

Abstract
Introduction:
Comparing ante-mortem and post-mortem dental data is a principal method of identification in forensic odontology. Radiographic images of amalgam have been used in dental forensics for identification due to their unique appearance.
Aim:
The aim of this study was to investigate whether radio-opaque composite restorations have a potential for identification in forensic odontology.
Materials and Methods:
Thirty typodont mandibular first molar teeth were prepared with Class-II (proximo-occlusal) cavities and restored with a radio-opaque composite (Tetric N-Ceram). Two sets of standardized radiographs were taken from the 30 teeth, keeping the radiological parameters constant. One set of these 30 radiographs was named as SET 1. Ten randomly chosen radiographs from the other set and two other radiographs of Class-II composite restorations in typodont teeth constituted SET 2. Thirty dentally trained examiners were asked to match the 12 radiographic images of SET 2 with those of SET 1.
Results:
The results show that 15 examiners were able to correctly match all the 12 images. Statistical analysis was done using kappa statistical test.
Conclusion:
This study shows that, if the post-mortem radiographs are accurate duplicates of ante-mortem radiographs of composite restorations, then the shape of the composite restoration is unique and can be used for identification.
Keywords: Composite dental resin, composite resins, forensic dentistry, dental radiography
Introduction
Forensic odontology plays a very important role in identification of persons, especially those who cannot be identified visually by members of the family, relatives, and friends of the deceased. Dental identification is a frequently applied method for identification of persons involved in mass disaster, accidents, and crime investigations,[1,2] where the remains are disfigured, mutilated, or skeletonized. Dental identification predominantly involves comparison of ante-mortem and post-mortem records. The records include charts or case sheets, photographs, radiographs, models, etc. Among these, dental radiography is a non-invasive method used to uncover data which are embedded within the soft tissues and in the teeth, which are not found by physical examination or are completely discernible during physical examination. A dental radiograph is a very common constituent of a patient record or case sheet. And comparison of these ante-mortem radiographs with post-mortem dental radiographs produces reliable results in a simple manner.[3] Comparison involves examining the features of the same jaw sector, single tooth or even a tooth surface for concordance between the ante-mortem and post-mortem data.[4] In different countries, the law requires a different number of concordant features to establish identification of a person.[5] Authors also differ in their opinion regarding the minimum number of concordant points required for positive identification.[6,7,8,9,10] Dental identification cannot be based on a predetermined number of comparative points because in dental identification certain coincident characteristics are accorded more weight than others. A single ante-mortem radiograph of a tooth compared with a post-mortem radiograph could be the only basis for an identification, whereas ante-mortem and post-mortem dental charts showing three or four matching restorations might be regarded as containing insufficient criteria for an identification.[8]
Kieser-Nielson[10] in 1980 stated that no physical or dental feature is unique. But, any physical feature does possess a certain discriminatory potential according to its frequency of occurrence. Further, Kieser-Nielson[2] stated that the restored tooth surface as seen in the radiograph should be regarded as the smallest unit to consider in the comparison of dental restorations for identification purposes. Comparing the ante-mortem and post-mortem dental radiographs along with the written data helps in establishing identification of the individual. de Villiers and Phillips presented two cases in which a single extraordinary dental feature was useful for identification of the individuals.[11] Similarly, Phillips[12] in 1983 studied the patterns of amalgam restoration and their uniqueness and found that amalgam fillings in first molar have a low degree of uniqueness. Contrary to Phillips, Borrmann and Gröndahl[13] in 1990 through their study concluded that when two sets of bitewing radiographs of restored teeth are compared, the observers could accurately identify all the cases when simple amalgam restorations were present. Later in 2009, Phillips and Stuhlinger[14] stated that if the ante-mortem and post-mortem radiographs of a compound amalgam restoration are exactly the same, then this feature is unique and can be used for identification. Zondag and Phillips[15] in 2009 have done a study comparing composite restorations and have found encouraging results that can be used in the identification of victims.
