

Abstract
Background
Vibration-induced finger flexion reflex (VFR) is inhibited with acupuncture to TE 5 or LI 4 at the skin innervated by the radial nerve.
Objective
The aim of this study was to determine if acupoints in regions innervated by the radial nerve are specific to inhibit VFR.
Materials and Methods
This experiment was performed using a crossover design with 3 acupuncture groups (needle insertion to the right LU 11, PC 9, or SI 1) and a control group (no needle treatment). Each acupoint was randomly needled on separate days. Ten healthy volunteers were recruited for this study. VFR was induced by applying vibration on the volar side of the right middle fingertip. An acupuncture needle was inserted in the acupoint and retained for 5 minutes. For the main outcome measure, maximum finger flexion force (MFFF) was measured during vibration and was compared among four groups.
Results
MFFFs in the acupuncture groups were significantly lower (p<0.05) than that in the control group. However, no significant difference was observed in MFFFs in the three intervention groups after acupuncture to LU 11, PC 9, and SI 1.
Conclusions
Acupuncture to the right LU 11, PC 9, or SI 1 point inhibited the ipsilateral VFR, which suggests that afferent inputs from the radial nerve with needle insertion were not specific, compared with those from the median and ulnar nerves to suppress neuronal activities in the VFR reflex circuits.
Key Words: Stiff Muscles, Vibration, Flexion Reflex, Acupuncture, Radial Nerve, Median Nerve, Ulnar Nerve
Introduction
Clinical acupuncturists have noticed that tension in stiff muscles can be reduced with needle insertion. The effectiveness of acupuncture in musculoskeletal diseases has been described in several acupuncture textbooks,1–4 and the main focus has been on the analgesic effect of acupuncture on chronic pain.4–6 Studies have shown that acupuncture suppresses afferent nerve activities that convey pain messages to the dorsal horn of the spinal cord.4,7 In musculoskeletal diseases such as lumbago, however, acupuncturists often observe clinically that chronic pain is attributed to continuous excessive tension in the skeletal muscles. In addition to producing an analgesic effect, acupuncture relaxes stiff muscles in patients who have chronic pain and, thus, might also help mitigate their pain. From this perspective, it is important to understand the effect of acupuncture on neuronal activities in the skeletal muscles.
Applying vibration to the volar side of the fingertip elicits a flexion reflex, called a vibration-induced finger flexion reflex (VFR).8 In general, VFR appears at the beginning of the vibration, gradually increases during the vibration, and disappears immediately after the vibration ceases. It has been observed that VFR is markedly reduced after the fingertip to which vibration will be applied is anesthetized, cooled, or had a skin graft. Therefore, the skin mechanoreceptors are considered to be receptors of this reflex.8–10 The flexor digitorum superficialis muscle (mFDS) has been considered as the main effector of VFR in studies using an electromyogram (EMG).9–14 Tonic flexion in the mFDS may occur because of recruitment and summation of the excitement from the afferent nerve with vibratory stimuli applied to the mFDS. Based on a cross-correlogram between motor-unit spikes in the mFDS and vibratory stimulus during VFR, the mFDS is assumed to be activated through the following two reflex arcs: (1) the spinal short loop and (2) the supraspinal long loop.10,13,15
Based on the well-established reflex circuit of VFR, which sustains involuntary muscular contraction induced by innoxious stimulation, several studies have been conducted to investigate the effects of acupuncture on VFR.12,14–20 These studies demonstrated consistently that acupuncture at the TE 5 acupoint12,15,16 (Waiguan: located 2 cun superior to the midline of the dorsal carpal cross-striation between the ulna and radius)21 or the LI 4 acupoint14,17–20 (Hegu: located between the first and second metacarpals in the midline of the radial side of the second metacarpal bone)21 inhibited VFR. The skin regions at TE 5 and LI 4 acupoints are innervated by the posterior cutaneous nerve of the forearm and the superficial ramus, respectively,21 which are derived from the radial nerve. Anatomically, it seems important to activate the radial nerve to inhibit VFR. However, from those studies alone, it cannot be proven that activation of the radial nerve with acupuncture has specific tension-easing effect on the forearm flexors.
The aim of this study was to investigate if activation of the radial nerve with acupuncture to the acupoint would specifically inhibit VFR.
