

Gestational diabetes mellitus (GDM) in both HIV-infected and -uninfected women has been poorly studied in Africa. We enrolled pregnant women ages 15–50 years at a large semiurban clinic in Cameroon. A 75-g oral glucose tolerance test (OGTT) was performed at 24–28 weeks' gestational age or at the earliest prenatal visit for those presenting after 28 weeks. Women were diagnosed with GDM according to American Diabetes Association criteria (1). Data on height, blood pressure, sociodemographics, obstetrical history, prepregnancy weight, HIV clinical status, combination antiretroviral therapy (cART) history, and pregnancy outcomes were collected. Exact logistic regression models were used to identify predictors of GDM.
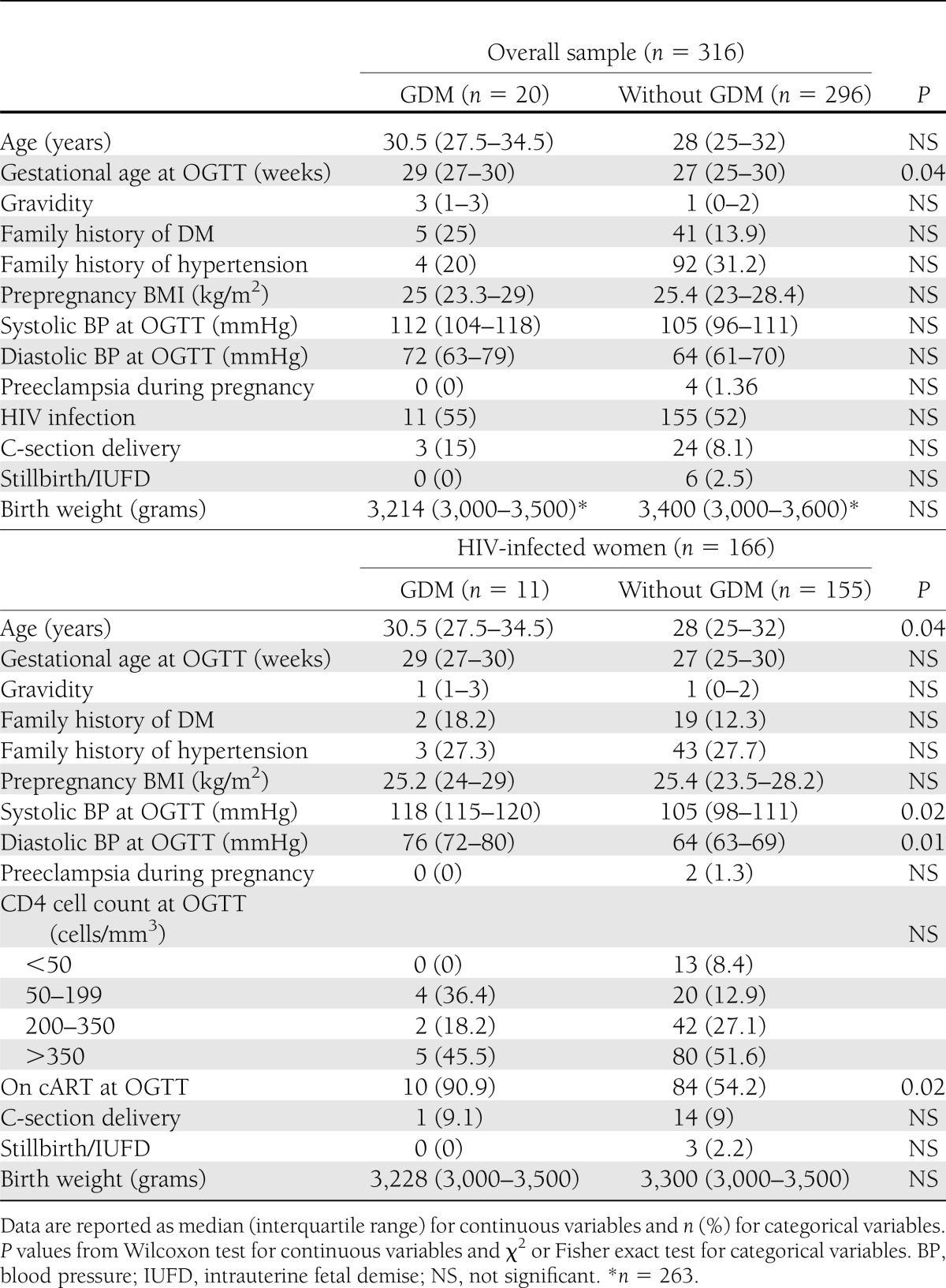
Of 316 participants, 20 (63%) had GDM, and 3 had overt diabetes (DM). Women with GDM presented for OGTT later than those without (29 vs. 27 weeks, P = 0.04) (Table 1). After adjustment for age, gestational age at the time of OGTT, family history of DM, HIV, and prepregnancy BMI, only age ≥30 years remained a significant predictor of GDM. Among HIV-infected women, 6.6% (11 of 166) exhibited GDM. In this subgroup, median age (30.5 vs. 28 years), systolic (118 vs. 105 mmHg) and diastolic (76 vs. 64 mmHg) blood pressure, and rates of cART use during pregnancy (90.9 vs. 54.2%) differed significantly between those with vs. without GDM (P = 0.04, 0.02, 0.01, and 0.02, respectively) (Table 1).