According to the American Dental Association, Council on Dental Materials, Instruments and Equipment, radiopacity is one of the five basic requirements any restorative material must fulfill.[16] A radiopaque restoration allows for easy distinguishing of existing restorations and primary caries, evaluation of contours, overhangs and major voids in restoration, and also helps in the identification of recurrent caries.[17,18,19,20,21,22] Too high or too low radiopacity are both undesirable for a radiographic diagnosis. Several studies have suggested that the radiographic detection of caries is improved if radiopacity of the restorative material is similar or slightly greater than that of enamel.[23,24] The extreme radiopacity of amalgam is not ideal for radiographic detection of caries and defects adjacent to restorations, since the high radiopacity interferes directly in the contrast, impairs visual acuity and, consequently, diminishes the perception of details.[18,25]
Resin-based composites have been rapidly replacing amalgam due to their physical characteristics, ease of handling, and especially due to their satisfactory esthetic features. The radiopacity of composite resins is due to the incorporation of filler particles into the matrix (glass and ceramic particles containing heavy metals such as aluminum, barium, strontium, zirconium, and ytterbium).[26]
The aim of this study was to investigate the standardized radiographic images of radiopaque composite restorations in molar teeth regarding their discriminatory potential for identification in forensic odontology.
Materials and Methods
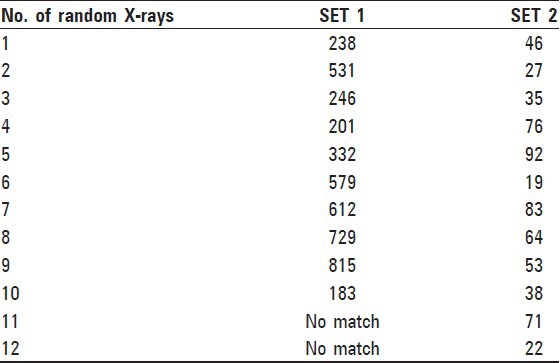
Thirty plastic typodont mandibular first molar teeth of natural size were used in this study. The typodont teeth that resemble the morphology of natural teeth are made of plastic materials such as ivorine, melamine, polycarbonate, etc., and are used for training students in restorative procedures. In this study, the teeth manufactured by Nissin co., Nakagyoku, Kyoto, Japan were used. In these 30 typodont mandibular teeth, Class-II (proximo-occlusal) cavities were prepared and restored with light cure composite (Tetric N-Ceram, Ivoclar-Vivadent, Schaan, Liechtenstein, Batch No.14523) by final year dental students [Figure 1]. Tetric N-Ceram is a light-curing, radiopaque nano-hybrid composite resin for direct dental restorative procedures [Figure 2]. Tetric N-Ceram has a high radiopacity of 400% aluminum compared to dental enamel which has a radiopacity of about 200%aluminum. The difference in radiopacity facilitates the radiographic detection of secondary caries, excess or inadequate quantities of material, air bubbles, and other imperfections. In this study, we required sufficient contrast in radiograph between the typodont and the restoration, which was provided by this material. The teeth were marked from 1 to 30 and mounted individually in a special acrylic mold to standardize the radiographic technique [Figure 3]. Two exact radiographs were taken, one to simulate the ante-mortem and the other to simulate the post-mortem radiographs by placing the cone perpendicular to the buccal aspect of each tooth and by maintaining the same source to object distance of 15 cm, same exposure time of 1 s, same mA of 10 units,and same kV of 70 units. The distance between the object (mounted tooth specimen) and the film was also standardized at 10 mm. One set of these 30 radiographs were labeled with a three-digit number and set aside as SET 1 (to simulate ante-mortem radiographs) [Figure 4]. Ten randomly chosen radiographic images from the other set of 30 radiographs and two other radiographs with Class-II composite fillings in similar typodont teeth were set aside as SET 2 (to simulate post-mortem radiographs) [Figure 5]. The remaining 20 radiographs from this set were not utilized in this study. The radiographs from SET 2 were each labeled with a two-digit number. The accurate correlation between SET 1 and SET 2 was recorded separately and not revealed to the examiners [Table 1]. The examiners were also not told about the presence of the two radiographs in SET 2 which did not have a match.
Figure 1.