Materials and Methods
Participants
Ten healthy volunteers (mean±standard deviation [SD]: 29.9±6.7 years; 8 males and 2 females) who had previously received acupuncture participated in the study. This experiment was conducted using a crossover design with 3 acupuncture groups and a control group (no needle treatment). All subjects provided written informed consent after the purpose and format of the study were explained to them. The ethics committee of Showa University School of Medicine approved this study.
Experimental Setting
Each subject was blindfolded and seated in an adjustable chair during the experiment. The right forearm of the subject was placed on the armrest to ensure its consistent position throughout the experiment. The right elbow and wrist joints were immobilized using a hook-and-loop fastener attached to the armrest (Fig. 1). The right hand was placed on a pad on the top of a box containing a vibrator with the palm faced down and the wrist in approximately 30° of dorsiflexion (Fig. 1). The right middle fingertip was placed on a force transducer (9E01-L2-5K; NEC San-ei Instruments, Ltd. Tokyo, Japan) that was attached to the tip of the vibrator. Next, a 60-Hz vibration with 1-mm displacement amplitude was applied for 20 seconds to the volar side of the right middle fingertip.14,22 Vibration was delivered using an electromagnetic vibrator (FF225N; Foster Electric Co., Ltd. Tokyo, Japan) driven by a sine-pulse generator (VP-7421A Function Generator; Matsushita Electrical Industrial Co., Ltd., Tokyo, Japan) coupled with a power amplifier (1706; Bose Corp., Tokyo, Japan). The output from the amplifier to the vibrator was monitored using a digital oscilloscope (Tectronix TDS 360p; Sony Corp., Tokyo, Japan) to measure the driving force of the vibrator, which was found to be 3.5–4.0 V to maintain a 1-mm amplitude of the 60 Hz vibration. Tonic finger flexion force induced by the vibration was measured isometrically with the force transducer, through an amplifier (6M67; NEC San-ei Instruments, Ltd. Tokyo, Japan). Force measurements were recorded with a pen recorder (VP-6712A; Matsushita Communication Industrial Co., Ltd. Tokyo, Japan).
FIG. 1.

Schema for experimental settings. Vibration at 60 Hz was applied to the volar side of the middle fingertip. Flexion force was measured by a pen recorder through a force transducer.
Measurement of VFR
VFRs were measured before and after acupuncture (5-minute needle retention).23 Specifically, measurements were taken 10 and 5 minutes before needle insertion, and at 5-minute intervals beginning immediately after needle removal, for a period of 40 minutes.
VFRs in the control group were measured at the same timepoints without acupuncture. This experiment was performed in accordance with previous studies.14,17–20,22
Acupuncture
Acupoints were used in the hand, under which no muscles exist to restrict afferent inputs from the skin. An acupuncturist applied a needle at the following three acupoints (Fig. 2), which are located over the dorsal surface of the right hand of each subject: (1) LU 11 (Shaoshang on the radial side of the thumb, 0.1 finger-cun proximolateral to the radial corner of the thumbnail)21,24; (2) PC 9 (Zhongchong on the radial side of the middle finger, 0.1 finger-cun proximolateral to the radial corner of the middle fingernail)21; or (3) SI 1 (Shaoze on the ulnar side of the little finger, 0.1 finger-cun proximomedial to the ulnar corner of the little fingernail).21,24 This study used the crossover protocol; therefore, each acupoint was randomly needled on separate days. To prevent a carryover effect, intervals of more than 1 week between each acupuncture treatment were maintained. Disposable stainless steel needles (diameter, 0.16 mm; length, 40 mm; Seirin Co., Ltd. Shizuoka, Japan) were used. Needle insertion was performed using the tapping-in method. The depth of needle insertion was 4 mm, and the needle was at a right angle to the skin and was maintained in this position (needle retention)23 for 5 minutes. No manipulation was performed during needle retention.
FIG. 2.
