

Abstract
Objectives
This study aims to examine the effectiveness of a 6-month lifestyle modification program on the improvement in metabolic syndrome (MetS) status and in stages of change for lifestyle behaviors associated with MetS among Korean older adults.
Methods
A lifestyle modification program was developed based on the transtheoretical model. The program consisted of health counseling, education classes, a self-management handbook, newsletters and a health diary. Older adults aged ≥60 (n = 480) with MetS were randomly assigned to the intervention group (IG) or the comparison group (CG). The IG received a comprehensive 6-month lifestyle modification intervention, while the CG received minimal information on MetS and lifestyle modification. Health examination and selfadministered survey were conducted before and after the intervention to determine the effectiveness of the program.
Results
After the intervention, the prevalence of MetS decreased to 38.1% in the IG and 52.4% in the CG (p = 0.046). The IG improved abdominal obesity (p = 0.016), blood pressure (p = 0.030), and triglyceride (p = 0.005) more than the CG did. The IG demonstrated significant improvements in the behavioral stages for portion control (p = 0.021), balanced diet (p < 0.001) and adequate intake of fruits and vegetables (p = 0.012). The IG reduced the prevalence of abdominal obesity (OR = 2.34) and improved MetS status (OR = 1.79) better than the CG. The IG were more likely to advance from preaction stages at baseline to action stage at post-intervention for portion control (OR = 3.29) and adequate intake of fruits and vegetables (OR = 2.06).
Conclusion
Lifestyle modification can improve the MetS status and behavioral stages in older adults.
Keywords: health behaviors, lifestyle change intervention, metabolic syndrome, older adults, stages of change
1. Introduction
Metabolic cardiovascular risk factors are significant predictors of cardiac events in old age [1,2], and concurrence of a number of metabolic cardiovascular risk factors is more common in older adults [3]. Metabolic syndrome (MetS) refers to a cluster of concurrent metabolic cardiovascular risk factors. According to the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP ATP III), MetS is defined as having three or more of the following: abdominal obesity, elevated blood pressure, impaired fasting glucose, elevated triglyceride, and decreased highdensity lipoprotein (HDL) cholesterol level [4]. MetS is associated with increased risk of cardiovascular disease (CVD) and type 2 diabetes [5], particularly with an increased CVD-related morbidity and mortality even when CVD or diabetes does not exist clinically [6,7].
MetS is increasing worldwide including Asia [4,8]. Asians tend to have higher risk of type 2 diabetes and CVD even at lower body mass index (BMI) than Caucasians [9]. The age-adjusted prevalence of MetS in South Korea (Korea hereafter) among Korean adults aged ≥20 years, using the NCEP ATP III definition based on the Korean National Health and Nutrition Examination Surveys, increased consistently and significantly from 24.9% in 1998 to 31.3% in 2007 [8], compared to 34.0% in the USA, 2003-2006 [10]. The prevalence is greater in older adults [6,8].
Lifestyle modification intervention especially targeting diet and physical activity is instrumental and necessary for reducing the prevalence of MetS [4,11,12]. Healthy diet and regular physical activity are essential in the lifestyle modification for MetS management [13,14]. The transtheoretical model (TTM) has often been employed as a framework for interventions for healthy diet and physical activity [15]. However, application of TTM to improve diet and physical activity has been limited in MetS studies in Korea until recently [16,17]. The stages of change (SOC) construct in the TTM emphasizes behavioral change as a process that involves adopting the new behavior and acting on it. The SOC postulates behavior change as a dynamic process consisted of mutually exclusive stages of readiness: precontemplation (not considering change), contemplation (considering change), preparation (decided to take action in the next month), action (changed behavior in the past 6 months), and maintenance (maintained the changed behavior for longer than 6 months) [18]. The assessment of SOC can guide an intervention to identify behavioral readiness and intention for change and to develop effective processes for behavioral change [19]. SOC are, in fact, a predictor of actual behavior such as dietary intake [18]. This study aims to examine the changes in MetS status in Korean older adults after a 6- month health education intervention program along with the improvement in behavioral stages from nonaction to action for lifestyle behaviors associated with MetS.
2. Materials and Methods
2.1. Intervention
A 6-month lifestyle change program was developed to control MetS through increasing physical activity, improving diet, and reducing weight. TTM is applied to our program to provide different intervention strategies to the older adults according to their SOC (precontemplation, contemplation or preparation, and action or maintenance [20]. Participants were encouraged to enhance MetS-related knowledge (definition, prevalence and trends, causes, and consequences of MetS) and life skills for hypocaloric, balanced diet, moderate drinking, and adequate level of physical activity [21]. Cognitive and behavioral strategies included consciousness raising, enhancing pros of lifestyle change and self efficacy, goal setting for behavior change, regular selfmonitoring of progress, and providing rewards to promote the movement from stage to stage and to reinforce healthy lifestyle (Table 1).