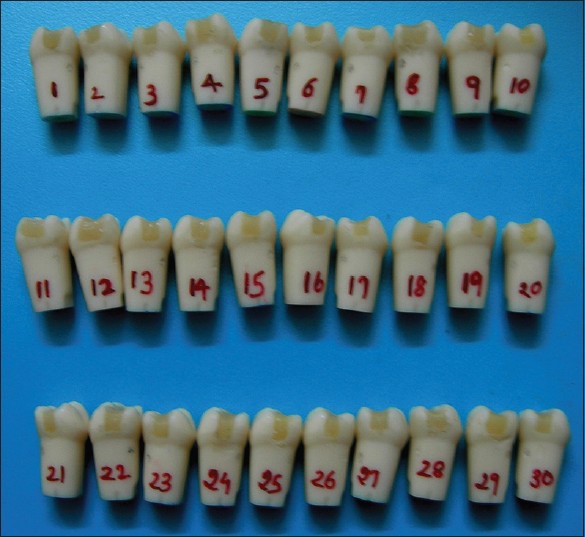
Typodont teeth numbered from 1 to 30 and restored with Class-II proximo-occlusal composite
Figure 2.

Tetric N-Ceram composite and Tetric N-Bond adhesive
Figure 3.
Typodont teeth were mounted individually in a special acrylic mold to standardize the radiographic technique
Figure 4.

Thirty radiographs in SET 1 to simulate ante-mortem radiographs
Figure 5.
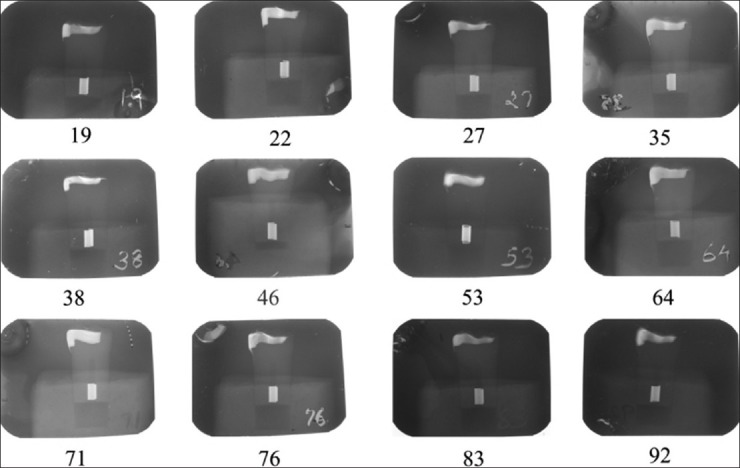
Ten randomly chosen radiographic images from the other set of 30 radiographs and two other radiographs with Class-II composite fillings in similar typodont teeth to simulate post-mortem radiographs in SET 2
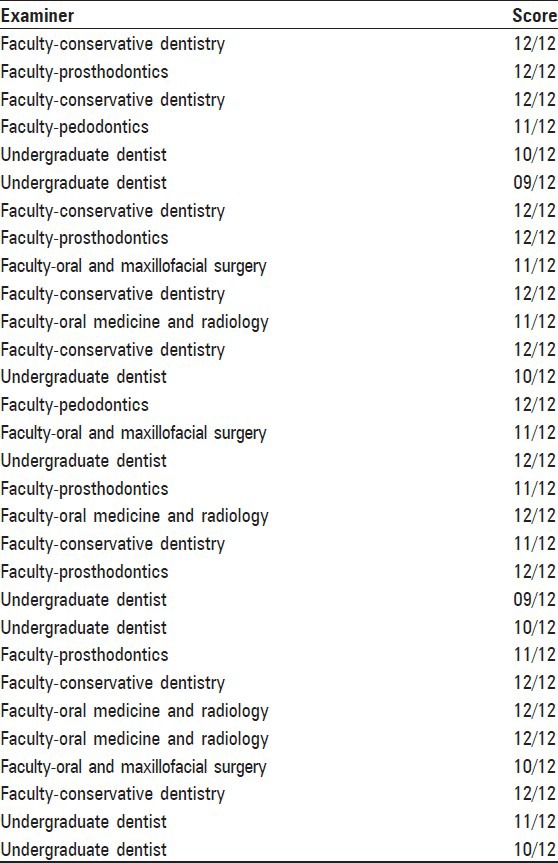
Table 1.
Correlation between SET 1 and SET 2
Thirty dentally trained professionals were requested to match the radiographic images from SET 2 with those of SET 1. Each examiner viewed the radiographs on their own without consulting anyone else. The success rate of each examiner was recorded. The examiners were as follows: Eight faculty members from the Department of Conservative Dentistry,five faculty members from the Department of Prosthodontics,two faculty members from the Department of Pedodontics, four faculty members from the Department of Oral Medicine and Radiology, three faculty members from the Department of Oral and Maxillofacial Surgery, and eight dentists with undergraduate degree.
