

Abstract
Attentional interference by threat is associated with PTSD, but the mechanisms of this relationship remain unclear. Attentional interference might be related to increased use of maladaptive thought control strategies, such as suppressing unwanted thoughts (thought suppression) or replacing threatening thoughts with everyday concerns (worry), which increase PTSD risk. Conversely, attentional interference might be associated with reduced use of adaptive strategies, such as talking about threatening thoughts (social control) which decrease PTSD risk. This study tested if thought control strategies mediate the relationship between attentional interference and PTSD. Sixty-one male Vietnam-era veterans completed measures of PTSD symptoms and thought control strategies. Participants also completed a visual search task measuring attentional interference, which required participants to identify a target letter string among a group of threat or neutral words. Attentional interference by threat was related to PTSD symptoms, and mediation analyses revealed significant indirect effects of attentional interference through thought suppression and worry. Attentional interference was related to reexperiencing and avoidance, but not hyperarousal, symptom clusters. Thought suppression was a unique mediator for reexperiencing, whereas thought suppression and worry both mediated the relationship with avoidance. These results offer evidence for maladaptive thought control strategies as a mechanism linking attentional biases for threat to PTSD.
Keywords: attention, PTSD, information processing bias, thought control, thought suppression
Information processing models describe attentional biases for threat as important factors in the development and maintenance of anxiety disorders (e.g., MacLeod & Mathews, 1988). Attentional biases can take several forms including vigilance, avoidance, or difficulty withdrawing attention from threat. Difficulty withdrawing attention from trauma-related stimuli has emerged as a form of attentional bias associated with Posttraumatic Stress Disorder (PTSD; Kimble, Fleming, Bandy, Kim, & Zambetti, 2010; Pineles et al., 2007; Pineles, Shipherd, Mostoufi, Abramowitz, & Yovel, 2009). In particular, individuals with PTSD have demonstrated difficulty withdrawing attention from trauma stimuli that results in interference to another primary task, a process termed attentional interference (Pineles et al., 2007; 2009).
Attentional interference might be expected to underlie PTSD symptoms such as intrusive thoughts, which are characterized by difficulty removing attention from distressing trauma memories. However, the mechanisms of the relationship between attentional interference and PTSD remain unclear. Metacognitive models of PTSD have argued that one’s responses to threat-relevant thoughts are important in determining whether such thoughts lead to long-lasting emotional problems (Wells & Davies, 1994). Specifically, individuals engage in attempts to control unwanted threatening thoughts. The type of strategy one uses can either increase or decrease risk that PTSD symptoms will be maintained. Avoidance-based strategies such as suppressing one’s thoughts or avoiding them are thought to be maladaptive, whereas approach-based strategies such as reappraising thoughts or reaching out for social support are thought to be more adaptive. Therefore, simply attending to threat-relevant information is not thought to be problematic by itself; rather, responding to threatening thoughts with avoidance-based strategies is thought to maintain PTSD (Wells, 2000). Bennett and colleagues (2009) found that thought control strategies partially mediated the relationship between PTSD symptoms and negative trauma-related cognitions, offering initial support for such a metacognitive model. Prior work has also shown that thought suppression mediates the relationship between negative beliefs about intrusions and intrusive thoughts in individuals exposed to an analogue stressor (Nixon, Cain, Nehmy, & Seymour, 2009). It is likely that similar associations occur for basic attentional processes. Specifically, maladaptive attempts to control unwanted threat-relevant thoughts may account for the relationship between difficulty withdrawing attention from threat and PTSD symptom severity. Thought suppression, worry, and social control are three thought control strategies shown to be positively or negatively related to PTSD symptoms in prior work, and may be particularly relevant to the relationship between attentional interference and PTSD symptom severity.
Having trouble withdrawing attention from threat might be expected to lead to attempts to suppress threatening thoughts when they occur. Cognitive bias modification, which trains attention away from threat, has been proposed as a means of escaping unwanted thoughts without resorting to ineffective thought suppression, suggesting that successful attention training would reduce the need for thought suppression (Wegner, 2011). However, the association between attentional interference by threat and use of thought suppression has yet to be examined. In contrast, the association between thought suppression and PTSD has been extensively studied. Individuals with PTSD report engaging in more thought suppression than individuals without PTSD, and thought suppression prospectively predicts the maintenance of PTSD symptoms over time (Amir et al., 1997; Ehlers, Mayou, & Bryant, 1998). Suppression of trauma-related thoughts is associated with greater rebound effects, or greater occurrence of the suppressed thought after the suppression induction, in individuals with PTSD compared to trauma-exposed control participants (Amstadter & Vernon, 2006; Shipherd & Beck, 1999; 2005). This effect is specific to trauma-related stimuli, with no greater rebound effects found for neutral stimuli (Shipherd & Beck, 2005). Although much of the experimental research on thought suppression in PTSD focuses on intrusive thoughts, thought suppression is conceptualized as a form of cognitive avoidance, and has been found to be related not only to intrusions but also to avoidance symptoms (Amir et al., 1997).
