

Abstract
OBJECTIVE
Type 1 diabetes mellitus causes increased carotid intima-media thickness (IMT) in adults. We evaluated IMT in young subjects with type 1 diabetes.
RESEARCH DESIGN AND METHODS
Participants with type 1 diabetes (N = 402) were matched to controls (N = 206) by age, sex, and race or ethnicity. Anthropometric and laboratory values, blood pressure, and IMT were measured. ANCOVA was used to assess differences controlling for demographic risk factors, cardiovascular risk factors, and HbA1c.
RESULTS
Subjects were 18.9 ± 3.3 years old (50% male, 82.7% non-Hispanic white). Youth with type 1 diabetes had thicker bulb IMT, which remained significantly different after adjustment for demographics and cardiovascular risk factors. Age, sex, adiposity, and systolic blood pressure were consistent significant determinants of IMT. Adjustment for HbA1c eliminated the difference, suggesting the difference was attributable to poor glycemic control.
CONCLUSIONS
Carotid IMT may be increased in youth with type 1 diabetes at high risk for cardiovascular disease. Better control of diabetes may be essential in preventing progression of atherosclerosis.
Type 1 diabetes mellitus leads to increased carotid intima-media thickness (IMT) (1) and higher risk for cardiovascular disease later in life (2). Large studies of carotid ultrasound in youth with type 1 diabetes are lacking. We evaluated adolescents and young adults to determine if increased carotid IMT was present in subjects with type 1 diabetes.
RESEARCH DESIGN AND METHODS
SEARCH CVD is an ancillary study to SEARCH for Diabetes in Youth (3). Nondiabetic controls (N = 402) were frequency matched to cases with type 1 diabetes (N = 206) by age, sex, and race or ethnicity (mean age, 18.9 ± 3.3 years; 50% male; 82.7% non-Hispanic white). The study received Institutional Review Board approval, and appropriate consent or assent was obtained.
Fasting lipids, glucose, and hemoglobin A1c (HbA1c) measurements were obtained (3). The average of two measures of height and weight was used for calculation of BMI z scores. The average of the second and third resting, seated, and auscultatory (aneroid) systolic blood pressure and diastolic blood pressure was used.
B-mode carotid ultrasounds of the common, bulb, and internal carotid arteries were obtained with a linear array transducer (5–12 MHz) at 90, 120, 150, 210, 240, and 270 degrees. Images were read on Amicas-Vericis (Merge, Chicago, IL). The mean IMT from all angles was used. Coefficients of variability for carotid measures of 800 subjects in our laboratory ranged from 1.8 to 5.5%, within published guidelines for reproducibility.
Statistical analyses with SAS software (version 9.2; SAS Institute, Cary, NC) included case-control comparisons of covariates using χ2 tests for categorical variables and t tests for continuous variables. ANCOVA was performed to determine if type 1 diabetes was independently associated with carotid measures after controlling for cardiovascular risk factors.