Table 1.
TTM-based cognitive and behavioral intervention strategies
| SOC | Methods | Strategies |
|---|---|---|
| PC | Consciousness raising | - Determine participants’ perceptions of the severity of MetS |
| Outcome expectation | - Provide personal feedback on the severity of MetS and related health behavior problems | |
| - Provide MetS related knowledge | ||
| - Provide information on the benefits of changing health behavior patterns to manage MetS | ||
| C/PR | Decisional balance (pros and cons) | - Explain the benefits of changing health behaviors in details |
| Modeling | - Counteract barriers to change with salient benefits | |
| Self-efficacy | - Provide observational learning opportunity through modeling | |
| Self-liberation | - Teach how-to information and skills for health behavior change | |
| Goal setting | - Sign commitment form | |
| - Set the reasonable and specific goals | ||
| A/M | Self-monitoring | - Self -monitor diet, activity and other health behaviors |
| Stimulus control | - Provide relapse prevention strategies | |
| Reinforcement management | - Provide reminders to engage healthy behaviors | |
| - Modify undesirable attribution | ||
| - Provide rewards for the completion of the study | ||
TTM = transtheoretical model; SOC = stages of change; MetS = metabolic syndrome; PC = precontemplation stage; C/PR = contemplation or preparation stage; A/M = action or maintenance stage.
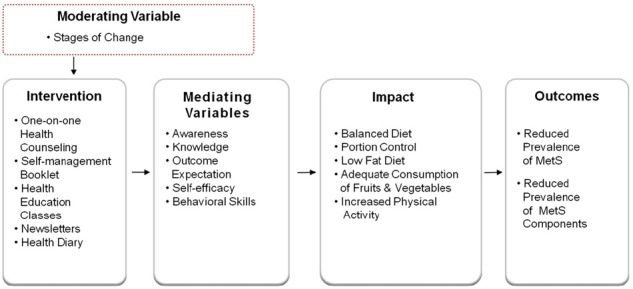
The intervention composed of individual counseling sessions with registered dietitians, health education classes, educational newsletters and booklets, and keeping a health diary. One-on-one health counseling was provided every other week, by telephone when faceto- face counseling was not possible. A booklet and a health diary were provided to those in the intervention group as health education material and also as a selfmonitoring tool. In addition to individual counseling, the intervention group members were invited to two health classes on prevention and management of hypertension, diabetes, obesity, and MetS. Monthly newsletters on healthy lifestyle were sent to the intervention group members (Figure 2). The comparison group, in contrast, was provided with their MetS status and a one-page health information sheet on MetS at baseline.
Figure 2. Logic model of the lifestyle change program.
2.2. Participants and recruitment
The participants were 430 adults aged 60 and older who were diagnosed with MetS after completing health examinations at one of 15 regional branch medical facilities of the Korea Association of Health Promotion (KAHP) between June 1, 2008 and April 30, 2009. MetS is defined by the NCEP ATP III criteria for MetS [4] and the Asia-Pacific standard for abdominal obesity [22]. That is, older adults who meet three or more of the following five conditions are classified as having MetS: (1) waist circumference >90 cm for men or >80 cm for women; (2) HDL cholesterol <40 mg/dL for men or <50 mg/dL for women; (3) triglyceride ≥150 mg/dL; (4) systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg; and (5) fasting glucose
≥100 mg/dL. Exclusion criteria for the study were: being on medication for weight control; having been diagnosed with diabetes or hypertension; being on treatment for MetS; and not providing signed consent form for participation in the study.