The results were statistically analyzed using kappa statistical test.
Results
The result given by each and every examiner was documented by recording the number of exact matches between SET 1 and SET 2 [Table 2].
Table 2.
Scores of the 30 examiners
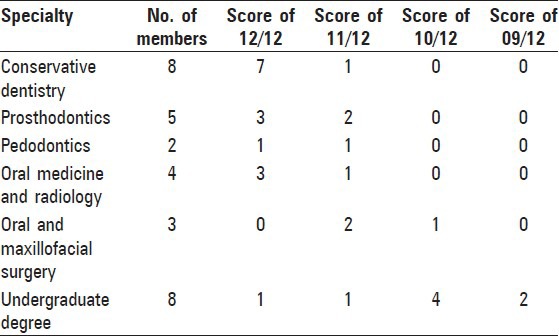
The scores of the examiners according to their specialty were separately tabulated [Table 3].
Table 3.
Scores of the examiners according to specialty
The results show that out of the 30 examiners, 15 examiners scored 12/12, 8 examiners scored 11/12, 5 examiners scored 10/12, and 2 examiners scored 9/12.
The scores were statistically analyzed using kappa statistical test for inter-examiner consistency and the result of the analysis was 0.83.
Discussion
Several studies are available in literature regarding the use of dental restorations for identification purposes.[27,28,29,30] In recent times, there has been an increase in demand for esthetic restorations among the patients, resulting in an increasing number of composite restorations over amalgam restorations. A variety of composite resins are available in the market, each having varying degree of radiopacity. The radiopacity of a composite restoration is an important property which helps in assessment of marginal overhangs, open gingival margins, interproximal caries, and recurrent caries. The radiopacity of composites also plays a significant role in forensic dentistry as it is very important for identification purposes.[31,32,33] In this study, the composite brand Tetric N-Ceram was used which has a radiopacity of 400% aluminum.[34,35]
The results show that out of the 30 dentally trained examiners, 15 were able to match all the 12 images correctly in spite of the presence of two random radiographs, i.e., success rate of 100%, 8 were able to match 11 images correctly, i.e., success rate of 91.66%, 5 were able to match 10 images correctly, i.e., success rate of 83.33%.
The results were statistically analyzed using kappa statistical test for agreement between examiners, giving a value of 0.83 which denotes very good agreement.
The results show that the discriminatory characteristic of a radiographic image of a two-surface composite restoration is unique and could be used for identification purposes, when ante-mortem and post-mortem X-ray images are identical.
The 30 examiners in this study were selected at random from various specialties and also included undergraduate dentists. Examiners were not equally selected from each specialty since the objective of this study did not include the comparing ability of examiners from one specialty being better than the other. The objective also did not include comparison of undergraduate examiners with post-graduate examiners. Although it was not the aim of this study to evaluate the differences between the examiners from different departments, the results are shown in a separate table [Table 3]. Table 3 shows that there is a tendency for dentists, who restore the tooth (restorative dentists) and who evaluate the status of the tooth (oral physicians), to match the radiographs better.
Consultations among examiners were not allowed in this study though in real life it is possible. None of the examiners were trained in forensic dentistry and so did not have the knowledge of the criticality of false-positive identification. Hence, many did not report about the two radiographs in SET 2 which did not have a match. If consultations were allowed, more examiners would have given a full score. If the examiners were given an option to report uncertainty (with “not sure”), then it would also have affected the results positively or negatively.
The examiners had to match the radiographs by analyzing the radiographic appearance of the composite restoration alone and not that of the teeth. Typodont teeth are easily available and their use in this study standardizes the morphology of the teeth and decreases the variability in their radiographic appearance. Natural teeth would have given a more challenging comparison, but would have contributed to variability in their radiographic appearance.
According to Kieser-Nielson, the restored tooth surface as seen in the radiograph should be regarded as the smallest unit to consider in the comparison of dental restorations for identification purposes. Even a single avulsed tooth collected from the scene of disaster may form the only evidence to the presence of a missing person in the scene. Hence, the validity of this study of a restoration in a single tooth is high.
Conclusion
If the post-mortem radiographs are accurate duplicates of ante-mortem radiographs of composite restorations, then the shape of the composite restoration is unique and the radiographic image can be used for successful identification.