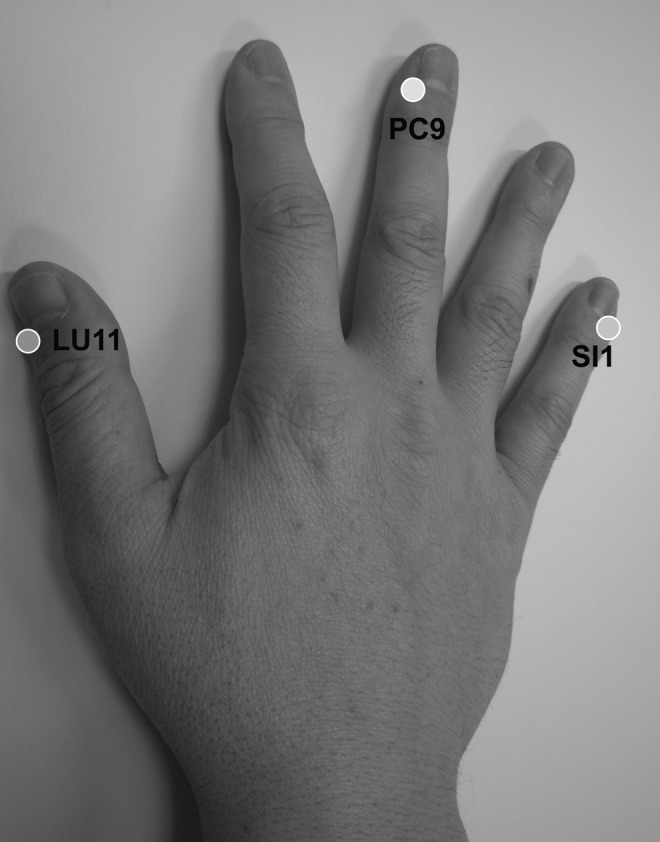
Acupoint locations in the right hand: LU 11; PC 9; and SI 1.
Statistical Analysis
For statistical comparisons, we measured the maximum finger flexion force (MFFF) of VFR at each measuring point, because the MFFF during VFR is a good representative of the entire finger flexor muscle activity during vibratory stimulation.14,22 The MFFF at 5 minutes before acupuncture and at each timepoint after removal of the needle (up to 40 minutes after) were expressed as percentages of the MFFF measured 10 minute before acupuncture in each subject according to previous studies.14,17–19,22 Using these data, the control group was compared with each of the acupuncture groups, and a comparison was made among the acupuncture groups at each measured timepoint, according to the Wilcoxon signed-rank test. Statistical analyses were performed using SPSS v.15.0J (SPSS, Chicago, IL).
Results
Figure 3 illustrates sample recording of the finger flexion force induced by VFR from a typical subject. The finger flexion force after acupuncture, applied to the LU 11, PC 9, or SI 1 acupoint, decreased in comparison with that before acupuncture. The values of MFFF calculated before acupuncture were 2.32 N, 2.06 N, and 2.17 N, which decreased to 0.62 N, 0.72 N, and 0.98 N after needle removal from the LU 11, PC 9, and SI 1 acupoints, respectively. However, this decrease in MFFF was not observed in the control group.
FIG. 3.
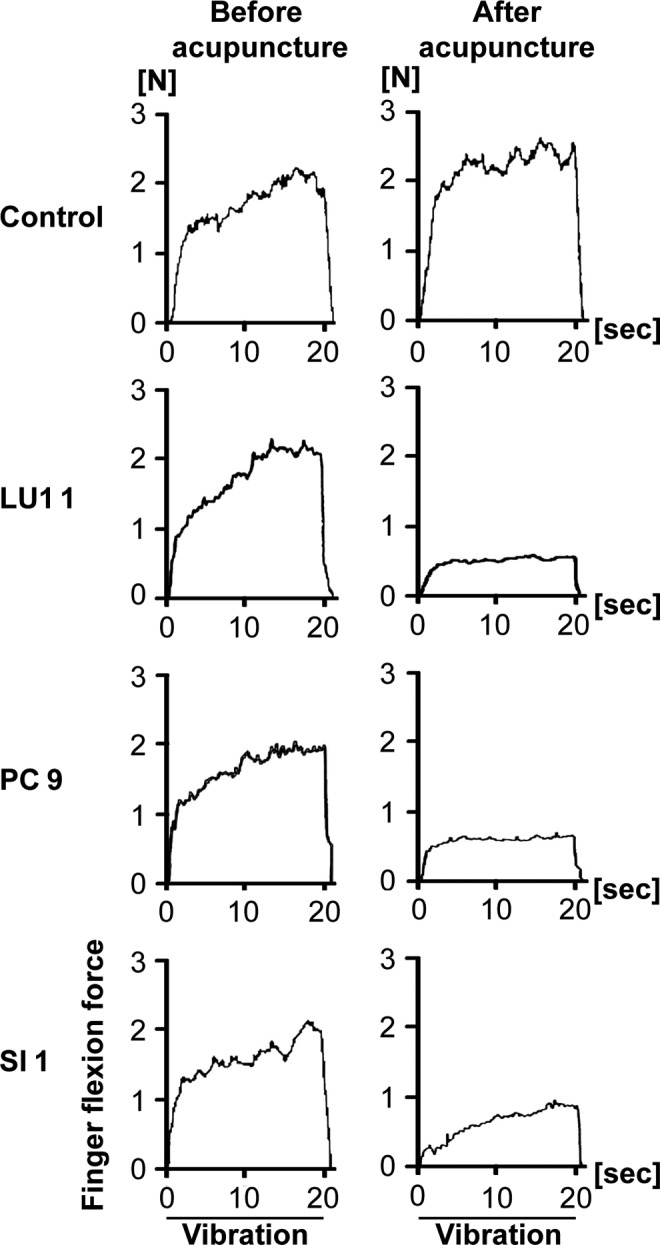
Records of finger flexion forces induced by vibration-induced finger flexion reflex (VFR) in a typical subject before (left column) and after (right column) acupuncture. The subjects in the control group (upper) had no obvious change in VFR caused by adaptation or fatigue in the finger flexion muscles. Finger flexion force during VFR decreased after acupuncture (second, third, and fourth row from the top), compared with those before acupuncture. sec, seconds.