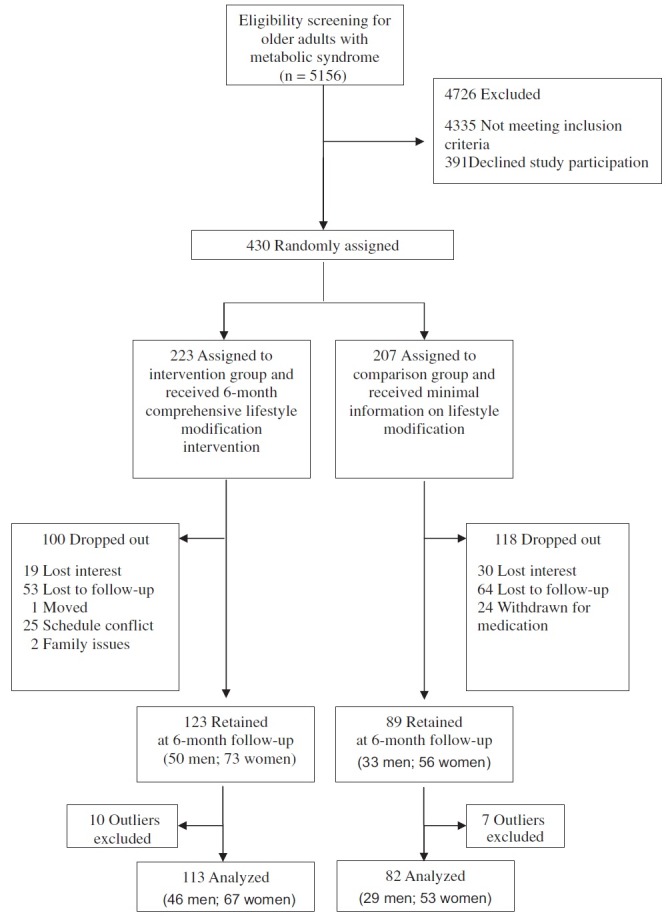
Of 5156 older adults identified with MetS, 821 met the eligibility criteria. Among those, 391 refused to participate in the study. The remaining 430 older adults who agreed with and were eligible for the intervention were randomly assigned to either the intervention group (IG) or the comparison group (CG). Participants in the IG received the aforementioned comprehensive 6-month lifestyle change intervention and the CG received minimal information on the MetS and lifestyle modification. During the study, 100 and 118 participants dropped out from IG and CG, respectively. The reasons for dropping out were described in Figure 1. The final analyses included 113 participants in IG and 82 in CG (Figure 1). This study was reviewed and approved by Institutional Review Board of the KAHP (# 09-B-04).
Figure 1. Flow of participants through the 6-month intervention.
2.3. Data collection
Height, weight, BMI and five components of MetS of all study participants were measured at baseline and postintervention (6 months from the baseline). Both height and weight were measured using the Fatness Measuring System (DS-102, Dong Sahn Jenix, Seoul, Korea). Weight was measured in the morning before breakfast, with participants in a T-shirt and shorts without shoes. BMI was calculated as the weight in kilograms divided by the square of height in meters. Waist circumference was measured at a level midway between the lowest rib and the iliac crest. Fasting blood samples were drawn before and after the intervention. The blood was separated by centrifugation and analyzed at the KAHP laboratories. Triglycerides, HDL cholesterol and fasting glucose levels were measured using HITACHI 7600-110 (HITACHI, Tokyo, Japan). Blood pressure was measured with an automatic digital sphygmomanometer (TM- 2655P; A&D, Tokyo, Japan). Measurements were made after participants had been seated quietly for at least 5 min in a chair with feet on the floor and arm supported at heart level. Classification of blood pressure is based upon the average of two or more readings on two or more occasions separated by at least 2 min.
SOC of the participants for health behaviors related to MetS were assessed through a self-administered questionnaire. The questionnaire was based on the multi-item algorithm of SOC (M-SOC) developed by Sutton et al [23]. It included four categories of dietary behavior: decreasing portion size, eating balanced diet and adequate amount of fruits and vegetables, and lowering fat consumption, and also included an item on daily physical activities. Cronbach α ranged from 0.686 for physical activity to 0.795 for portion control.
2.4. Analysis
Using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), independent-samples t test and chi-square test were performed to examine differences between the IG and CG at baseline. McNemar and Pearson chi-square tests were applied to analyze within-group and between-group differences in SOC distribution of health behaviors and prevalence data at baseline and 6 months. The odds ratio effect sizes were calculated to investigate
improvement in health behaviors and prevalence of MetS in the IG relative to the CG.
3. Results
3.1. Baseline characteristics
The IG and CG were similar in demographic composition, health status, and health behaviors overall at baseline (Table 2). More than a third of the participants were male, and the mean ± SD age of the participants was 65.68 ± 3.38 years for the IG and 65.73 ± 4.07 years for the CG. All patients in both groups had MetS at baseline, with BMI of 25.87 ± 2.36 kg/m2 in the IG and 26.12 ± 2.36 kg/m2 in the CG. In both IG and CG, more than half of the participants practiced balanced diet, but the prevalence of other health behaviors such as portion control, low fat diet, adequate intake of fruits and vegetables, and physical activity was relatively lower, respectively. Meanwhile, behavioral stages at baseline differed between the groups in low fat diet and physical
Table 2.