RESULTS
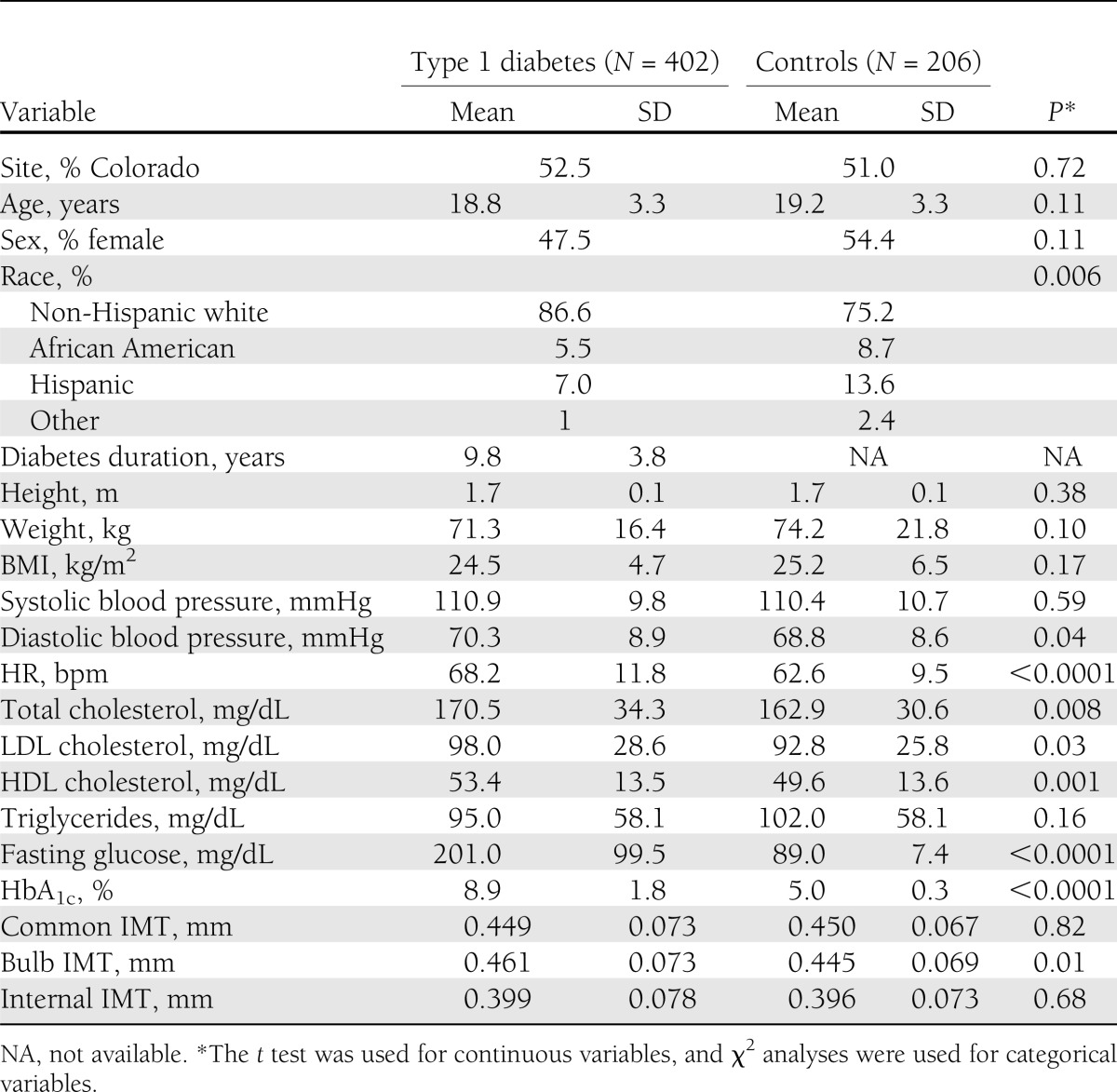
Youth with type 1 diabetes (Table 1) did not differ from controls regarding age, sex, BMI z score, waist circumference, systolic blood pressure, or diastolic blood pressure. There were more non-Hispanic whites with type 1 diabetes. Cases had higher heart rate, total cholesterol, LDL cholesterol, HDL cholesterol, fasting glucose, and HbA1c and had thicker bulb IMT (P < 0.03). These differences persisted after adjustment for demographics and cardiovascular risk factors. Older age, male sex, increased adiposity, and systolic blood pressure z score were the most consistent significant determinants of carotid thickness. LDL cholesterol was a determinant of internal carotid IMT and triglycerides of common and bulb IMT (R2 for common, 0.12; bulb, 0.15; internal, 0.16; all models P ≤ 0.001). The addition of HbA1c eliminated the case-control difference for carotid bulb (0.464 in cases compared with 0.447 in controls; P = 0.15), suggesting that glycemic control may be an important factor explaining the difference in carotid thickness.
Table 1.