Worry, or the strategy of replacing unwanted thoughts with worry about less important concerns, is another avoidant thought control strategy (Wells & Davies, 1994). Attentional interference by threat might contribute to the use of worry as a control strategy, as a means of distracting oneself from threat cues that are difficult to disengage. Emerging evidence indicates that reducing attentional biases, by training attention away from threat, decreases self-reported worry in individuals with high levels of worry and in individuals diagnosed with generalized anxiety disorder (Hazen, Vasey, & Schmidt, 2009; Amir, Beard, Burns, & Bomyea, 2009). Similarly, training attention away from threat reduced persistence of worry following a lab-based worry induction in a nonclinical sample (Krebs, Hirsch, & Mathews, 2010). Taken together, these findings suggest a relationship between attentional biases for threat and use of worry. Prior research has also shown that worry is related to PTSD symptoms both concurrently (Bennett, Beck, & Clapp, 2009; Scarpa, Wilson, Wells, Patriquin, & Tanaka, 2009) and prospectively (Holeva, Tarrier, & Wells, 2001), offering support for worry as a PTSD maintenance factor.
Social control, or the solicitation of validation and/or support from others in response to negative unwanted thoughts, requires withdrawing attention from a stimulus, reflecting upon one’s reaction to that stimulus, and choosing to discuss that reaction with another individual. If difficulty withdrawing attention from threatening stimuli reduces one’s ability to engage in this adaptive, but potentially resource-demanding, strategy for managing threatening thoughts, attentional interference might decrease use of social control. Because social control also requires active engagement with the unwanted thought through continued focus on the thought during the solicitation of social support, individuals who have difficulty withdrawing attention from threat may be reluctant to use such an approach-based strategy. Social control is conceptualized as a protective factor and is negatively related to PTSD symptoms both concurrently and prospectively (Bennett et al., 2009; Holeva et al., 2001; Reynolds & Wells, 1999). Therefore, attentional interference by threat is expected to decrease use of social control, and decreased use of social control is expected to increase risk for PTSD.
The aim of the current study was to examine these three thought control strategies as potential mediators of the relationship between attentional interference by threat and PTSD. Consistent with metacognitive theory, we predicted that attentional interference would not lead to PTSD directly, but that attentional interference would have an indirect effect on PTSD through its effect on thought control strategies. Specifically, we predicted that attentional interference by threat would be associated with increased use of avoidance-based thought control strategies (thought suppression and worry) and decreased use of approach-based strategies (social control), and that these thought control strategies would mediate the relationship between attentional interference and PTSD.
A secondary aim of the current study was to examine whether attentional interference is differentially related to the DSM-IV-TR PTSD symptom clusters of reexperiencing (cluster B), avoidance (cluster C), and hyperarousal (cluster D). Because attentional interference is thought to underlie PTSD symptoms such as intrusive memories, it was predicted that attentional interference would be related to reexperiencing symptoms. Given the evidence that thought suppression is associated with increased intrusions, and we predicted that the relationship between attentional interference and reexperiencing would be mediated by thought suppression. Additionally, it was expected that attentional interference would be related to avoidance symptoms and that this association would be mediated by all three thought control strategies. Thought suppression and worry are both forms of cognitive avoidance, which might be expected to facilitate other forms of avoidance, such as refusing to talk about a traumatic event, avoiding reminders of the event, and emotional numbing. Social control is a strategy of disclosing one’s thoughts to others, which is incompatible with avoidance. Therefore, social control is expected to be negatively related to avoidance symptoms. Because hypervigilance is theorized to be related to facilitation of attention towards threat rather than delayed withdrawal from threat, no association between attentional interference and hyperarousal symptoms was expected.
Method
Participants
These data were collected as part of a larger study comparing attention facilitation and interference in veterans with PTSD (Pineles et al., 2007). Sixty-one male Vietnam-era veterans were recruited from a Department of Veterans Affairs (VA) medical center. Participants’ ages ranged from 47 to 64, with a mean age of 54.75 (SD = 4.5). The racial/ethnic make-up of the sample was 45 (74%) Caucasian, 10 (16%) African American, 3 (5%) Latino/Hispanic, 1 (1.6%) American Indian, 1 (1.6%) Biracial, and 1 (1.6%) “Other.”
Materials
White Bear Suppression Inventory (WBSI; Wegner & Zanakos, 1994)
The WBSI is a commonly used and well-validated measure of thought suppression. Responses on a five-point Likert scale (1 = “strongly disagree,” 3 = “neutral,” 5 = “strongly agree”) yield total scores ranging from 15 to 75. Higher scores indicate more suppression. The WBSI has demonstrated good reliability and temporal stability (Wegner & Zanakos, 1994). Scores on the WBSI are positively correlated with number of recent intrusive thoughts (Muris, Merckelbach, & Horselenberg, 1996). The internal consistency of the scale in this study was α = .97.