Baseline characteristics of the 6-month participants
| Characteristics | Intervention Group (n = 113) | Comparison Group (n = 82) | pa |
|---|---|---|---|
| Demographics | |||
| Male, n (%) | 46 (40.7) | 29 (35.4) | 0.449 |
| Age, yrs, mean(SD) | 65.68 (3.38) | 65.73 (4.07) | 0.839 |
| 60-64, yrs, n (%) | 42 (37.2) | 36 (43.9) | 0.068 |
| 65-69, yrs, n (%) | 61 (54.0) | 32 (39.0) | |
| + 70, yrs, n (%) | 10 (8.8) | 14 (17.1) | |
| Health outcomes | |||
| Weight, kg, mean(SD) | 65.68 (9.71) | 65.17 (9.28) | 0.712 |
| BMI, kg/m2, mean(SD) | 25.87 (2.36) | 26.12 (2.36) | 0.474 |
| Abdominal obesity, n (%) | 94 (83.2) | 69 (84.1) | 0.858 |
| High SBP, n (%) | 75 (66.4) | 56 (68.3) | 0.778 |
| High DBP, n (%) | 45 (39.8) | 21 (25.6) | 0.038 |
| High Blood pressure, n (%) | 84 (74.3) | 58 (70.7) | 0.576 |
| High TG, n (%) | 86 (76.1) | 61 (74.4) | 0.784 |
| Low HDL-C, n (%) | 69 (61.1) | 49 (59.8) | 0.854 |
| High FBG, n (%) | 57 (50.4) | 51 (62.7) | 0.103 |
| Health Behaviors | |||
| Portion control, n (%) | 16 (14.5) | 11 (13.6) | 0.850 |
| Balanced diet, n (%) | 61 (55.5) | 43 (53.8) | 0.816 |
| Low fat diet, n (%) | 13 (11.9) | 10 (12.5) | 0.905 |
| Fruit and vegetable intake, n (%) | 20 (18.0) | 18 (22.0) | 0.497 |
| Physical activity, n (%) | 10 (8.9) | 3 (3.7) | 0.147 |
aChi-square test or independent t test.
BMI = body mass index; WC = waist circumference; SBP = systolic blood pressure; DBP = diastolic blood pressure; TG = triglyceride; HDLC = high-density lipoprotein cholesterol; FBG = fasting blood glucose; MetS = metabolic syndrome.
activity: more in the IG were in the contemplation and preparation stages and fewer were in the precontemplation stage for both behaviors, compared to the CG group (Table 3).
Table 3.
Distributions of participants across the three stages of health behavior change before and after the intervention
| Intervention Group | Comparison Group | Between group difference at baseline | Between group difference at 6 month | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 month | Change | pa | Baseline | 6 month | Change | pa | pb | pb | |
| n (%) | n (%) | % | n (%) | n (%) | % | |||||
| Portion control | 0.933 | 0.021 | ||||||||
| PC | 8 (7.3) | 7 (7.1) | –0.2 | 1.000 | 5 (6.2) | 6 (7.4) | 1.2 | 1.000 | ||
| C/PR | 86 (78.2) | 56 (57.1) | –21.1 | <0.001 | 65 (80.2) | 61 (75.3) | –4.9 | 0.523 | ||
| A/M | 16 (14.5) | 35 (35.7) | 21.2 | 0.003 | 11 (13.6) | 14 (17.3) | 3.7 | 0.581 | 0.882c | 0.027c |
| n | 110 (100.0) | 98 (100.0) | 81 (100.0) | 81 (100.0) | ||||||
| Balanced diet | 0.713 | <0.001 | ||||||||
| PC | 3 (2.7) | 7 (7.1) | 4.4 | 0.344 | 4 (5.0) | 2 (2.4) | –2.6 | 0.687 | ||
| C/PR | 46 (41.8) | 19 (19.2) | –22.6 | <0.001 | 33 (41.3) | 41 (50.0) | 8.7 | 0.280 | ||
| A/M | 61 (55.5) | 73 (73.7) | 18.2 | 0.162 | 43 (53.8) | 39 (47.6) | –6.2 | 0.643 | 0.831c | 0.018c |
| n | 110 (100.0) | 99 (100.0) | 80 (100.0) | 82 (100.0) | ||||||
| Low fat diet | <0.001 | 0.061 | ||||||||
| PC | 5 (4.6) | 16 (16.3) | 11.7 | 0.027 | 25 (31.3) | 20 (24.4) | –6.9 | 0.458 | ||
| C/PR | 91 (83.5) | 51 (52.0) | –31.5 | <0.001 | 45 (56.3) | 48 (58.5) | 2.2 | 0.760 | ||
| A/M | 13 (11.9) | 31 (31.6) | 19.7 | 0.003 | 10 (12.5) | 14 (17.1) | 4.6 | 0.481 | 0.883c | 0.090c |
| n | 109 (100.0) | 98 (100.0) | 80 (100.0) | 82 (100.0) | ||||||
| Fruit and vegetable intake | 0.390 | 0.012 | ||||||||
| PC | 0 (0.0) | 9 (9.0) | 9.0 | 0.004 | 1 (1.2) | 10 (12.2) | 11.0 | 0.012 | ||