Changes in MFFF in the acupuncture and control groups are shown in Figure 4. Immediately after needle removal to 40 minutes after needle removal, the MFFFs of the acupuncture groups (LU 11, PC 9, and SI 1) were significantly lower (p<0.05) than that of the control group. However, no statistical difference in the MFFFs at each measured timepoint was observed among the acupuncture groups.
FIG. 4.

Changes in maximum finger flexion force (MFFF) for 10 subjects in the acupuncture group (the left box, LU 11; the second box from the left, PC 9; and the third box from the left, SI 1) and control group (the right box in each timepoint). Vertical axis is the percentage of 10 minutes (min) before value of MFFF and the horizontal axis is time. The top, middle, and bottom lines of the boxes correspond to the 75th, 50th (median), and 25th percentiles, respectively. The whiskers extend from the minimum to the maximum value. The circles indicate the arithmetic mean. The broken line represents baseline (10 min before value of MFFF). *p<0.05, **p<0.01.
Discussion
This study showed that VFR was inhibited with acupuncture at the LU 11, PC 9, or SI 1 acupoint in the skin area dominated by the radial, median, or ulnar nerves, respectively. The inhibitory effect with needle insertion at LU 11 in the thumb obtained in this study supports previous findings of the inhibitory effect obtained with needle insertion at the TE 312,15,16 or LI 414,17–20 acupoints. This implies that the radial nerve has an inhibitory connection with the relative motor neurons to the forearm flexor muscles in the spinal cord. Similar to the acupoints on the radial nerve region, VFR was inhibited with acupuncture to respective acupoints in the skin areas dominated by the median and ulnar nerves. These findings suggest that the radial nerve was not specific to VFR inhibition, and the afferent nerves innervating the forearm have inhibitory connections with the relative motor neurons of the forearm flexor muscles in the spinal cord.
In the current study, MFFF was used only during vibratory stimulation as an indicator of VFR, because MFFF reflects activation of the mFDS reliably during vibratory stimulation. In a previous study, the current authors confirmed that there was a significant positive correlation between MFFF and the area under the curve (AUC) of the flexion force,22 that existed between MFFF and integrated surface EMG,14 and that existed between the AUC of the flexion force and integrated surface EMG.14 Therefore, a decrease in MFFF indicates a decrease in the entire muscle activity during vibratory stimulation.
An interesting question remains: “Is deep needling treatment that reaches the muscle better than superficial needling treatment that does not reach the muscle?” Ceccheerelli et al. argued that the muscular afferents are important for pain control in humans.25 In another acupuncture study using functional magnetic resonance imaging in humans, Feng et al. proposed that needle insertion to the deep muscles was necessary to achieve appreciable clinical effects.26 Moreover, Hayward et al. reported that the increase in discharges in group III and IV afferent fibers from the muscle might be responsible for inhibition of the homonymous or heteronymous motoneurons in cats.27 On the basis of these findings, it was assumed that activation of the afferent fibers innervating the deep muscles under TE 5 and LI 4 acupoints with needle insertion may play an important role in VFR inhibition.12,14–20 However, in the current study, VFR was clearly inhibited by acupuncture at the acupoints under which no muscles exist. The current findings strongly suggest that, with acupuncture treatment, activities arising exclusively from the skin afferent fibers worked toward reducing muscle tension significantly.