Thought Control Questionnaire (TCQ; Wells & Davies, 1994)
The TCQ is a 30 item self-report measure which assesses five thought control strategies. The TCQ asks participants to rate the extent to which they engage in different control strategies on a 4 point Likert-type scale. The TCQ has been validated in both unselected samples (Wells & Davies, 1994) and in psychiatric patients with diagnoses of PTSD and Major Depression (Reynolds & Wells, 1999). For the purposes of this study, we examined two strategies that have been consistently associated with PTSD symptoms: worry and social control. The worry subscale includes six items which assess the tendency to replace unpleasant or unwanted thoughts with worries about less pressing concerns (e.g., “I worry about more minor things instead”). The social control scale includes six items, three of which are reverse-scored, and assesses the extent to which participants disclose unpleasant or unwanted thoughts to others (e.g., “I talk to a friend about the thought”). In this study, the internal consistency was α = .79 for the worry scale and α = .76 for the social control scale.
PTSD Checklist (PCL)
The PCL is a 17-item self-report measure of PTSD symptom severity. Each item of the PCL corresponds to a symptom of PTSD as specified by the Diagnostic and Statistical Manual (DSM-IV-TR; American Psychiatric Association, 2000). Participants are asked to rate the degree to which they are bothered by each symptom on a scale from 1 to 5 (“not at all” to “extremely”). The PCL has good reliability and has been well-validated in samples of military veterans (Forbes, Creamer, & Biddle, 2001). We used the total score of the PCL as our measure of overall PTSD symptom severity. We also calculated cluster scores for each of the DSM-IV-TR PTSD symptom clusters. For each cluster, the sum of the items corresponding to those symptoms was calculated, with 5 items for reexperiencing, 7 items for avoidance, and 5 items for hyperarousal. In this study, the internal consistency was α = .96 for the total scale, and .93, .92, and .88 for the reexperiencing, avoidance, and hyperarousal scales, respectively.
Visual Search Task (VST)
Stimuli on interference trials were threat-relevant words, categorized neutral words related to a school theme, and unpronounceable letter strings (nonwords). Threat-relevant and neutral words had been validated in previous study with Vietnam veterans and were matched for length and frequency of usage (Litz et al., 1996). Interference trials included a nonword target embedded in an array of 3, 5, or 7 identical distracters (either threat-relevant or neutral; see Figure 1). Each trial began with a fixation cross which was presented for 700 ms. Immediately following the fixation cross, the array of letter strings appeared on the screen, where it remained until the participant made a response. The computer screen then remained blank for 1000 ms between trials. Participants were asked to report whether or not the “oddball” letter string was a word or a nonword by pressing one of two keys on the keyboard. For the purposes of this study, a threat bias score was calculated by subtracting response time (RT) on trials with neutral words in the background from trials with threat words in the background. This bias score was used as our measure of attentional interference by threat, and larger numbers reflect greater interference.
Figure 1.
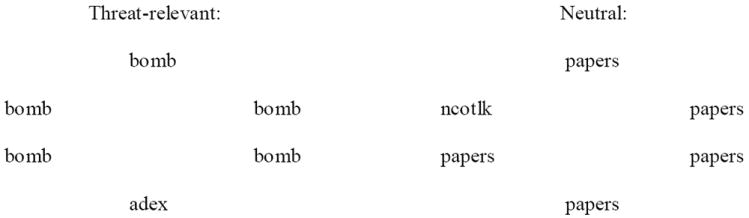
Sample arrays for interference trials on the Visual Search Task.
Note. Not to scale. These are examples of trials with five distractors; other trials included three or seven distracters.
All stimuli were presented on a 21” monitor (800 × 600, 60 Hz) using Superlab software. Stimuli were presented in black Times New Roman font on a white background, and were equally spaced around a 175mm × 80mm ellipsoid area, subtending a visual angle of approximately 11.2° × 5.0°. The full version of the VST also included facilitation trials, assessing facilitation of attention towards threatening targets in nonword backgrounds. The full VST also included catch trials which consisted of target nonwords surrounded by nonword distractors, and target neutral words surrounded by neutral word distractors. These catch trials were included for participant engagement. Neither facilitation nor catch trails were included in any analyses reported below. For more information about the full VST, please see Pineles et al. (2007).
Procedure
Participants met individually with the experimenter and completed the VST and all self-report questionnaires. The facilitation and interference trials of the VST were presented in blocks, and participants were randomly assigned to complete either interference or facilitation trials first. Thirty three participants (54%) completed the interference trials first. Prior to starting the VST, all participants first read instructions and completed 20 practice trials with auditory feedback about accuracy.
Data Analytic Plan
We will describe the demographics of the sample and examine whether any demographic variables are correlated with any of the thought control strategies assessed. Our primary analysis will be a multiple mediation model with attentional interference entered as the independent variable, thought suppression, worry, and social control entered as mediators, and PTSD symptom severity entered as the dependent variable. Because facilitation of attention was not associated with overall PTSD symptoms in the larger study (Pineles et al., 2007), no mediation analyses were planned for facilitation trials.1 Per currently accepted standards for mediation analyses, we planned to use bootstrapping with 5000 samples to calculate all indirect effects, using the SPSS macro developed by Preacher and Hayes (2008). Additional multiple mediational models were planned to examine these thought control strategies as mediators of the relationship between attentional interference and each of the specific PTSD symptom clusters (reexperiencing, avoidance, and hyperarousal symptoms). Finally, to explore the direction of these effects, we planned reverse meditational models with attentional interference entered as a mediator of the relationships between thought control and PTSD symptom severity. For all analyses, we will collapse across condition (interference first, facilitation first) and array size (3, 5, or 7 distracters). Because condition order affected the attentional interference results in the parent study (Pineles et al., 2007), we will include condition as a covariate in all of the analyses reported. All confidence intervals (CIs) reported will be bias-corrected. Unstandardized betas will be reported, and partial correlation coefficients (pr) will be provided as indices of effect size.