| C/PR | 91 (82.0) | 36 (36.0) | –46.0 | <0.001 | 63 (76.8) | 45 (54.9) | –21.9 | 0.006 | ||
| A/M | 20 (18.0) | 55 (55.0) | 37.0 | <0.001 | 18 (22.0) | 27 (32.9) | 10.9 | 0.151 | 0.459c | 0.028c |
| n | 111 (100.0) | 100 (100.0) | 82 (100.0) | 82 (100.0) | ||||||
| Physical activity | <0.001 | 0.066 | ||||||||
| PC | 14 (12.5) | 12 (12.1) | –0.4 | 0.832 | 39 (47.6) | 18 (22.0) | –25.6 | <0.001 | ||
| C/PR | 88 (78.6) | 66 (66.7) | –11.9 | 0.002 | 40 (48.8) | 55 (67.1) | 18.3 | 0.025 | ||
| A/M | 10 (8.9) | 21 (21.2) | 12.3 | 0.019 | 3 (3.7) | 9 (11.0) | 7.3 | 0.109 | 0.151c | 0.140c |
| n | 112 (100.0) | 99 (100.0) | 82 (100.0) | 82 (100.0) | ||||||
aMcNemar test; bChi-square test for overall differences; cChi-square test for between group differences in A/M stage.
PC = precontemplation stage; C/PR = contemplation and preparation stage; A/M = action and maintenance stage; MetS = metabolic syndrome.
3.2. Changes in the behavioral stages and metabolic syndrome prevalence
After the intervention, the prevalence of MetS decreased to 38.1% in IG and 52.4% in CG (p = 0.046). (Figure 3). More specifically, IG improved abdominal
Figure 3. Changes in metabolic syndrome prevalence among participants. a Chi-square test. MetS = metabolic syndrome; SBP = systolic blood pressure; DBP = diastolic blood pressure; BP = blood pressure; TG = triglyceride; HDL-C = high density lipoprotein cholesterol; FBG = fasting blood glucose.

obesity (–22.1%), blood pressure (–28.3%), triglyceride (–35.4%) more than CG did. Along with the changes in MetS status, significant improvements in the behavioral change stages were observed in the IG versus CG in 6 months for portion control, balanced diet, and adequate intake of fruits and vegetables. The number of participants in the IG increased significantly in the action/maintenance stages from baseline to postintervention for portion control (+21.2%, p = 0.003), low fat diet (+19.7%, p = 0.003), adequate intake of fruits and vegetables
(+37.0%, p < 0.001), and physical activity (+12.3%, p = 0.019), respectively (Table 3). At the same time, the IG reduced the number of participants in the contemplation/preparation stage in 6 months for all 5 behavior categories. In contrast, significant improvement in behavioral stages in the CG was observed only for physical activity where the proportion of participants in the precontemplation stage decreased and those in the contemplation stage increased significantly. However, for adequate intake of fruits and vegetables, the number of participants in the CG increased in the precontemplation stage and decreased in the contemplation/preparation stage after the intervention.
3.3. Desirable changes in the health status and behaviors
Table 4 presents changes from abnormal health status or preaction stage for health behavior at baseline to normal health status or action stage for health behavior at postintervention. Compared to the CG, the IG reduced waist circumference significantly (OR effect size = 2.34, 95% CI = 1.12, 3.55), experienced marginal reduction of triglyceride (OR effect size = 1.86, 95% CI = 0.99, 2.72) and improved MetS status more than the CG (OR effect size = 1.79, 95% CI = 1.07, 2.52). Similarly for health behaviors, the IG improved portion control (OR effect size = 3.29, 95% CI = 1.36, 5.21), and adequate intake of fruits and vegetables (OR effect size = 2.06, 95% CI = 1.11, 3.01) significantly more than the CG from preaction stage at baseline to action stage at postintervention.
Table 4.