Case-control contrasts
CONCLUSIONS
We present the largest comparison of carotid IMT in adolescents and young adults with type 1 diabetes and healthy controls, demonstrating thicker carotid bulb IMT in cases after adjustment for cardiovascular risk factors. Because the rate of progression of IMT in healthy subjects (mean age, 40 years) in the Bogalusa Heart study was 0.017–0.020 mm/year (4), our difference of 0.016 mm suggests that our type 1 diabetic subjects had a vascular age 1 year advanced from their chronological age. We found that IMT was related to type 1 diabetes, age, sex, adiposity, and systolic blood pressure, with triglycerides playing a role in common and bulb IMT, and LDL played a role in internal carotid IMT. Further adjustment for HbA1c ablated the case-control difference in IMT, suggesting that the thicker carotid IMT in the subjects with diabetes could be attributed to diabetes-related hyperglycemia.
In the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study, progression of IMT over the course of 6 years was faster in subjects with type 1 diabetes, yielding a thicker final IMT in cases (5). There was no difference in IMT at baseline. However, DCCT/EDIC did not image the bulb, which is likely the earliest site of thickening according to the Bogalusa Heart Study, which found the carotid bulb to be significantly thicker than the other two segments (6).
Previous studies of youth reported case-control differences in the common carotid IMT, which is in contrast to our finding of no difference. However, they were conducted in a different country with a different ethnicity (7), enrolled patients with poorer glycemic control (higher HbA1c) (8), or had a control group with a more favorable cardiovascular risk factor profile than our controls (9). Other studies that found no case-control difference in IMT in youth either examined a much smaller number of younger subjects (10) or failed to image the carotid bulb (11). Our analyses reinforce the importance of imaging the carotid bulb, often the site of earliest detectible subclinical atherosclerosis in youth.
The DCCT/EDIC study demonstrated that the intensive treatment group had a slower progression of IMT (5) and that mean HbA1c levels explained most of the differences in IMT progression between treatment groups (12). One longitudinal study of youth found children with type 1 diabetes who had progression of IMT over the course of 2 years had higher HbA1c (13). Our data emphasize the role of diabetes-related hyperglycemia in increasing IMT in youth with type 1 diabetes.
As seen in other studies of IMT in youth with diabetes (14), very little of the variance in IMT is explained by our models. Another limitation is our cross-sectional design, which precludes us from determining the causative factors for increased IMT. Our use of a slightly more overweight control group, although representative of our clinic population, may have obscured some case-control difference. However, we were adequately powered to see a difference with our sample size and variability such that we were powered to detect a mean difference of 0.017 compared with published studies of youth with type 1 diabetes that showed a difference of 0.034 mm (15) to 0.15 mm (16).
In summary, our study provides novel evidence that carotid thickness is increased in youth with type 1 diabetes compared with healthy controls and that this difference is not accounted for by traditional cardiovascular risk factors. Better control of diabetes-related hyperglycemia may be needed to reduce future cardiovascular disease.
Acknowledgments
The SEARCH CVD study was funded by R01DK078542 (to D.D.).
No potential conflicts of interest relevant to this article were reported.
E.M.U., D.D., R.B.D., L.M.D., R.F.H., S.R.D., S.M., and R.P.W. were involved in the design and collection of the data. E.M.U., D.D., R.B.D., A.S.S., L.M.D., R.F.H., S.R.D., S.M., and R.P.W. were involved in data analyses and manuscript preparation and contributed to editing. E.M.U. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Parts of this study were presented at the 71st Scientific Sessions of the American Diabetes Association, San Diego, California, 24–28 June 2011.
The SEARCH CVD study is indebted to the many youth and their families, and their health care providers, whose participation made this study possible. The authors also thank all of the SEARCH for Diabetes in Youth investigators and study staff, whose help was essential in moving this project forward.