Results
No demographic variables (age, race) were related to use of any of the three thought control strategies assessed (rs < .25, ns; Fs < 1.5, ns). Thought suppression was positively correlated with worry (r = .57, p < .001) and negatively correlated with social control (r = -.52, p < .001). The correlation between worry and social control was not statistically significant (r = -.23, p = .08). Average response times on the VST are presented in Table 1.
Table 1.
Mean Response Times in Milliseconds on the Visual Search Task
| Low PTSD (n = 29) | High PTSD (n = 32) | Total (n = 61) | |
|---|---|---|---|
| Trauma Backgrounds | 1648 (500) | 1800 (567) | 1728 (537) |
| Neutral Backgrounds | 1736 (604) | 1756 (479) | 1747 (537) |
| Attentional Interference (Trauma-Neutral) | -88 (119) | 44 (167) | -19 (160) |
Note. Mean response times are presented in milliseconds with standard deviations in parentheses. PTSD symptom severity was dichotomized for ease of presentation, with participants with PCL scores of 50 or higher included in the High PTSD group.
Overall PTSD symptom severity
Participants reported a wide range of PTSD symptom severity, with PCL scores covering the entire possible range of scores on this measure (17 to 85). The mean PCL score in this sample was 49 (median = 50; SD = 17.65). A score of 50 or higher is indicative of clinically significant PTSD symptoms for this population (Forbes et al., 2001). Attentional interference was significantly associated with overall PTSD symptoms (t = 2.08, p = .04, pr = .27). The associations between attentional interference and thought suppression (t = 2.42, p = .02, pr = .31), worry (t = 2.19, p =.03, pr = .28), and social control (t = 2.23, p = .03, pr =.29) were all significant (see Figure 2a for coefficients). After controlling for attentional interference, thought suppression (t = 6.86, p < .001, pr =.68) and worry (t = 2.25, p =.03, pr = .29) were significantly related to PTSD symptoms. The association between social control and PTSD symptoms, however, was not significant (t = 0.10, p = .92, pr < .01). The overall indirect effect was significant, (95% CI = [.0143, .0585]; confidence intervals not containing zero are statistically significant), and the relationship between attentional interference and PTSD symptoms was reduced to nonsignificance after entering the mediators into the model (t = -0.09, p = .93, pr = .01; see also Figure 2a). Indirect effects were significant for attentional interference through thought suppression (95% CI = [.0114, .0493]) and worry (95% CI = [.0001, .0232]); however, the indirect effect of attentional interference through social control was not significant (95% CI: [-.0103, .0078]). These findings indicate that the three thought control strategies fully mediated the relationship between attentional interference and PTSD symptoms, and that thought suppression and worry, but not social control, were significant mediators.
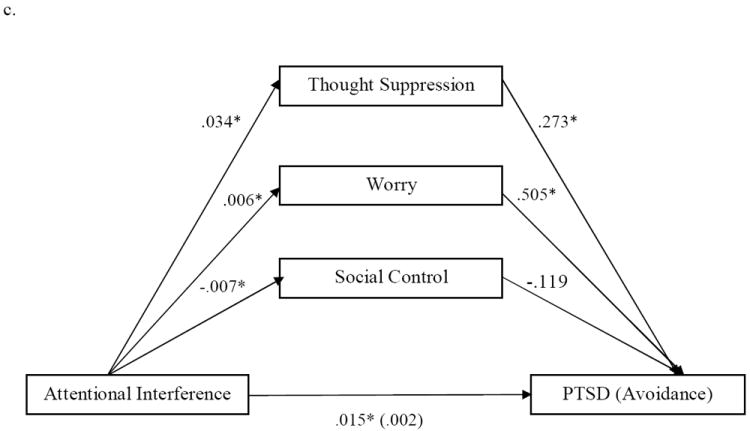
Figure 2.