Improvement in health outcomes and behaviors between groups
| Intervention Group | Comparison Group | pa | Odds ratio effect size (95% CI) | |||
|---|---|---|---|---|---|---|
| n | n (%) | n | n (%) | |||
| Health outcomes | Abnormal | Normalized | Abnormal | Normalized | ||
| WC | 94 | 31 (33.0) | 69 | 12 (17.4) | 0.033 | 2.34 (1.12, 3.55) |
| SBP | 75 | 38 (50.7) | 56 | 21 (37.5) | 0.229 | 1.71 (0.87, 2.55) |
| DBP | 45 | 28 (62.2) | 21 | 12 (57.1) | 0.083 | 1.24 (0.37, 2.10) |
| Blood pressure | 84 | 39 (46.4) | 58 | 21 (36.2) | 0.210 | 1.53 (0.80, 2.25) |
| TG | 86 | 44 (51.2) | 61 | 22 (36.1) | 0.078 | 1.86 (0.99, 2.72) |
| HDL-C | 69 | 41 (59.4) | 49 | 29 (59.2) | 0.895 | 1.01 (0.49, 1.53) |
| Fasting glucose | 57 | 17 (29.8) | 51 | 20 (39.2) | 0.100 | 0.66 (0.29, 1.03) |
| Metabolic syndrome | 113 | 70 (61.9) | 82 | 39 (47.6) | 0.046 | 1.79 (1.07, 2.52) |
| Health Behaviors | Preaction | Action | Preaction | Action | ||
| Portion control | 94 | 28 (29.8) | 70 | 8 (11.4) | 0.008 | 3.29 (1.36, 5.21) |
| Balanced diet | 49 | 35 (71.4) | 37 | 18 (48.6) | 0.162 | 2.64 (0.97, 4.30) |
| Low fat diet | 96 | 24 (25.0) | 70 | 11 (15.7) | 0.160 | 1.79 (0.81, 2.76) |
| Fruit & vegetable intake | 91 | 44 (48.4) | 64 | 20 (31.3) | 0.033 | 2.06 (1.11, 3.01) |
| Physical activity | 102 | 15 (14.7) | 79 | 8 (10.1) | 0.452 | 1.53 (0.56, 2.50) |
aChi-square test.
WC = waist circumference; SBP = systolic blood pressure; DBP = diastolic blood pressure; TG = triglyceride; HDL-C = high density lipoprotein cholesterol; FBG = fasting blood glucose; MetS = metabolic syndrome.
4. Discussion and Conclusion
This is one of few experimental studies on MetS intervention, to our knowledge, for Korean older adults in multiple regions in Korea that applied TTM constructs. Recent literature on MetS studies based on the TTM framework was a cross-sectional survey study with a focus on exercise behavior [16], or conducted with a smaller number of middle-aged Koreans with MetS and type 2 diabetes in a 16-week intervention [24]. Our study presents a case in which older adults could improve their MetS status by modifying lifestyle behaviors despite the belief that health behaviors in old age are so embedded in lifestyle that they are difficult to change [25]. In fact, Villareal et al [3] argued that older adults are sufficiently compliant with lifestyle modification intervention to accomplish lifestyle-induced weight loss that is comparable to young and middle-aged adults. It is of note that the older adults in our study demonstrated psychobehavioral changes and improvement in MetS prevalence without medical treatment. Recruited participants of this study were those in predisease stage for any of the MetS components, and none were taking medications or under treatment for cardiometabolic conditions.
Reduction of MetS prevalence was more prominent in IG in which fewer participants remained thinking about changing behaviors (contemplation/preparation stage) and significantly more participants advanced to the action/maintenance stage for dietary behaviors in 6 months. Although the CG also improved their MetS status and some lifestyle behaviors with minimal intervention by being informed about their MetS status and receiving a one-page health education leaflet on MetS, the amount of change in the MetS prevalence was smaller and the behavior change did not occur in the action/maintenance stage in the CG. Increase in the proportion of participants in the action/maintenance stage occurred only in the IG. For low fat diet and physical activity, respectively, more participants were in the contemplation/preparation stage in the IG at baseline; therefore they might have been more ready to practice the healthy behavior and to transition to the action/maintenance stage than those in CG. However, the number in the precontemplation subgroup decrease and the size of the contemplation/preparation subgroup did not increase in the CG for low fat diet, let alone transitioning to the action/maintenance stage. For physical activity, on the other hand, a significant number of older adults in the CG moved from the precontemplation to contemplation/preparation stages although not many advanced to the action/maintenance stage. Selfawareness of the MetS status might have influenced the intention of the older adults in the CG to be physically active in everyday life. Johnson et al [26] maintain that pretest and post-test assessments of SOC and health status performed in interventions might inform and influence those in the CG to change. However, the dietary behavior changes may require more specific knowledge and skills, and the IG, who had regular encounters with and reinforcement from dietitians, demonstrated greater improvement in dietary behaviors and MetS prevalence.