It is well-known that acupuncture activates various groups of the afferent fibers.1,28,29 Using single-unit nerve recording techniques in rats, Kagitani et al. demonstrated that manual acupuncture needle stimulation to the hind limbs activated the single-unit afferents belonging to the group I, II, III, and IV fibers in the spinal dorsal roots.28 The current authors have previously demonstrated that pain-eliciting transcutaneous electrical nerve stimulation (TENS) inhibited VFR, whereas non-pain-eliciting TENS did not.22 Furthermore, inhibitory effects induced by needle insertion with manipulations inducing stronger stimulations, are distinctly greater than that by needle insertion without any manipulations.18 Collectively, these results suggest that activation of the noxious afferent fibers may play an important role in VFR inhibition. The importance of the noxious stimulation in VFR inhibition is supported by the results of previous studies, which showed that high-intensity noxious TENS inhibited motor neuronal excitability in the upper extremity.30–33 This indicates that the noxious afferent fibers have an inhibitory connection with motor neurons in the spinal cord.30–33 A noxious component of acupuncture treatment may help significantly to ease excessive muscle tension, which might secondarily contribute toward mitigation of chronic pain.
VFR is assumed to be stimulated through the following two reflex arcs: (1) the spinal short loop and (2) the supraspinal long loop.9,13,15 Interestingly, the activities in the both loops are suppressed by acupuncture at the TE 5 acupoint in the upper extremity, and suppression on the supraspinal long loop lasts relatively longer than that on the short loop.15 Thus, the current authors presume that the activities in the long-loop circuit were mainly suppressed by sensory inputs from the LU 11, PC 9, or SI 1 acupoint elicited by needle insertion; therefore, a continuous decrease in VFR was observed after needle removal.
The current authors conducted a crossover study because fewer subjects are required to detect an acupuncture effect with needle insertion at three acupoints. As reported previously, crossover designs have often shown greater statistical power than parallel-group designs with large samples.34 The most significant problem of a crossover study is its carryover effect. To prevent a carryover effect, the current study was specifically designed based on a previous study, which had an interval of at least 1 week between acupuncture treatments.35
The current study had several limitations. There were only 10 subjects, who had previously received acupuncture and had moderate knowledge about it. Therefore, the effect of VFR inhibition should be tested in subjects who had not previously received acupuncture.
Conclusions
Acupuncture to the right LU 11, PC 9, or SI 1 point inhibited the ipsilateral VFR, which suggests that afferent inputs from the radial nerve with needle insertion were not specific, compared with those from the median and ulnar nerves to suppress neuronal activities in the VFR reflex circuits.
Acknowledgments
The authors thank Koji Sakurai (the Educational Foundation of Hanada Gakuen, Tokyo) for his support. Thanks are also extended to all participants of the Japan School of Acupuncture, Moxibustion, and Physiotherapy. The Educational Foundation of Hanada Gakuen funded this study. This work was supported by JSPS KAKENHI Grant Number 23500622.
Disclosure Statement
No competing financial interests exist.