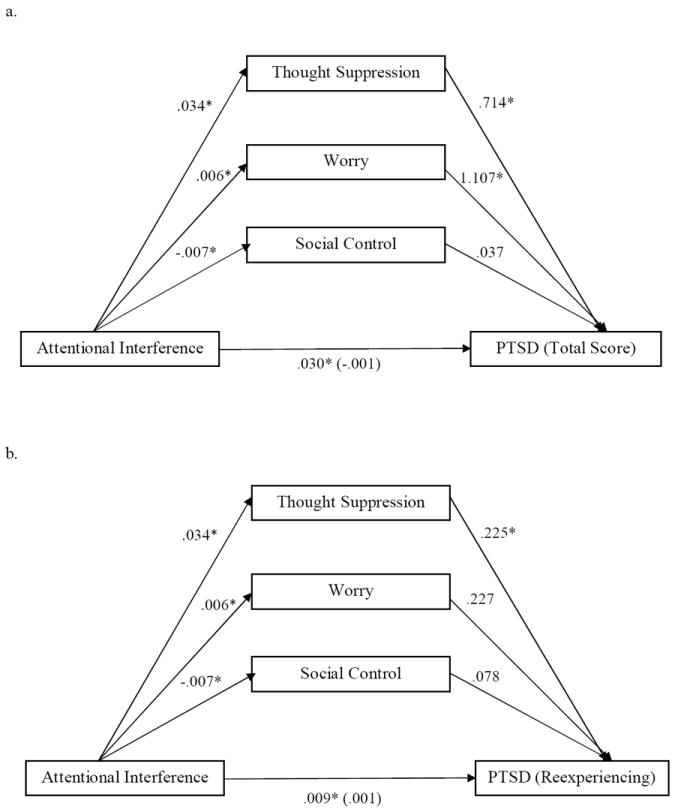
a. Mediational Model for Overall PTSD symptom severity
b. Mediational Model for Reexperiencing Symptoms
c. Mediational Model for Avoidance Symptoms
Note. *p < .05. The paths from attentional interference to PTSD show the total effects and the direct effects after controlling for the mediators, with the direct effects in parentheses. All betas are unstandardized.
One possible explanation for this pattern of findings is that social control has an independent association with PTSD symptoms, but is no longer significant after statistically controlling for other thought control strategies. To explore this possibility, we ran a post-hoc meditational model with social control entered as the sole mediator. In the simple meditational model, social control was significantly related to PTSD symptoms after controlling for attentional interference (β = -1.6664, t = -3.03, p = .004, pr =-.37), such that greater use of social control was related to lower PTSD symptom levels. There was also a significant indirect effect of attentional interference on PTSD symptoms through social control in the predicted direction (95% CI = [.0017, .0327]), and the association between attentional interference and PTSD symptoms was reduced to nonsignificance after accounting for social control (β = .0179, t = 1.29, ns, pr =.17). Taken together, these findings indicate that attentional interference is related to use of social control and that social control mediates the relationship between attentional interference and PTSD symptoms. However, the effect of social control on PTSD symptoms may be better accounted for by other thought control strategies (thought suppression and worry).
PTSD Symptom Cluster Analyses
We next examined each of the PTSD symptom clusters separately. Mean scores on the PCL subscales, divided by the number of items, were as follows: reexperiencing = 2.62 (SD = 1.1), avoidance = 2.97 (SD = 1.1), and hyperarousal = 3.08 (SD = 1.1). Using standard scoring criteria, individual symptoms with scores of 3 or higher are considered present (Forbes et al., 2001). Attentional interference was a significant predictor of both reexperiencing (β = .0091, t = 2.00, p = .05, pr = .26), and avoidance symptoms (β = .0149, t = 2.37, p = .02, pr = .30). The relationship between attentional interference and hyperarousal was not significant (β =.0056, t = 1.24, ns, pr = .16); therefore, no mediation analyses are reported for this cluster.
We then ran two multiple meditational models to follow up on the significant relationships, one with reexperiencing as the outcome variable and one with avoidance as the outcome (see Figures 2b and 2c). In both models attentional interference was entered as the predictor and the same three thought control strategies were entered as mediators. The pathways between attentional interference and the three thought control strategies are identical to those presented in the overall model. After controlling for attentional interference, thought suppression was a significant predictor of reexperiencing symptoms (t = 5.74, p < .001, pr = .61), but neither worry nor social control were significant predictors, (ts < 2, ns, prs < .17). The overall indirect effect was significant in this model (95% CI = [.0037, .0169]), and after controlling for the mediators, the association between attentional interference and reexperiencing dropped to nonsignificance (t = .17, ns, pr =.02). A significant indirect effect of attentional interference on reexperiencing symptoms emerged only for thought suppression, (95% CI = [.0033, .0162]), with no indirect effects for the paths through worry, (95% CI = [-.0006, .0067]), or social control, (95% CI = [-.0048, .0019]). These findings indicate that thought suppression uniquely and fully accounted for the relationship between attentional interference and reexperiencing symptoms.
In terms of avoidance symptoms, after controlling for attentional interference, both thought suppression (t = 5.40, p < .001, pr = .59), and worry (t = 2.30, p = .03, pr = .29), were significant predictors. The relationship between social control and avoidance, however, was not significant (t = -0.62, ns, pr = .08). The overall indirect effect was significant for avoidance (95% CI = [.0061, .0256]), and the association between attentional interference and avoidance dropped to nonsignificance after entering the mediators into the model (t = .37, ns, pr = .05). Significant indirect effects of attentional interference on avoidance emerged for the paths through thought suppression, (95% CI = [.0044, .0191]), and worry, (95% CI = [.0002, .0105]), but not social control, (95% CI = [-.0022, .0063]). These results indicate that thought suppression and worry together fully account for the relationship between attentional interference and avoidance symptoms.