The TTM and SOC postulate that behavioral change is a temporal dimension and thus occurs as a process [19]. The SOC in the TTM also indicate that action is not an event but a process in which regression can occur. Our results corroborate such a notion by showing that the number of participants increased in the precontemplation stage or decreased in the action/maintenance stage in certain behaviors in 6 months. It also draws attention to the need for follow-up lifestyle management and care to reinforce continued action and to prevent from relapsing to earlier behavior stages.
This study does not include socioeconomic status information of the participants, measurement of dietary caloric intake, or assessment of the types, intensity, and frequency of physical activity, and thus is limited in its explanative capacity. The volume of dropouts in this study calls for program monitoring. Another issue of discussion is that SOC is an essential but not the only construct of the TTM. This study is narrow in the TTM scope by leaving out other constructs of the TTM such as the processes of change, decisional balance, and selfefficacy [27]. However, SOC is a predictor of behavioral performance [18], and our findings shows changes in the composition of the SOC in participant groups and in actual health status in a randomized controlled trial with a lifestyle modification intervention.
Despite some limitations, our randomized controlled trial study demonstrated the effectiveness of a theorybased lifestyle modification program for MetS in reducing the prevalence of MetS in older adults. This study was conducted with a relatively larger sample from multiple regions compared to previous lifestyle intervention studies on MetS in Korea. This study presents that lifestyle modification alone can improve the MetS status in older adults. It also shows that significant differences occurred in the changes in behavioral stages between the IG and CG in 6 months: more in the IG moved to the action/maintenance stage in several behavior categories. Further research is warranted to investigate the effects of the intervention program in younger adults with MetS, and to incorporate other constructs of the TTM to explain the facilitation of behavioral changes by the intervention program for MetS management and control.
Acknowledgments
This study was registered in the Clinical Research Information Service by Korea Centers for Diseases Control and Prevention, Korea (# KCT 0000344).
References
- 1.Psaty BM, Furberg CD, Kuller LH, et al. Traditional risk factors and subclinical disease measures as predictors of first myocardial infarction in older adults: the Cardiovascular Health Study. Arch Intern Med. 1999 Jun;159(12):1339–47. doi: 10.1001/archinte.159.12.1339. [DOI] [PubMed] [Google Scholar]
- 2.Tervahauta M, Pekkanen J, Nissinen A. Risk factors of coronary heart disease and total mortality among elderly men with and without preexisting coronary heart disease. Finnish cohorts of the Seven Countries Study. J Am Coll Cardiol. 1995 Dec;26(7):1623–9. doi: 10.1016/0735-1097(95)00395-9. [DOI] [PubMed] [Google Scholar]
- 3.Villareal DT, Miller III BV, Banks M, et al. Effect of lifestyle intervention on metabolic coronary heart disease risk factors in obese older adults. Am J Clin Nutr. 2006 Dec;84(6):1317–23. doi: 10.1093/ajcn/84.6.1317. [DOI] [PubMed] [Google Scholar]
- 4.National Institute of Health Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive Summary of the third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001 May 16;285(19):2486–97. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 5.Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005 Apr 16-22;365(9468):1415–28. doi: 10.1016/S0140-6736(05)66378-7. [DOI] [PubMed] [Google Scholar]
- 6.Ford ES, Giles WH, Mokdad AH. Increasing prevalence of the metabolic syndrome among US adults. Diabetes Care. 2004 Oct;27(10):2444–9. doi: 10.2337/diacare.27.10.2444. [DOI] [PubMed] [Google Scholar]
- 7.Levantesi G, Macchia A, Marfisi R, et al. Metabolic syndrome and risk of cardiovascular events after myocardial infarction. J Am Coll Cardiol. 2005 Jul;46(2):277–83. doi: 10.1016/j.jacc.2005.03.062. [DOI] [PubMed] [Google Scholar]
- 8.Lim S, Shin H, Song J, et al. Increasing prevalence of metabolic syndrome in Korea. Diabetes Care. 2011 Jun;34(6):1323–8. doi: 10.2337/dc10-2109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Palaniappan LP, Wong EC, Shin JJ, et al. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int J Obes. 2011 Mar;35(3):393–400. doi: 10.1038/ijo.2010.152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ervin RB. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003-2006. National Center for Health Statistics; Hyattsville, MD: 2009. [PubMed] [Google Scholar]