This preliminary investigation was carried out with the radiographs taken with absolute standardization. In real life such exact ante-mortem and post-mortem radiographs may not be possible due to factors like wear and fracture of the restoration, change in dentition and radiological errors. Further research can be done by conducting similar studies in patients with long-standing composite restorations which will mimic real-life situation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Pretty IA, Sweet D. A look at forensic dentistry–Part 1: The role of teeth in the determination of human identity. Br Dent J. 2001;190:359–66. doi: 10.1038/sj.bdj.4800972. [DOI] [PubMed] [Google Scholar]
- 2.Keiser-Nielsen S. Bristol: John Wright and Sons; 1980. The final report. Person Identification by Means of their Teeth; pp. 54–72. [Google Scholar]
- 3.Jain AK, Chen H. Matching of dental X-ray images for human identification. Pattern Recogn. 2004;37:1519–32. [Google Scholar]
- 4.Buchner A. The identification of human remains. Int Dent J. 1985;35:307–11. [PubMed] [Google Scholar]
- 5.Phillips VM, Scheepers CF. Comparison between fingerprint and dental concordant characteristics. J Forensic Odontostomatol. 1990;8:17–9. [PubMed] [Google Scholar]
- 6.Adams BJ. Establishing personal identification based on specific patterns of missing, filled, and unrestored teeth. J Forensic Sci. 2003;48:487–96. [PubMed] [Google Scholar]
- 7.Stimson PG. Radiology in forensic odontology. Dent Radiogr Photogr. 1975;48:51–5. [PubMed] [Google Scholar]
- 8.Luntz LL, Luntz P. Handbook for Dental Identification. Philadelphia: J.B.Lippincott Company; 1973. Antemortem records. [Google Scholar]
- 9.Sognnaes RF. Dental evidence in the postmortem identification of Adolf Hitler, Eva Braun, and Martin Bormann. Leg Med Annu. 1977;1976:173–235. [PubMed] [Google Scholar]
- 10.Keiser-Nielsen S. Dental identification: Certainty V probability. Forensic Sci. 1977;9:87–97. doi: 10.1016/0300-9432(77)90073-5. [DOI] [PubMed] [Google Scholar]
- 11.de Villiers CJ, Phillips VM. Person identification by means of a single unique dental feature. J Forensic Odontostomatol. 1998;16:17–9. [PubMed] [Google Scholar]
- 12.Phillips VM. The uniqueness of amalgam restorations for identification. J Forensic Odontostomatol. 1983;1:33–8. [PubMed] [Google Scholar]
- 13.Borrman H, Gröndahl HG. Accuracy in establishing identity by means of intraoral radiographs. J Forensic Odontostomatol. 1990;8:31–6. [PubMed] [Google Scholar]
- 14.Phillips VM, Stuhlinger M. The discrimination potential of amalgam restorations for identification: Part 1. J Forensic Odontostomatol. 2009;27:17–22. [PubMed] [Google Scholar]
- 15.Zondag H, Phillips VM. The discrimination potential of radio-opaque composite restorations for identification: Part 3. J Forensic Odontostomatol. 2009;27:27–32. [PubMed] [Google Scholar]
- 16.American Dental Association. Obstacles to the development of a standard for posterior composite resins. Council on Dental Materials, Instruments, and Equipment. J Am Dent Assoc. 1989;118:649–51. doi: 10.14219/jada.archive.1989.0070. [DOI] [PubMed] [Google Scholar]
- 17.Stanford CM, Fan PL, Schoenfeld CM, Knoeppel R, Stanford JW. Radiopacity of light-cured posterior composite resins. J Am Dent Assoc. 1987;115:722–4. doi: 10.14219/jada.archive.1987.0308. [DOI] [PubMed] [Google Scholar]
- 18.Espelid I, Tveit AB, Erickson RL, Keck SC, Glasspoole EA. Radiopacity of restorations and detection of secondary caries. Dent Mater. 1991;7:114–7. doi: 10.1016/0109-5641(91)90056-5. [DOI] [PubMed] [Google Scholar]