Reverse Mediational Models
To explore the direction of these effects, we ran additional mediational models examining attentional interference as a mediator of the relationship between thought control and PTSD symptom severity. Three separate models were run for each of the thought control strategies assessed. Thought suppression (t =2.42, p = .02, pr =.31), worry (t = 2.19, p =.03, pr =.28), and social control (t = -2.23, p = .02, pr = -.28) were significantly related to attentional interference. However, the association between attentional interference and PTSD was no longer significant after controlling for thought suppression (t = .19, ns, pr = .03), worry (t = .94, ns, pr = .12), or social control (t = 1.28, ns, pr =.17). The indirect effect of thought control on PTSD symptom severity through attentional interference was not significant for any of these models.
We ran similar reverse meditational models for each of the three PTSD symptom clusters. In each of these models, the relationship between attentional interference and reexperiencing, avoidance, or hyperarousal symptoms dropped to nonsignificance after controlling for thought suppression, worry, or social control, ts < 1.6, ns, prs < .20. None of the indirect effects in these models were significant.
Discussion
Thought control strategies fully mediated the relationship between attentional interference and PTSD symptoms. Consistent with our predictions, difficulty withdrawing attention from threat was related to increased use of thought suppression and worry, which accounted for the relationship between attentional interference and PTSD symptoms. These findings are consistent with metacognitive theories of PTSD, which argue that simply attending to threat is not problematic; rather, responding to threat-relevant thoughts with suppression or avoidance leads to longer-lasting problems. The indirect effect of attentional interference on PTSD through social control was significant in a simple meditational model, but not when including thought suppression and worry as additional mediators. These findings indicate that thought suppression and worry better account for the relationship between attentional interference and PTSD than social control. Therefore, to break the link between attentional biases for threat and PTSD, decreasing use of thought suppression and worry may be more helpful than encouraging active coping such as soliciting social support in response to one’s threatening thoughts.
The predictions for differential relationships between attentional interference and the three DSM-IV-TR PTSD symptom clusters were partially supported. Consistent with predictions, attentional interference was significantly related to reexperiencing and avoidance but not hyperarousal symptoms. The mediational analyses support thought control strategies as mechanisms of the relationship between attentional interference and both reexperiencing and avoidance symptoms. Consistent with predictions, thought suppression completely mediated the relationship between attentional interference and reexperiencing symptoms, and was the only significant mediator of this relationship. This is consistent with previous work indicating that thought suppression increases intrusions of trauma-related thoughts in individuals with PTSD (Amstadter & Vernon, 2006; Shipherd & Beck, 1999; 2005). Our findings can also inform a persistent question in the thought suppression literature: If thought suppression increases intrusions, why do people use this ineffective strategy? Our findings indicate that individuals may use thought suppression because they have difficulty disengaging attention from threat. If one attends to a threatening stimulus, but is able to withdraw attention quickly and attend to other stimuli in the environment, there is no need to engage in maladaptive thought suppression. However, if one has difficulty withdrawing attention from threat, particularly from threatening information irrelevant to the task at hand, one may attempt to suppress threat-related thoughts when they occur. Our findings suggest that cognitive bias modification (CBM) techniques, which are used to train attention away from threat, may have the added benefit of reducing the need for thought suppression (Wenzlaff, 2011). Furthermore, if CBM successfully reduces thought suppression, it may then reduce reexperiencing symptoms of PTSD.
In our study, both thought suppression and worry mediated the relationship between attentional interference and avoidance symptoms. Suppression is generally conceptualized as a type of cognitive avoidance, and would therefore be expected to predict engagement in other forms of avoidance. However, existing research on the role of thought suppression in PTSD has focused primarily on reexperiencing symptoms, specifically on intrusive thoughts. Our findings indicate that thought suppression is related to avoidance as well as reexperiencing symptoms, and that future research on thought suppression could expand its focus from intrusive thoughts to other PTSD symptoms, including behavioral avoidance and emotional numbing. Likewise, worry is conceptualized as a form of cognitive avoidance (Borkovec, Alcaine, & Behar, 2004). This study offers support for the avoidance model of worry and indicates that worry is uniquely associated with the avoidance symptoms of PTSD.
Contrary to our predictions, but consistent with the findings for overall PTSD symptoms, social control was not a significant mediator of the relationship between attentional interference and avoidance symptoms. Interestingly, the path from attentional interference to social control was significant, indicating that difficulty withdrawing attention from threat was associated with less use of social control. As mentioned previously, difficulty withdrawing attention from threat may leave fewer cognitive resources available to engage in a resource-demanding strategy such as social control. An alternative explanation is that engaging in social control leads to faster withdrawal of attention from threat. Marroquin (2011) has argued that social support can correct negative attentional biases associated with depression by encouraging reorientation towards neutral or positive stimuli and by providing a wider range of neutral and positive stimuli in the attentional field. Similar processes could correct threat-relevant biases associated with PTSD. Talking to others about one’s unwanted threat-relevant thoughts might offer the opportunity to receive corrective information and discourage dwelling upon threat-relevant content. A greater understanding of the possible reciprocal relationships between negative attentional biases and social control is an important topic for future research.