References
- 1.Stux G. Berman B. Pomeranz B. Basics of Acupuncture. Berlin, Heidelberg & New York: Springer-Verlag; 2003. Scientific basis of acupuncture; pp. 7–86. [Google Scholar]
- 2.Helms MJ. Acupuncture Energetics. New York: Thieme; 1995. Treating musculoskeletal pain; pp. 457–520. [Google Scholar]
- 3.Hecker UH. Steveling A. Peuker TE. Kastner J. Practice of Acupuncture. New York: Thieme; 2005. Pragmatic five-step concept for treating locomotor pain and headaches; pp. 421–435. [Google Scholar]
- 4.Baldry EP. Acupuncture, Trigger Points and Musculoskeletal Pain. Brookline, MA: Elsevier Churchill Livingstone; 2005. Principles of trigger point acupuncture, The practical application of trigger point acupuncture; pp. 45–358. [Google Scholar]
- 5.Barlas P. Ting SL. Chesterton LS. Jones PW. Sim J. Effects of intensity of electroacupuncture upon experimental pain in healthy human volunteers: A randomized, double-blind, placebo-controlled study. Pain. 2006;122(1–2):81–89. doi: 10.1016/j.pain.2006.01.012. [DOI] [PubMed] [Google Scholar]
- 6.Hübscher M. Vogt L. Bernhörster M. Rosenhagen A. Banzer W. Effects of acupuncture on symptoms and muscle function in delayed-onset muscle soreness. J Altern Complement Med. 2008;14(8):1011–1016. doi: 10.1089/acm.2008.0173. [DOI] [PubMed] [Google Scholar]
- 7.Kim JH. Kim HY. Chung K. Chung JM. Electroacupuncture reduces the evoked responses of the spinal dorsal horn neurons in ankle-sprained rats. J Neurophysiol. 2011;105(5):2050–2057. doi: 10.1152/jn.00853.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eklund G. Hagbarth KE. Torebjork E. Exteroceptive vibration-induced finger flexion reflex in man. J Neurol Neurosurg Psychiatry. 1978;41(5):438–443. doi: 10.1136/jnnp.41.5.438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Motomiya Y. Physiological and clinical researches with humans into tonic vibratory and finger flexion reflexes caused by oscillation [in Japanese] Jikeikai Med J. 1984;99(5):725–733. [Google Scholar]
- 10.Kodachi K. Characteristics of finger flexion reflex induced by finger tip vibration [in Japanese] Jikeikai Med J. 1987;102(5):1279–1290. [Google Scholar]
- 11.Endo Y. Homma I. Koizumi H. Marumo E. Sakai T. Characteristics of vibration-induced finger flexion reflex and its clinical applications [in Japanese] Jikeikai Med J. 1981;28(3):187–192. [Google Scholar]
- 12.Homma S. Nakajima Y. Toma S. Inhibitory effect of acupuncture on the vibration-induced finger flexion reflex in man. Electroenceph Clin Neurophysiol. 1985;61(2):150–156. doi: 10.1016/0013-4694(85)91054-5. [DOI] [PubMed] [Google Scholar]
- 13.Kodachi K. Sibuya M. Homma I. Difference in electromyographic response of finger flexion muscles between tonic reflex and finger flexion reflex induced by finger tip vibration. Neurosci Lett. 1987;75(3):303–307. doi: 10.1016/0304-3940(87)90539-8. [DOI] [PubMed] [Google Scholar]
- 14.Takakura N. Yajima H. Takayama M. Kawase A. Homma I. Inhibitory effect of needle penetration on vibration-induced finger flexion reflex in humans. Acupunct Med. 2010;28(2):78–82. doi: 10.1136/aim.2009.001149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kodachi K. Sibuya M. Endo Y. Homma I. Inhibitory effect of acupuncture on the finger flexion reflex induced by finger tip vibration. Neurosci Res. 1987;4(5):419–423. doi: 10.1016/0168-0102(87)90007-1. [DOI] [PubMed] [Google Scholar]
- 16.Homma I. Endo Y. Sakai T. Inhibitory effect of acupuncture on the vibration-induced finger flexion reflex in man. Neurosci Lett. 1980;19(2):209–212. doi: 10.1016/0304-3940(80)90196-2. [DOI] [PubMed] [Google Scholar]
- 17.Takakura N. Kanamaru A. Sibuya M. Effect of acupuncture at right Hoku point on the bilateral vibration-induced finger flexion reflex in man. Am J Chin Med. 1992;20(2):115–126. doi: 10.1142/S0192415X92000126. [DOI] [PubMed] [Google Scholar]
- 18.Takakura N. Ogawa H. Iijima S, et al. Effect of acupuncture at the right Hoku point on bilateral vibration-induced finger flexion reflex in man: Comparison between in situ and Sparrow Pecking technique. Am J Chin Med. 1993;21(3–4):213–219. doi: 10.1142/S0192415X93000248. [DOI] [PubMed] [Google Scholar]
