanaka S, Nishino M, Umemura H, Shiraha S, Kuyama T. Intestinal involvement in Behcet's disease: review of 136 surgical cases in the Japanese literature. Dis Colon Rectum. 1981;24:103–106. doi: 10.1007/BF02604297. [DOI] [PubMed] [Google Scholar]
- 35.Ghonge NP, Aggarwal B, Gothi R. CT enterography: state-of-the-art CT technique for small bowel imaging. Indian J Gastroenterol. 2013;32:152–162. doi: 10.1007/s12664-013-0307-4. [DOI] [PubMed] [Google Scholar]
- 36.Desmond AN, O'Regan K, Curran C, et al. Crohn's disease: factors associated with exposure to high levels of diagnostic radiation. Gut. 2008;57:1524–1529. doi: 10.1136/gut.2008.151415. [DOI] [PubMed] [Google Scholar]
- 37.Jung YS, Park DI, Kim ER, et al. Quantifying exposure to diagnostic radiation and factors associated with exposure to high levels of radiation in Korean patients with inflammatory bowel disease. Inflamm Bowel Dis. doi: 10.1097/MIB.0b013e31828c844f. Epub 2013 May 22. DOI: 10.1097/MIB.0b013e31828c844f. [DOI] [PubMed] [Google Scholar]
- 38.Lee CH, Goo JM, Ye HJ, et al. Radiation dose modulation techniques in the multidetector CT era: from basics to practice. Radiographics. 2008;28:1451–1459. doi: 10.1148/rg.285075075. [DOI] [PubMed] [Google Scholar]
- 39.Yu L, Bruesewitz MR, Thomas KB, Fletcher JG, Kofler JM, McCollough CH. Optimal tube potential for radiation dose reduction in pediatric CT: principles, clinical implementations, and pitfalls. Radiographics. 2011;31:835–848. doi: 10.1148/rg.313105079. [DOI] [PubMed] [Google Scholar]
- 40.Kaza RK, Platt JF, Al-Hawary MM, Wasnik A, Liu PS, Pandya A. CT enterography at 80 kVp with adaptive statistical iterative reconstruction versus at 120 kVp with standard reconstruction: image quality, diagnostic adequacy, and dose reduction. AJR Am J Roentgenol. 2012;198:1084–1092. doi: 10.2214/AJR.11.6597. [DOI] [PubMed] [Google Scholar]
- 41.Wold PB, Fletcher JG, Johnson CD, Sandborn WJ. Assessment of small bowel Crohn disease: noninvasive peroral CT enterography compared with other imaging methods and endoscopy: feasibility study. Radiology. 2003;229:275–281. doi: 10.1148/radiol.2291020877. [DOI] [PubMed] [Google Scholar]