A primary limitation of the current study is the use of cross-sectional data to test our theoretical model, which precludes any claims about causality. We cannot rule out the possibility that thought control strategies are reactions to reexperiencing and avoidance symptoms, nor that these are associated with other causal factors. We based our theoretical model on prior experimental findings that randomly assigning participants with PTSD to engage in thought suppression increases intrusive memories of trauma-related stimuli (Amstadter & Vernon, 2006; Shipherd & Beck, 2005), and longitudinal studies indicating that worry and thought suppression prospectively predict the maintenance of PTSD symptoms over time (Ehlers et al., 1998; Holeva et al, 2001). The reverse meditational models help to support the proposed direction of effects, as we found no evidence that attentional interference mediates the relationship between thought control and PTSD symptoms. However, future research using longitudinal data to test these meditational models is warranted. Another limitation of the current study is the use of a self-report measure of PTSD. The lack of a structured clinical interview limits the generalizability of our findings to individuals diagnosed with PTSD. However, participants were recruited from a clinical setting and half of our sample reported PTSD symptoms in the clinically significant range, offering support for the relevance of these findings to clinical populations. Because our sample was limited to male Vietnam-era veterans, it would be important to replicate these findings in women and in other populations of trauma survivors. Strengths of this study include the assessment of attentional interference using a performance-based measure, the inclusion of higher order thought control strategies, and the examination of PTSD symptom clusters in addition to overall symptom severity.
These results extend the existing literature by examining mechanisms of the relationship between attentional interference and PTSD. Specifically, the results provide support for a theoretical model in which difficulty withdrawing attention from threat leads to maladaptive thought control strategies including suppressing unwanted thoughts, replacing these thoughts with worries about more mundane concerns, and using less social control. Thought suppression was related to higher levels of both reexperiencing and avoidance symptoms, whereas worry was only related to avoidance symptoms. These results suggest that targeting thought control strategies during PTSD treatment could be helpful, especially in addressing reexperiencing and avoidance symptoms. In particular, mindfulness and acceptance-based therapies might be beneficial, with their focus on nonjudgmental awareness and acceptance, rather than suppression, of unwanted thoughts and internal experiences. These findings also point to a relationship between information processing biases, which may occur outside conscious awareness or effortful control, and strategic attempts to control one’s thoughts. The interplay between these processes, and their implications for PTSD and other forms of psychopathology, is an exciting direction for future research.
Acknowledgments
These data were collected as part of a larger study (Pineles, Shipherd, Welch, & Yovel, 2007). Blair E. Wisco was supported by Award Number T32MH019836 from the National Institute of Mental Health. Suzanne L. Pineles was supported by a VA Career Development Award from the Department of Veterans Affairs. Jillian C. Shipherd was supported by grant W81XWH-09-1-0535 from the U.S. Army Medical Research Unit- Europe. Brian P. Marx was supported by grants W81XWH-08-2-0028 and W81XWH-08-2-0100 from the U.S. Army Medical Research and Materiel Command. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Veteran Affairs, National Center for PTSD, National Institute of Mental Health, or the National Institutes of Health.
Footnotes
We ran exploratory analyses examining the relationship between facilitation of attention towards threat and each of the PTSD symptom clusters, to ensure that the null results found by Pineles and colleagues (2007) were not due to a failure to separate out hyperarousal symptoms. Facilitation of attention was not related to any of the symptom clusters, even hyperarousal (βs < .005, ts < 1, ns).
References
- Amir M, Kaplan Z, Efroni R, Levine Y, Benjamin J, Kotler M. Coping styles in post-traumatic stress disorder (PTSD) patients. Personality and Individual Differences. 1997;23:399–405. doi: 10.1016/S0191-8869(97)80005-0. [DOI] [Google Scholar]
- Amir N, Beard C, Burns M, Bomyea J. Attention modification program in individuals with Generalized Anxiety Disorder. Journal of Abnormal Psychology. 2009;118:28–33. doi: 10.1037/a0012589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amstadter AB, Vernon LL. Suppression of neutral and trauma targets: Implications for Posttraumatic Stress Disorder. Journal of Traumatic Stress. 2006;19:517–526. doi: 10.1002/jts.20142. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV-TR. Washington DC: Author; 2000. [Google Scholar]
- Bennett SA, Beck JG, Clapp JD. Understanding the relationship between posttraumatic stress disorder and trauma cognitions: The impact of thought control strategies. Behaviour Research and Therapy. 2009;47:1018–1023. doi: 10.1016/j.brat.2009.07.015. [DOI] [PubMed] [Google Scholar]