- 11.Grundy SM, Hansen B, Smith Jr SC, et al. Clinical management of metabolic syndrome: report of the American Heart Association/ National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Circulation. 2004 Feb 4;109(4):551–6. doi: 10.1161/01.CIR.0000112379.88385.67. [DOI] [PubMed] [Google Scholar]
- 12.Klein S, Burke LE, Bray GA, et al. Clinical implications of obesity with specific focus on cardiovascular disease: a statement for professionals from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation. 2004 Nov 2;110(148):2952–67. doi: 10.1161/01.CIR.0000145546.97738.1E. [DOI] [PubMed] [Google Scholar]
- 13.Jakicic JM, Otto AD. Physical activity considerations for the treatment and prevention of obesity. Am J Clin Nutr. 2005 Jul;1(Suppl. 82):226S–9S. doi: 10.1093/ajcn/82.1.226S. [DOI] [PubMed] [Google Scholar]
- 14.Johannsen DL, Redman LM, Ravussin E. The role of physical activity in maintaining a reduced weight. Curr Atheroscler Rep. 2007 Dec;9(6):463–71. doi: 10.1007/s11883-007-0062-z. [DOI] [PubMed] [Google Scholar]
- 15.Kim CJ. Development of an exercise intervention program based on stages of exercise using the transtheoretical model in patients with type 2 diabetes mellitus. J Korean Acad Fundam Nurs. 2002 Apr;9(1):123–32. [Google Scholar]
- 16.Kim CJ, Kim BT, Chae SM. Application of the transtheoretical model: exercise behavior in Korean adults with metabolic syndrome. J Cardiovasc Nurs. 2010 Jul-Aug;25(4):323–31. doi: 10.1097/JCN.0b013e3181c8a3e8. [DOI] [PubMed] [Google Scholar]
- 17.Oh EG, Bang SY, Hyun SS, et al. Effects of a 6-month lifestyle modification intervention on the cardiometabolic risk factors and health-related qualities of life in women with metabolic syndrome. Metabolism. 2010 Jul;59(7):1035–43. doi: 10.1016/j.metabol.2009.10.027. [DOI] [PubMed] [Google Scholar]
- 18.Glanz K, Patterson RE, Kristal AR, et al. Stages of change in adopting healthy diets: fat, fiber, and correlates of nutrient intake. Health Educ Q. 1994;21(4):499–519. doi: 10.1177/109019819402100412. Winter. [DOI] [PubMed] [Google Scholar]
- 19.Velicer WF, Prochaska JO, Fava JL, et al. Smoking cessation and stress management: application of the transtheoretical model of behavior change. Homeost Health Dis. 1998;38(5-6):216–33. [Google Scholar]
- 20.Lippke S, Ziegelmann JP, Schwarzer R. Stage-specific adoption and maintenance of physical activity: testing a three-stage model. Psychol Sport Exerc. 2005 Sep;6(5):585–603. [Google Scholar]
- 21.Dalle Grave R, Calugi S, Centis E, et al. Lifestyle modification in the management of the metabolic syndrome: achievements and challenges. Diabetes Metab Syndr Obes. 2010 Nov 2;3:373–85. doi: 10.2147/DMSOTT.S13860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.World Health Organization Western Pacific Region; International Association for the Study of Obesity; International Obesity Task Force. The Asia-Pacific perspective: redefining obesity and its treatment. Balmain, Australia: Health Communications Australia Pty Limited. 2000:55. Feb. Supported by the Regional Office for the Western Pacific, World health Organization, the International Association for the Study of Obesity, the International Obesity Task Force.
- 23.Sutton K, Logue E, Jarjoura D, et al. Assessing dietary and exercise stages of change to optimize weight loss intervention. Obes Res. 2003 May;11(5):641–52. doi: 10.1038/oby.2003.92. [DOI] [PubMed] [Google Scholar]
- 24.Kim CJ, Kim DJ, Park HR. Effects of a cardiovascular risk reduction intervention with psychobehavioral strategies for Korean adults with type 2 diabetes and metabolic syndrome. J Cardiovasc Nurs. 2011 Mar-Apr;26(2):117–28. doi: 10.1097/JCN.0b013e3181ec02ae. [DOI] [PubMed] [Google Scholar]
- 25.McTigue KM, Harris R, Hemphill B, et al. Screening and interventions for obesity in adults: summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2003 Dec 2;139(11):933–49. doi: 10.7326/0003-4819-139-11-200312020-00013. [DOI] [PubMed] [Google Scholar]
- 26.Johnson SS, Driskell MM, Johnson JL, et al. Transtheoretical model intervention for adherence to lipid-lowering drugs. Dis Manag. 2006 Apr;9(2):102–14. doi: 10.1089/dis.2006.9.102. [DOI] [PubMed] [Google Scholar]
- 27.Prochaska JO, Redding CA, Evers KE. The transtheoretical model and stages of change. In: Glanz K, Rimer BK, Wiswanath K, editors. Health behavior and health education: theory, research, and practice. 4th ed. Jossey-Bass; San Francisco: 2008. pp. 97–121. [Google Scholar]