References
- 1.Wagenknecht LE, Zaccaro D, Espeland MA, Karter AJ, O’Leary DH, Haffner SM. Diabetes and progression of carotid atherosclerosis: the insulin resistance atherosclerosis study. Arterioscler Thromb Vasc Biol 2003;23:1035–1041 [DOI] [PubMed] [Google Scholar]
- 2.Krolewski AS, Kosinski EJ, Warram JH, et al. Magnitude and determinants of coronary artery disease in juvenile-onset, insulin-dependent diabetes mellitus. Am J Cardiol 1987;59:750–755 [DOI] [PubMed] [Google Scholar]
- 3.Dabelea D, Pihoker C, Talton JW, et al. SEARCH for Diabetes in Youth Study Etiological approach to characterization of diabetes type: the SEARCH for Diabetes in Youth Study. Diabetes Care 2011;34:1628–1633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stein JH, Douglas PS, Srinivasan SR, et al. Distribution and cross-sectional age-related increases of carotid artery intima-media thickness in young adults: the Bogalusa Heart Study. Stroke 2004;35:2782–2787 [DOI] [PubMed] [Google Scholar]
- 5.Nathan DM, Lachin J, Cleary P, et al. Diabetes Control and Complications Trial. Epidemiology of Diabetes Interventions and Complications Research Group Intensive diabetes therapy and carotid intima-media thickness in type 1 diabetes mellitus. N Engl J Med 2003;348:2294–2303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Urbina EM, Srinivasan SR, Tang R, Bond MG, Kieltyka L, Berenson GS, Bogalusa Heart Study Impact of multiple coronary risk factors on the intima-media thickness of different segments of carotid artery in healthy young adults (The Bogalusa Heart Study). Am J Cardiol 2002;90:953–958 [DOI] [PubMed] [Google Scholar]
- 7.Margeirsdottir HD, Stensaeth KH, Larsen JR, Brunborg C, Dahl-Jørgensen K. Early signs of atherosclerosis in diabetic children on intensive insulin treatment: a population-based study. Diabetes Care 2010;33:2043–2048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stakos DA, Schuster DP, Sparks EA, Wooley CF, Osei K, Boudoulas H. Cardiovascular effects of type 1 diabetes mellitus in children. Angiology 2005;56:311–317 [DOI] [PubMed] [Google Scholar]
- 9.Schwab KO, Doerfer J, Krebs A, et al. Early atherosclerosis in childhood type 1 diabetes: role of raised systolic blood pressure in the absence of dyslipidaemia. Eur J Pediatr 2007;166:541–548 [DOI] [PubMed] [Google Scholar]
- 10.Gunczler P, Lanes R, Lopez E, Esaa S, Villarroel O, Revel-Chion R. Cardiac mass and function, carotid artery intima-media thickness and lipoprotein (a) levels in children and adolescents with type 1 diabetes mellitus of short duration. J Pediatr Endocrinol Metab 2002;15:181–186 [DOI] [PubMed] [Google Scholar]
- 11.Parikh A, Sochett EB, McCrindle BW, Dipchand A, Daneman A, Daneman D. Carotid artery distensibility and cardiac function in adolescents with type 1 diabetes. J Pediatr 2000;137:465–469 [DOI] [PubMed] [Google Scholar]
- 12.Polak JF, Backlund JY, Cleary PA, et al. DCCT/EDIC Research Group Progression of carotid artery intima-media thickness during 12 years in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study. Diabetes 2011;60:607–613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dalla Pozza R, Netz H, Schwarz H-P, Bechtold S. Subclinical atherosclerosis in diabetic children: results of a longitudinal study. Pediatr Diabetes 2010;11:129–133 [DOI] [PubMed] [Google Scholar]
- 14.Urbina EM, Kimball TR, McCoy CE, Khoury PR, Daniels SR, Dolan LM. Youth with obesity and obesity-related type 2 diabetes mellitus demonstrate abnormalities in carotid structure and function. Circulation 2009;119:2913–2919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Heilman K, Zilmer M, Zilmer K, et al. Arterial stiffness, carotid artery intima-media thickness and plasma myeloperoxidase level in children with type 1 diabetes. Diabetes Res Clin Pract 2009;84:168–173 [DOI] [PubMed] [Google Scholar]
- 16.Atabek ME, Kurtoglu S, Pirgon O, Baykara M. Arterial wall thickening and stiffening in children and adolescents with type 1 diabetes. Diabetes Res Clin Pract 2006;74:33–40 [DOI] [PubMed] [Google Scholar]