- 19.Curtis PM, Jr, von Fraunhofer JA, Farman AG. The radiographic density of composite restorative resins. Oral Surg Oral Med Oral Pathol. 1990;70:226–30. doi: 10.1016/0030-4220(90)90124-b. [DOI] [PubMed] [Google Scholar]
- 20.Goshima T, Goshima Y. Radiographic detection of recurrent carious lesions associated with composite restorations. Oral Surg Oral Med Oral Pathol. 1990;70:236–9. doi: 10.1016/0030-4220(90)90126-d. [DOI] [PubMed] [Google Scholar]
- 21.Tveit AB, Espelid I. Radiographic diagnosis of caries and marginal defects in connection with radiopaque composite fillings. Dent Mater. 1986;2:159–62. doi: 10.1016/s0109-5641(86)80027-6. [DOI] [PubMed] [Google Scholar]
- 22.Bouschlicher MR, Cobb DS, Boyer DB. Radiopacity of compomers, flowable and conventional resin composites for posterior restorations. Oper Dent. 1999;24:20–5. [PubMed] [Google Scholar]
- 23.Willems G, Noack MJ, Inokoshi S, Lambrechts P, Van Meerbeek B, Braem M, et al. Radiopacity of composites compared with human enamel and dentine. J Dent. 1991;19:362–5. doi: 10.1016/0300-5712(91)90056-5. [DOI] [PubMed] [Google Scholar]
- 24.Hara AT, Serra MC, Haiter-Neto F, Rodrigues AL., Jr Radiopacity of esthetic restorative materials compared with human tooth structure. Am J Dent. 2001;14:383–6. [PubMed] [Google Scholar]
- 25.Imperiano MT, Khoury HJ, Pontual MA, Montes MJ, da Silveira MF. Comparative radiopacity of four low viscosity composites. Braz J Oral Sci. 2007;6:1278–82. [Google Scholar]
- 26.Cruvinel DR, Garcia LF, Casemiro LA, Pardini LC, Pires-de-Souza FC. Evaluation of radiopacity and microhardness of composites submitted to artificial aging. Mater Res. 2007;10:325–9. [Google Scholar]
- 27.Pretty IA, Smith PW, Edgar WM, Higham SM. The use of quantitative light-induced fluorescence (QLF) to identify composite restorations in forensic examinations. J Forensic Sci. 2002;47:831–6. [PubMed] [Google Scholar]
- 28.Benthaus S, DuChesne A, Brinkmann B. A new technique for the postmortem detection of tooth-coloured dental restorations. Int J Legal Med. 1998;111:157–9. doi: 10.1007/s004140050138. [DOI] [PubMed] [Google Scholar]
- 29.Hermanson AS, Bush MA, Miller RG, Bush PJ. Ultraviolet illumination as an adjunctive aid in dental inspection. J Forensic Sci. 2008;53:408–11. doi: 10.1111/j.1556-4029.2008.00657.x. [DOI] [PubMed] [Google Scholar]
- 30.Bush MA, Bush PJ, Miller RG. Detection and classification of composite resins in incinerated teeth for forensic purposes. J Forensic Sci. 2006;51:636–42. doi: 10.1111/j.1556-4029.2006.00121.x. [DOI] [PubMed] [Google Scholar]
- 31.Turgut MD, Attar N, Onen A. Radiopacity of direct esthetic restorative materials. Oper Dent. 2003;28:508–14. [PubMed] [Google Scholar]
- 32.Salzedas LM, Louzada MJ, de Oliveira Filho AB. Radiopacity of restorative materials using digital images. J Appl Oral Sci. 2006;14:147–52. doi: 10.1590/S1678-77572006000200015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wenzel A, Hintze H, Hørsted-Bindslev P. Discrimination between restorative dental materials by their radiopacity measured in film radiographs and digital images. J Forensic Odontostomatol. 1998;16:8–13. [PubMed] [Google Scholar]
- 34.Mahn E. The renaissance of a classic: Tetric-N Ceram-a perfect combination of experience and innovation. [Last Cited on 2012 Mar 03]. Available from: htp://www.dental-tribune.com/articles/specialities/cosmetic_dentistry/162_the_renaissance_of_a_classic_tetric-n_cerama_perfect_combination_of_experience_and_innovation.html .
- 35.Dukic W, Delija B, Derossi D, Dadic I. Radiopacity of composite dental materials using a digital X-ray system. Dent Mater J. 2012;31:47–53. doi: 10.4012/dmj.2011-119. [DOI] [PubMed] [Google Scholar]