Table 1.
Baseline characteristics and birth outcomes of pregnant women
Our overall rate of GDM (6.3%) is comparable with those reported in developed settings (U.S. 3.2–7.6% and Europe 2–11.6%) (2) as well as scarce African data (Nigeria 4.5–13.4% ([3], Ethiopia 3.7% [4], and South Africa 3.8–8.8% [5]). These rates vary depending on the method and criteria used. Had we used World Health Organization 1999 criteria, 3.2% would have had GDM. In multivariate analysis, older age, but not prepregnancy BMI, remained a significant predictor of GDM. Waist circumference has been shown to be a better predictor of cardiovascular/metabolic disease in nonobese subjects, which may account for this finding. HIV infection was not associated with GDM. The use of cART, particularly, protease inhibitors, has been associated with insulin resistance in pregnant and nonpregnant women. The low rates of cART (33 of 166) and protease inhibitor (1 of 166) use in the HIV-infected subgroup may explain why an association between HIV and GDM was not found in our study. Among HIV-infected women, GDM was associated with higher blood pressure. Almost all (91%) of the HIV-infected women with GDM were on cART. Our cohort had insufficient numbers of HIV-infected women not on cART with GDM to create an adequately powered multivariate model. Nonetheless, the significant association between cART and GDM in univariate analysis is consistent with reports in developed countries.
Our study is limited by its small sample size. The low rates of cART use limited our ability to assess effects of HIV/cART on GDM. Lastly, we could not properly evaluate effects of GDM on birth weight, since subjects delivered at different facilities.
Our study revealed a GDM rate within the range of that in advanced economies, evidence for the growing prevalence of diabetes in Africa, which is projected to double by 2030 as obesity, westernization of diets, and urbanization increase. Moreover, continued high rates of HIV with expanding access to cART may further impact this phenomenon. As GDM is a largely ignored disease in Africa, future studies to determine the scope and identify individuals at risk will inform health policy in resource-limited settings.
Acknowledgments
This study was funded in part by NICHD K23HD070760-01A1 (to J.J.) and the Mount Sinai Global Health Innovation Fund.
J.J. designed the study, analyzed data, and wrote the manuscript. M.W. collected data and helped write the manuscript. R.B.V.D. and M.G. edited the manuscript. E.N. helped analyze data and edited the tables. D.P. and P.T.M. helped design and implement the study and edited the manuscript. E.J.A., R.S.S., and D.L. assisted in study design, audited the data analyses, and edited the manuscript. J.J. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The authors thank all patients and staff at Cameroon Baptist Convention Health Services, Dr. Nancy Palmer, Fanny Epie, Dr. Christopher Sellers, and Dr. Margee Louisias.
References
- 1.American Diabetes Association Standards of medical care in diabetes—2010. Diabetes Care 2010;33(Suppl. 1):S11–S61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schneider S, Bock C, Wetzel M, Maul H, Loerbroks A. The prevalence of gestational diabetes in advanced economies. J Perinat Med 2012;0:1–10 [DOI] [PubMed] [Google Scholar]
- 3.Anzaku AS, Musa J. Prevalence and associated risk factors for gestational diabetes in Jos, North-central, Nigeria. Arch Gynecol Obstet 2013;287:859–863 [DOI] [PubMed] [Google Scholar]
- 4.Seyoum B, Kiros K, Haileselase T, Leole A. Prevalence of gestational diabetes mellitus in rural pregnant mothers in northern Ethiopia. Diabetes Res Clin Pract 1999;46:247–251 [DOI] [PubMed] [Google Scholar]
- 5.Mamabolo RL, Alberts M, Levitt NS, Delemarre-van de Waal HA, Steyn NP. Prevalence of gestational diabetes mellitus and the effect of weight on measures of insulin secretion and insulin resistance in third-trimester pregnant rural women residing in the Central Region of Limpopo Province, South Africa. Diabet Med 2007;24:233–239 [DOI] [PubMed] [Google Scholar]