- Borkovec TD, Alcaine OM, Behar E. Avoidance theory of worry and generalized anxiety disorder. In: Heimberg CTR, Mennin D, editors. Generalized anxiety disorder: Advances in research and practice. New York, NY: Guilford Press; 2004. pp. 77–108. [Google Scholar]
- Ehlers A, Mayou RA, Bryant B. Psychological predictors of chronic posttraumatic stress disorder after motor vehicle accidents. Journal of Abnormal Psychology. 1998;107:508–519. doi: 10.1037/0021-843X.107.3.508. [DOI] [PubMed] [Google Scholar]
- Forbes D, Creamer M, Biddle D. The validity of the PTSD Checklist as a measure of symptomatic changes in combat-related PTSD. Behaviour Research and Therapy. 2001;39:977–986. doi: 10.1016/S0005-7967(00)00084-X. [DOI] [PubMed] [Google Scholar]
- Hazen RA, Vasey MW, Schmidt NB. Attentional retraining: A randomized clinical trial for pathological worry. Journal of Psychiatric Research. 2009;43:627–633. doi: 10.1016/j.jpsychires.2008.07.004. [DOI] [PubMed] [Google Scholar]
- Holeva V, Tarrier N, Wells A. Prevalence and predictors of Acute Stress Disorder and PTSD following road traffic accidents: Thought control strategies and social support. Behavior Therapy. 2001;32:65–83. doi: 10.1016/S0005-7894(01)80044-7. [DOI] [Google Scholar]
- Kimble MO, Fleming K, Bandy C, Kim J, Zambetti A. Eye tracking and visual attention to threatening stimuli in veterans of the Iraq war. Journal of Anxiety Disorders. 2010;24:293–299. doi: 10.1016/j.janxdis.2009.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krebs G, Hirsch CR, Mathews A. The effect of attention modification with explicit vs. minimal instructions on worry. Behaviour Research and Therapy. 2010;48:251–256. doi: 10.1016/j.brat.2009.10.009. [DOI] [PubMed] [Google Scholar]
- Litz BT, Weathers FW, Monaco V, Herman DS, Wulfson M, Marx B, et al. Attention, arousal, and memory in posttraumatic stress disorder. Journal of Traumatic Stress. 1996;9:497–518. doi: 10.1002/jts.2490090308. [DOI] [PubMed] [Google Scholar]
- MacLeod C, Mathews A. Anxiety and the allocation of attention to threat. The Quarterly Journal of Experimental Psychology A: Human Experimental Psychology. 1988;40:653–670. doi: 10.1080/14640748808402292. [DOI] [PubMed] [Google Scholar]
- Marroquin B. Interpersonal emotion regulation as a mechanism of social support in depression. Clinical Psychology Review. 2011;31:1276–1290. doi: 10.1016/j.cpr.2011.09.005. [DOI] [PubMed] [Google Scholar]
- Muris P, Merckelbach H, Horselenberg R. Individual differences in thought suppression. The White Bear Suppression Inventory: Factor structure, reliability, validity and correlates. Behaviour Research and Therapy. 1996;34:501–513. doi: 10.1016/0005-7967(96)00005-8. [DOI] [PubMed] [Google Scholar]
- Nixon RDV, Cain N, Nehmy T, Seymour M. The influence of thought suppression and cognitive load on intrusions and memory processes following an analogue stressor. Behavior Therapy. 2009;40:368–379. doi: 10.1016/j.beth.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Pineles SL, Shipherd JC, Welch LP, Yovel I. The role of attentional biases in PTSD: Is it interference or facilitation? Behaviour Research and Therapy. 2007;45:1903–1913. doi: 10.1016/j.brat.2006.08.021. [DOI] [PubMed] [Google Scholar]
- Pineles SL, Shipherd JC, Mostoufi SM, Abramowitz SM, Yovel I. Attentional biases in PTSD: More evidence for interference. Behaviour Research and Therapy. 2009;47:1050–1057. doi: 10.1016/j.brat.2009.08.001. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/BRM.40.3.879. [DOI] [PubMed] [Google Scholar]
- Reynolds M, Wells A. The Thought Control Questionnaire - psychometric properties in a clinical sample, and relationships with PTSD and depression. Psychological Medicine. 1999;29:1089–1099. doi: 10.1017/S003329179900104X. [DOI] [PubMed] [Google Scholar]
- Scarpa A, Wilson LC, Wells AO, Patriquin MA, Tanaka A. Thought control strategies as mediators of trauma symptoms in young women with histories of child sexual abuse. Behaviour Research and Therapy. 2009;47:809–813. doi: 10.1016/j.brat.2009.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shipherd JC, Beck JG. The effects of suppressing trauma-related thoughts on women with rape-related posttraumatic stress disorder. Behaviour Research and Therapy. 1999;37(2):99–12. doi: 10.1016/s0005-7967(98)00136-3. [DOI] [PubMed] [Google Scholar]
- Shipherd JC, Beck JG. The role of thought suppression in posttraumatic stress disorder. Behavior Therapy. 2005;36:277–287. doi: 10.1016/S0005-7894(05)80076-0. [DOI] [Google Scholar]
- Wegner DM. Setting free the bears: Escape from thought suppression. American Psychologist. 2011;66:671–680. doi: 10.1037/a0024985. [DOI] [PubMed] [Google Scholar]
- Wegner DM, Zanakos S. Chronic thought suppression. Journal of Personality. 1994;62:615–640. doi: 10.1111/j.1467-6494.1994.tb00311.x. [DOI] [PubMed] [Google Scholar]
- Wells A. Emotional disorders and metacognition: Innovative cognitive therapy. Chichester, UK: Wiley; 2000. [Google Scholar]
- Wells A, Davies MI. The Thought Control Questionnaire: A measure of individual differences in the control of unwanted thoughts. Behaviour Research and Therapy. 1994;32:871–878. doi: 10.1016/0005-7967(94)90168-6. [DOI] [PubMed] [Google Scholar]