- 19.Takakura N. Ogawa H. Iijima S, et al. Effect of acupuncture at the Hoku point on vibration-induced finger flexion reflex in man: Comparison between [sic] press needle technique, electroacupuncture, and in situ technique. Am J Chin Med. 1995;23(3–4):313–318. doi: 10.1142/S0192415X95000377. [DOI] [PubMed] [Google Scholar]
- 20.Takakura N. Iijima S. Kanamaru A, et al. Vibration-induced finger flexion reflex and inhibitory effect of acupuncture on this reflex in cervical spinal cord injury patients. Neurosci Res. 1996;26(4):391–394. doi: 10.1016/s0168-0102(96)01119-4. [DOI] [PubMed] [Google Scholar]
- 21.Mehrab D. Textbook of Acupuncture. Saarbrücken: VDM Verlag Dr. Müller GmbH & Co.; 2010. The fourteen channels (Jing luo) pp. 77–427. [Google Scholar]
- 22.Takakura N. Yajima H. Homma I. Inhibitory effect of pain-eliciting transcutaneous electrical stimulation on vibration-induced finger flexion reflex in the human upper limb. Jpn J Physiol. 2004;54(3):243–248. doi: 10.2170/jjphysiol.54.243. [DOI] [PubMed] [Google Scholar]
- 23.World Health Organization (WHO) WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region. Geneva: WHO Western Pacific Region; 2007. Acupuncture and moxibustion; p. 247. [Google Scholar]
- 24.World Health Organization (WHO) WHO Standard Acupuncture Point Locations in the Western Pacific Region. Geneva: WHO Western Pacific Region; 2008. WHO standard acupuncture point location; pp. 25–231. [Google Scholar]
- 25.Ceccheerelli F. Bordin M. Gagliardi G. Caravello M. Comparison between superficial and deep acupuncture in the treatment of the shoulder's myofascial pain: A randomized and controlled study. Acupunct Electrother Res. 2001;26(4):229–238. doi: 10.3727/036012901816355938. [DOI] [PubMed] [Google Scholar]
- 26.Feng Y. Bai L. Ren Y, et al. fMRI connectivity analysis of acupuncture effects on the whole brain network in mild cognitive impairment patients. Magn Reson Imaging. 2012;30(5):672–682. doi: 10.1016/j.mri.2012.01.003. [DOI] [PubMed] [Google Scholar]
- 27.Hayward L. Breitbach D. Rymer WZ. Increased inhibitory effects on close synergists during muscle fatigue in the decerebrate cat. Brain Res. 1988;440(1):199–203. doi: 10.1016/0006-8993(88)91178-x. [DOI] [PubMed] [Google Scholar]
- 28.Kagitani F. Uchida S. Hotta H. Aikawa Y. Manual acupuncture needle stimulation of the rat hindlimb activates groups I, II, III, and IV single afferent nerve fibers in the dorsal spinal roots. Jpn J Physiol. 2005;55(3):149–155. doi: 10.2170/jjphysiol.R2120. [DOI] [PubMed] [Google Scholar]
- 29.Kagitani F. Uchida S. Hotta H. Afferent nerve fibers and acupuncture. Auton Neurosci. 2010;157(1–2):2–8. doi: 10.1016/j.autneu.2010.03.004. [DOI] [PubMed] [Google Scholar]
- 30.Uncini A. Kujirai T. Gluck B. Pullman S. Silent period induced by cutaneous stimulation. Electroencephalogr Clin Neurophysiol. 1991;81(5):344–352. doi: 10.1016/0168-5597(91)90023-q. [DOI] [PubMed] [Google Scholar]
- 31.Walk D. Fisher MA. Effects of cutaneous stimulation on ipsilateral and contralateral motoneuron excitability: An analysis using H reflexes and F waves. Electromyogr Clin Neurophysiol. 1993;33(5):259–264. [PubMed] [Google Scholar]
- 32.Rossi A. Zalaffi A. Decchi B. Interaction of nociceptive and non-nociceptive cutaneous afferents from foot sole in common reflex pathways to tibialis anterior motoneurones in humans. Brain Res. 1996;714(1–2):76–86. doi: 10.1016/0006-8993(95)01483-7. [DOI] [PubMed] [Google Scholar]
- 33.Inghilleri M. Cruccu G. Argenta M. Polidori L. Manfredi M. Silent period in upper limb muscles after noxious cutaneous stimulation in man. Electroencephalogr Clin Neurophysiol. 1997;105(2):109–115. doi: 10.1016/s0924-980x(97)96579-6. [DOI] [PubMed] [Google Scholar]
- 34.Max MB. The design of clinical trials for treatment of pain. In: Max MB, editor; Lynn J, editor. Symptom Research: Methods and Opportunities. Washington, DC: National Institutes of Health; 2003. [Jul 21;2013 ]. [Google Scholar]
- 35.Takakura N. Yajima H. Analgesic effect of acupuncture needle penetration: A double-blind crossover study. Open Med. 2009;3(2):e54–e61. [PMC free article] [PubMed] [Google Scholar]